Personalized Antibodies for Gastroesophageal Adenocarcinoma (PANGEA): A Phase II Study Evaluating an Individualized Treatment Strategy for Metastatic Disease https://t.co/J9JpKnj1t3
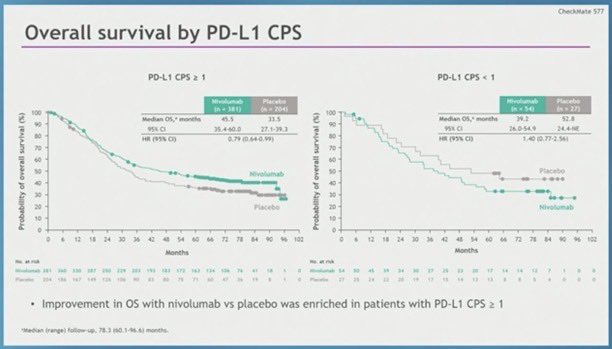
#CM577 there is no benefit (especially CPS0) in CPS low/neg tumors. 44% of pts. And this is not even by histology which would make adenocarcinoma look even worse. Why is this buried in the supplement? & Why would you give this drug for a year to people having no benefit?
@fernandbteich First, #CM577 should be considered obsolete anyway for adenocarcinoma due to #ESOPEC & #MATTERHORN.
But yes, OS in CM577 would be even less impressive if the control arm actually got SOC antiPD1 in first line at recurrence when appropriate (ie PDL1+ and or MSI-H).
@fernandbteich Oh sorry I misunderstood your comment ‘drawing the line’. Yes, rather than requiring proof before doing certain treatments, some do it until it is disproved 10 times before it is stopped, maybe.
#CM577 there is no benefit (especially CPS0) in CPS low/neg tumors. 44% of pts. And this is not even by histology which would make adenocarcinoma look even worse. Why is this buried in the supplement? & Why would you give this drug for a year to people having no benefit?
@fernandbteich Where to draw the line to what is called HER2+ for trastuzumab? Why is the FISH ratio of 2 used, not 1.9 or 2.5? Or Claudin18.2+ for zolbetuximab why is 2+ in 75% of cells used? They are not perfect either, but it is done, which is better than giving those drugs to everybody.
@LizzySmyth1 HR 0.78 NS per the presentation but not in the paper (rather HR 0.99 <12m HR 0.67) >12m)
Where have we seen this tuning fork curve before? ~1/3 pts no diff. CM577
I think it’s a good idea to see the results by PDL1 1, 5, 10: will likely show same thing as all previous studies
@LizzySmyth1 HR 0.78 NS per the presentation but not in the paper (rather HR 0.99 <12m HR 0.67) >12m)
Where have we seen this tuning fork curve before? ~1/3 pts no diff. CM577
I think it’s a good idea to see the results by PDL1 1, 5, 10: will likely show same thing as all previous studies
@LizzySmyth1 🦗🦗
I just read the paper.
Can you please tell me the HR for OS in the ITT full analysis population? I can’t find it!
Any reason you can think of that HR results for OS (not just EFS) of ITT & by PDL1 <1, <5, or <10 aren’t in the publication or the supplement?
📢 FDA ODAC gets it ✅️ for patients
Immune checkpoint inhibitors are a PD-L1 targeted 🎯 therapy in GEA.
No target, no efficacy.
Let's focus on:
➡️ alternative targets (CLD 18.2, FGFR2b, MTAP...)
➡️ overcoming immune evasion (bispecifics, T-cell engagers, CAR-T..)
#TOPGEAR @ESMO2024
- periop chemo +/- RT for #GEA
- no benefit adding RT
- now 6 Phase 3 studies w/o CRT benefit vs or added to neoADJ/ADJ tx for GEA:
- CRITICS, ARTIST1, ARTIST2, neoAEGIS, ESOPEC, TOPGEAR
- SOC is periop #FLOT for all GEA
Time to move away from radiotherapy in operable GEA #ESMO24
TOPGEAR ➡️ no survival benefit when RT added to periop chemo
TOPGEAR + ESOPEC : both great trials with a definitive answer = no more RT
✅Great drugs in development - let's focus on systemic Rx for cure @myESMO
🚨PRODIGE23🚨
Long term results now published!
T3-4 rectal adenocarcinoma
Randomized:
CRT➡️🔪➡️FOLFOX
mFOLFIRINOX ➡️ CRT➡️🔪➡️FOLFOX
✅✅✅Improved OS!!!
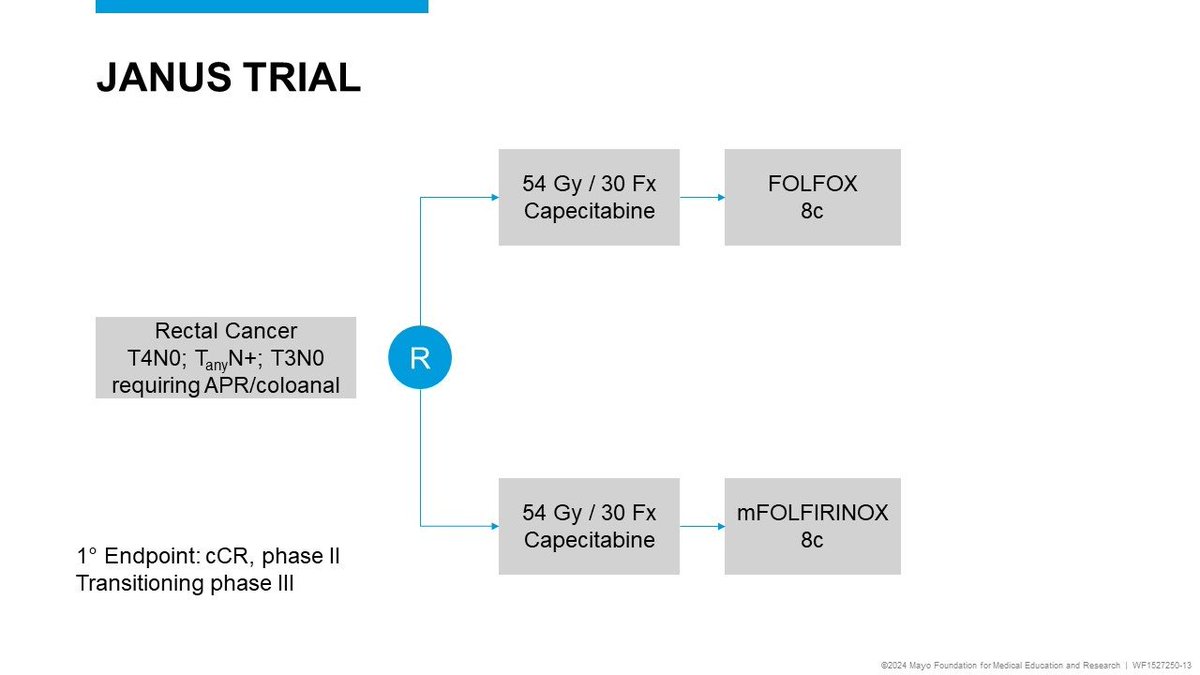
Looking forward to JANUS clarifying if TNT with FOLFIRINOX vs. FOLFOX improves cCR and/or DFS/OS
https://t.co/8As1EhDnup
#SPOTLIGHT#GLOW#Zolbetuximab#Vyloy
"Zolbetuximab BLA resubmitted 5/9/2024, after CRL issued on 1/4/2024 by FDA due to 3rd-party manufacturer deficiencies seen during the pre-license inspection of the facility." Target Action Date: 11/9/2024
https://t.co/nf0AlEEY3J.