An ever-curious Cardiologist 🫀 Always viewing things from different prospectives, in both work and life 🔬 📍Fellow of the Imaging Unit at @hgermanstrias
When a PFO is not really a PFO. 🔍
Closure of a small ASD at the FO with an Occlutech 23/25 mm in a young stroke patient with high RoPE/PASCAL scores. 3D TEE was key for accurate wire crossing in a highly aneurysmal septum 🎯
📍@ Ospedale di Prato Santo Stefano
Implications of small aortic annulus in patients treated with TAVI according to hemodynamic phenotypes of severe aortic stenosis ❣️Last publication of @Doc_Niro 👉https://t.co/PCoYaDLvWE when he was with us @iCorGTrias Small aortic annulus may delay diagnosis and treatment!!
#ACC25#CircSimPub Two-year follow-up results of TRILUMINATE trial indicate significant reduction in tricuspid regurgitation severity & decreased HF hospitalization rates with tricuspid TEER compared to medical therapy. https://t.co/H9ef9xgLtt #AHAJournals@hahn_rt@tavrkapadia
Free until April 1: Late Clinical Outcomes of BEV in Small Annuli (PARTNER Trials)
https://t.co/uESp9e0HlX See also https://t.co/ox3U1DBVVK
https://t.co/bF6UrBY9Fq
https://t.co/fj1b0vKT2K
https://t.co/CnZNK1NOft @JACCJournals@ACCinTouch@PPibarot@djc795@ESC_Journals@escardio
Pleased to share that I am now fully certified in Adult TOE by EACVI!
A sincere thank you to my mentor, @VDelgadoGarcia, and to @EFerrerSistach for their invaluable guidance and support in helping me grow.
Ad maiora!
With the first woman President, Dr Victoria Delgado, a new mandate in the #EACVI journey is just starting.
I feel honored to have the opportunity to work, learn and get inspired by the fantastic personalities of @VDelgadoGarcia and EACVI Past President @s_e_petersen in the next two years.
Victoria is a great leader, superb mentor, cardiologist and researcher. Victoria’s journey has been marked by relentless hard work and passion for #cvimaging, commitment to excellence and to uplift others.
She has incredible metrics for her age (h index >100, citations > 110 k), reflecting worldwide academic impact and exceptional productivity.
I am convinced that the #EACVI is in excellent hands under her leadership
@EACVIPresident
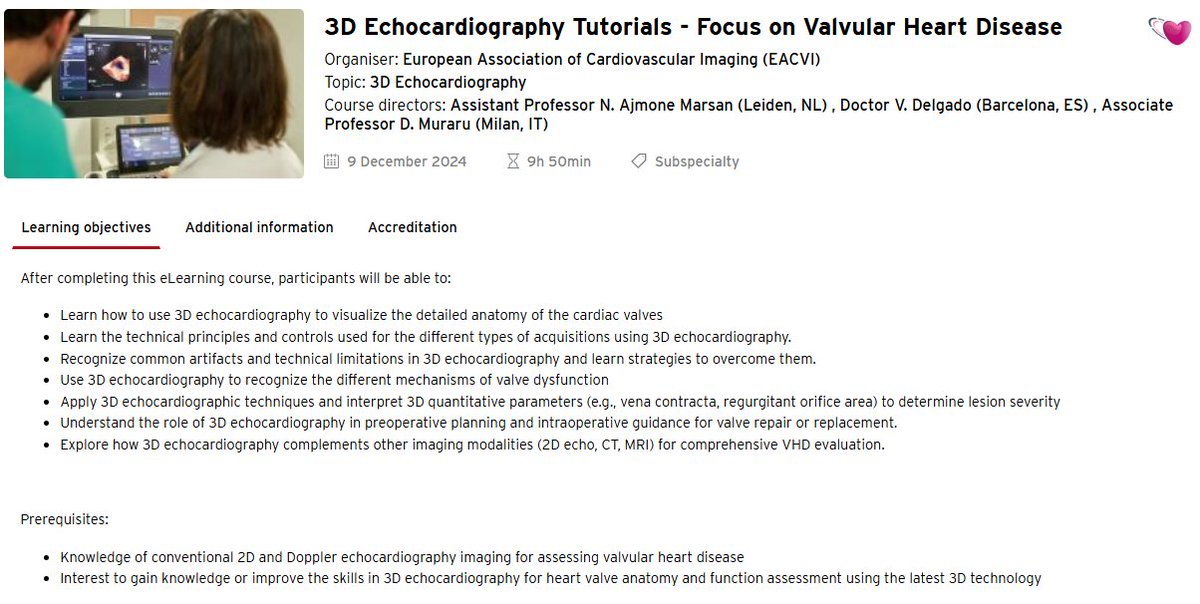
New Tutorials on 3D echocardiography for valvular heart disease 👉 https://t.co/lcKtKhwlP6
💗28 chapters with all you need to know on 3D echo and valvular heart disease
💗9 CME credits when you complete them
You can't miss it!
@denisamuraru@NAjmoneMarsan@EACVIPresident
Must-read review on cardiogenic shock just published in The Lancet:
-> cardiogenic shock is a complex syndrome defined by systemic hypoperfusion and inadequate cardiac output arising from a wide array of underlying causes
->few therapeutic interventions have shown survival benefit
-> results from RCTs support early revascularisation of the culprit vessel in infarct-related cardiogenic shock and temporary circulatory support in selected patients
-> numerous questions remain unanswered, including pharmacotherapy, mechanical circulatory support devices, secondary organ dysfunction, and supportive care
https://t.co/Ap2YOqILCa @TheLancet
It has been an absolute pleasure to have @Doc_Niro with us as fellow of the Cardiovascular imaging department of the @IcorCat at @hgermanstrias
Kind, hard worker and enthusiastic
His achievements, the best reward for us! Good luck in your new endeavor!
#TCT2024 in case you missed it! EARLY TAVR meets primary endpoint driven by Unplanned CV Hospitalization. Also prevents ⬇️ QoL! https://t.co/TtwC0AijM9 @NEJM@TCTMD
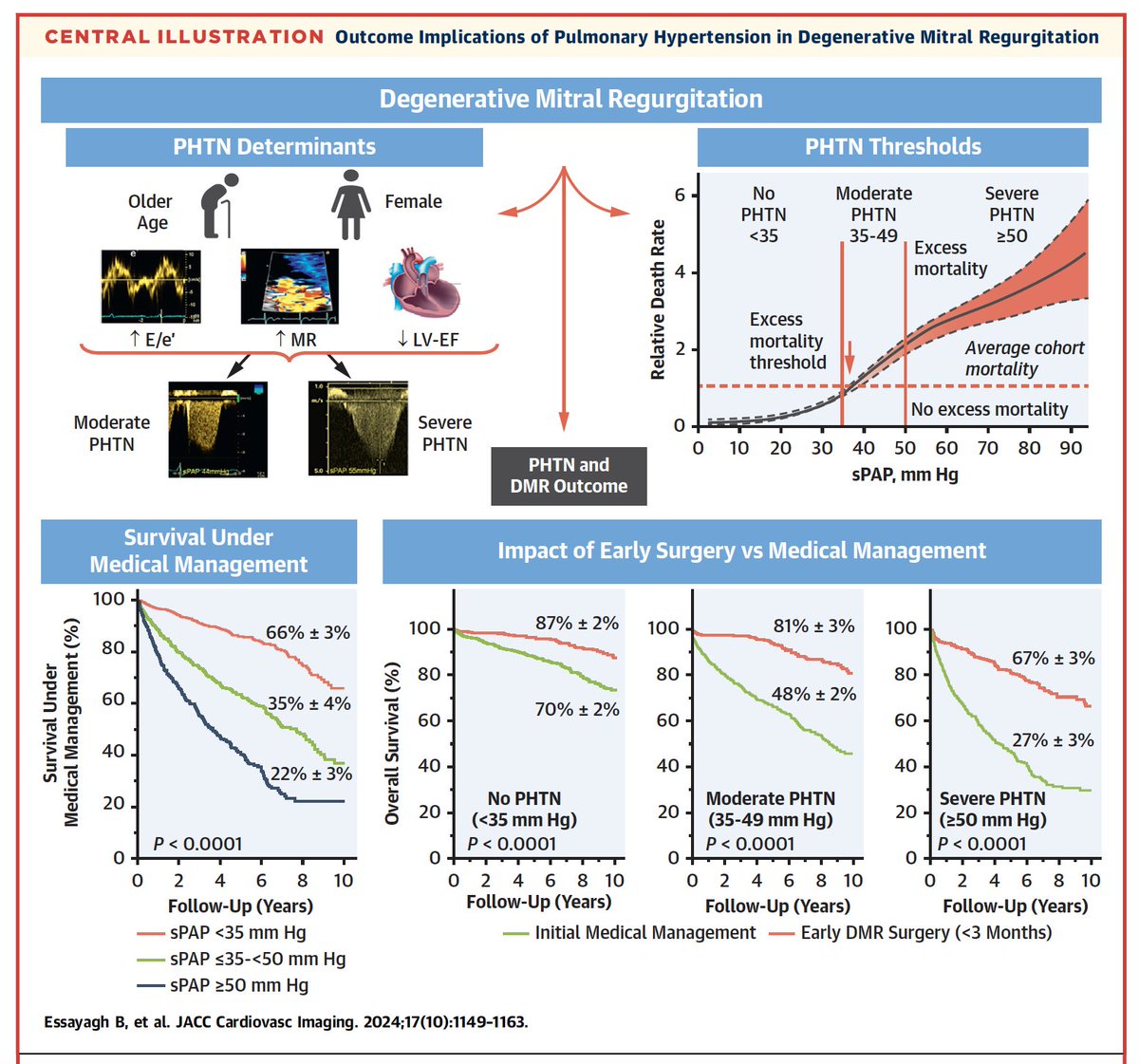
New multicenter registry data in #JACCImaging including > 3700 patients with isolated moderate-to-severe degenerative MR (DMR) on the prognostic impact of pulmonary hypertension (PHTN) measured by Doppler echocardiography.
https://t.co/aKLyFAbSwH
Key messages:
- SPAP response to the significant DMR is heterogeneous: 25% had classic severe PHTN (SPAP ≥ 50 mm Hg), and 30% had moderate PHTN (ie, 35-49 mm Hg).
- excess mortality emerges for SPAP levels much below classical thresholds, with moderate PHTN (35-49 mm Hg) independently associated with excess mortality under medical management, which is eliminated after surgical correction of DMR.
- severe PHTN (SPAP ≥ 50 mm Hg) is associated with more severe excess mortality, which is attenuated but not suppressed after surgical correction of DMR.
- SPAP by Doppler is not just a surrogate for DMR severity, but is incremental to the Doppler EROA, RVol, and clinical characteristics in predicting outcome -> it is pivotal to obtain SPAP during #echofirst throughout the spectrum of DMR severity.
In conclusion, consider moderate PHTN (35-49 mm Hg) in the decision-making for early surgical repair in patients with severe DMR to restore their life expectancy.
Discussing atrial secondary TR with the electrophysiologists during our meeting "ATRIAL FIBRILLATION. CHANGING THE PARADIGM: FROM THE TREATMENT OF ARRHYTHMIA TO THAT OF THE ARRHYTHMIC PATIENT" was great. This condition is not even cited in the latest ESC GL about AF.
#echofirst cheat sheet
How to approach MR?
B4 the exam:
-hemodynamic status
- GMDT in SMR?
- AF?
- Symptoms?
- Need for stress test (after exam)
Step by step approach inside a structured and comprehensive minimum dataset followed by pathology based data set
The complete diagnosis is the result of putting together different information from the echo exam like putting together pieces of a puzzle 🧩
The Guideline Directed Triangle of the Truth:
GDTT
👊how much
👊why
👊structural integrity
1how much?
🫵Volumetric parameters from minimum data set as LVOT SV, total LV SV with its plausibility check by looking at RVOT SV & tot. RV SV
🫵Increased E wave inflow velocity > 1,2 m/s & DVI
🫵Vena contracta
🫵PISA EROA in case it has been suitable to use
2why?
🔑Leaflet position
🔑Jet direction
🔑3D confirming
3 structural integrity
📏LVEDS
🛢️LAVI
LVEF, GLS
“sPAP”