The primary is the source of first progression in >50% of cases of #lungcancer patients, and TRACERx showed us that in 32% of NSCLC the primary polyclonally seeds metastases. In our @IASLC consensus, now in JTO https://t.co/9LzfFi4ICc, makes the case for eradicating it with #radiotherapy. The EGFRm phase III data are the most compelling OS 34.4 vs 26.2 months with TKI+RT. There are still unresolved questions in the non-AGA population. We are opening the phase III PRIME-LUNG trial https://t.co/4J4JsgWu31 @TROGfightcancer@TOGAANZ to answer this question! #radonc
@_ShankarSiva & @Forde_Elizabeth have a dream. And they have beautifully articulated how the Radiotherapy community can work together to make it a reality
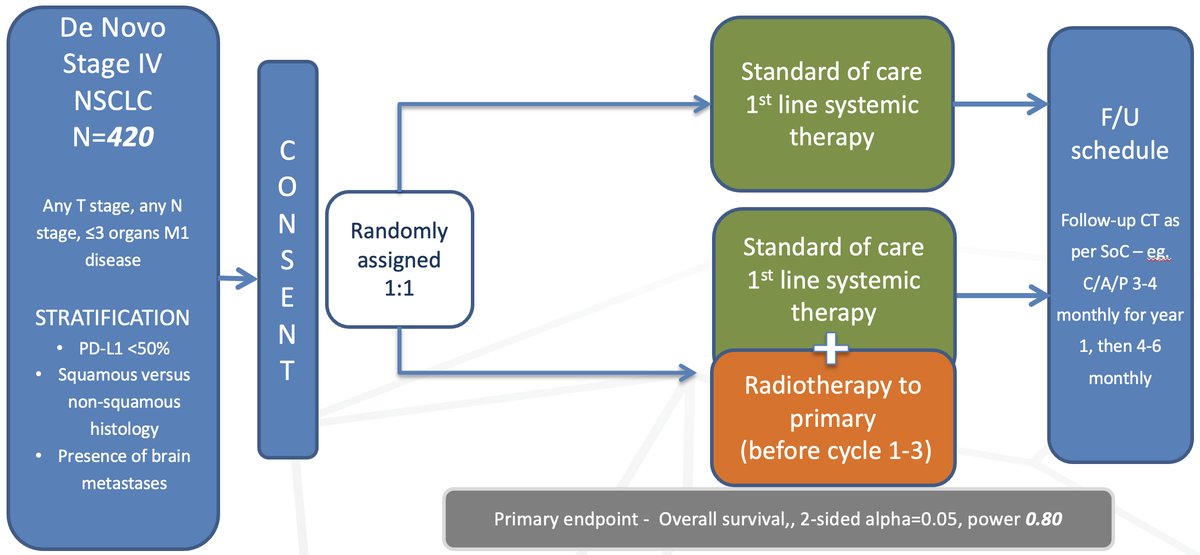
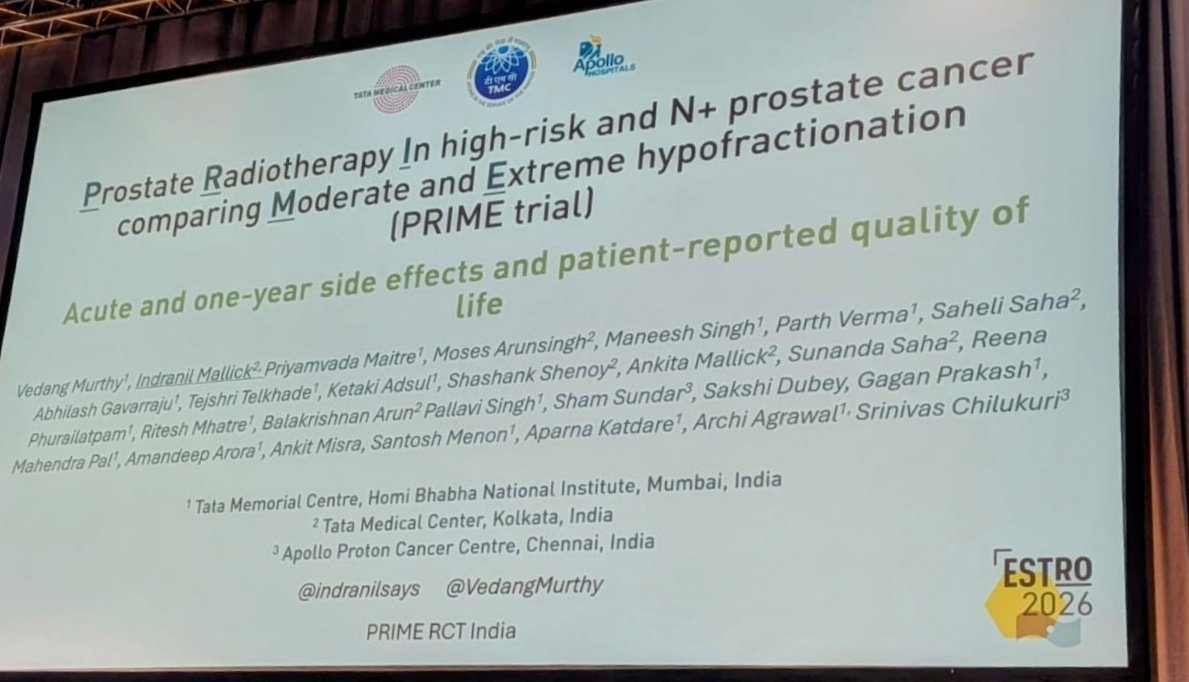
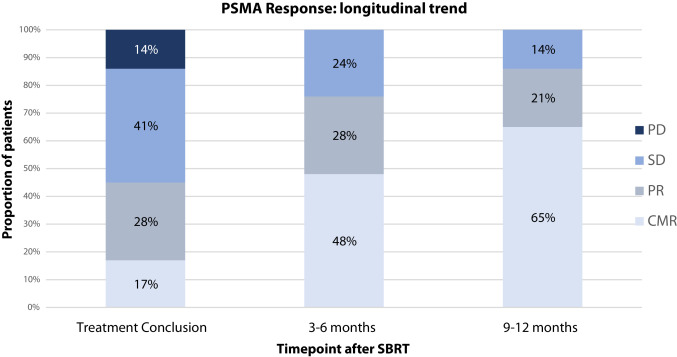
Is SBRT (36.25 Gy/5#) non-inferior to MHRT in high-risk & N+ prostate cancer?
526 patients, 3 centres, mpMRI + PSMA staging, 77% whole-pelvis RT.
Largest RCT in this population. From @TataMemorial@RadOncTMC 🔥
#ESTRO2026
Very proud of my whole team esp @indranilsays for brilliantly presenting the 1y AE data of the largest RCT in HR and N+ CaP.
SBRT is safe! Gr 3 AE very low.
More to follow....
#ESTRO26 - 📣 FASTRACKII final results, median F/U of 5 years. Thank you patients, funders, investigators - #kidneycancer#kcsm
1) 100% Local Control: No local recurrences were observed at 36, 60, or 84 months.
2) 100% Cancer-Specific Survival
3) Grade 3 AEs remain at 10%
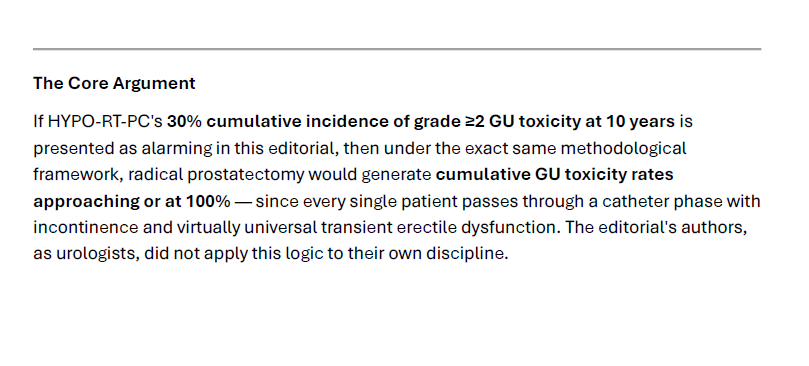
Really? Isn’t an editorial an opinion piece @DriesDeveltere? I hope you realise that if you used the same CTCAE scale for grading cumulative toxicity, you would have 100% G2+ indefinitely with prostatectomy…. Plenty of #radonc talk about these 2 trials cumulative AEs, which you would know if you had bothered to collaborate with one to write this editorial/opinion piece….
@DriesDeveltere@JCO_ASCO@RicBertolo While I agree it is easy to underestimate the burden of toxicity, I doubt cumulative incidence of Gr 2 is the best. A man who needs flomax for a month due to RT in my mind is similar to a man needing a catheter immediately after RP. Should we say RP causes 100% cumulative Gr 3?
Come and join us in the Uro Radiation Oncology Unit at @TataMemorial@RadOncTMC as a Fellow. Post MD/DNB.
You are guaranteed lots of fun! Get in touch if interested!
Come and join us in the Uro Radiation Oncology Unit at @TataMemorial@RadOncTMC as a Fellow. Post MD/DNB.
You are guaranteed lots of fun! Get in touch if interested!
Stereotactic Radiotherapy has transformed our field, and everyone should benefit!
🗺️From Constraints to Confidence: A Roadmap of 'Simple' SBRT 🗺️
Our thoughts in the SBRT special issue of @IJROBP 🥰
Free link⤵️
https://t.co/T2Mfc3pygm
85 years of care, compassion, and commitment.
Since 1941, @TataMemorial has remained dedicated to accessible cancer care, advancing research, and training the next generation of oncology professionals.
Honouring the legacy. Renewing the commitment.
#85YearsOfCare#FoundationDay
Hi everyone! Been a while, but back today with a teaching video on palliative RT for GI cancers.
IMO palliative RT can be v effective, but is underutilized.
Here is 13 min on indications, regimens, common q's re: palliative RT by GI site.
Slides & full video link below 🧵1/5.
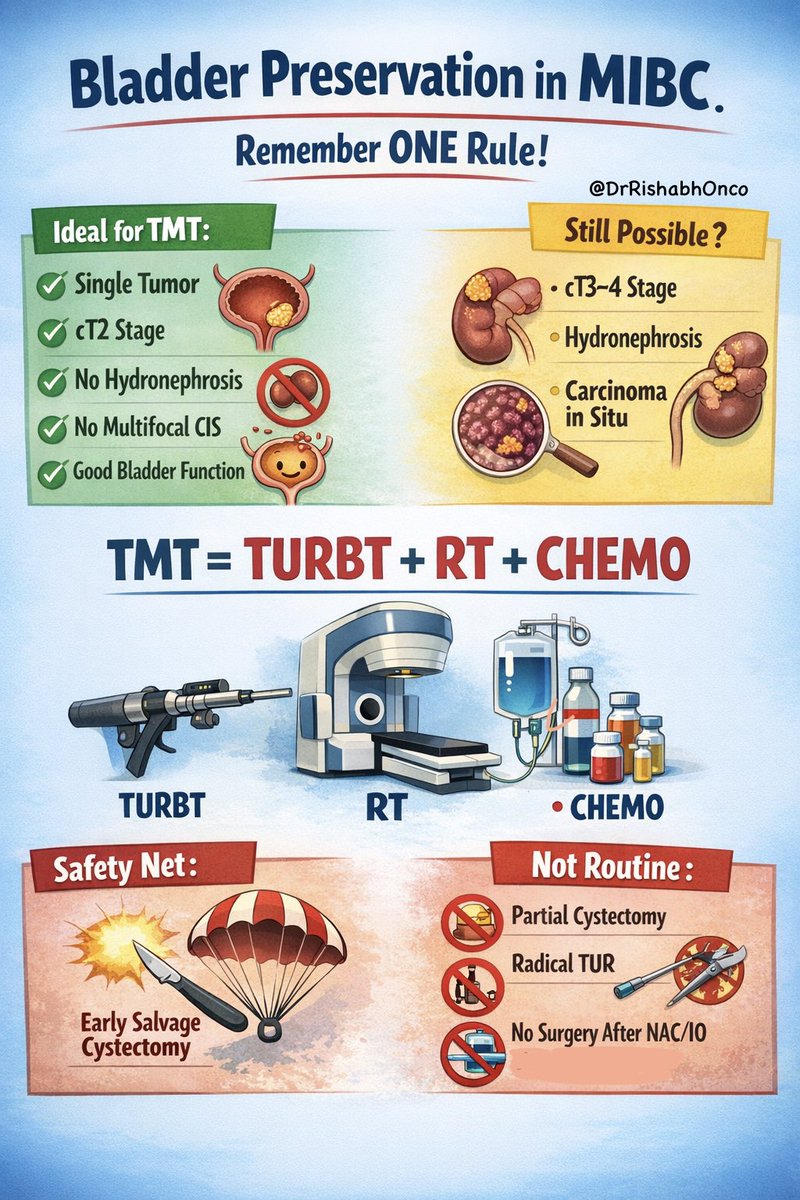
Radical cystectomy is NOT the only standard for MIBC anymore. 🚻🔥
The International Bladder Cancer Group just made it crystal clear in European Urology 📘
If you remember ONE thing, remember this 👇
🧠 TMT = TURBT + RT + Chemo
That’s bladder preservation.
That’s guideline backed.
That’s no longer niche care.
Who wins with TMT 🎯
🟢 Single tumor
🟢 cT2
🟢 No hydronephrosis
🟢 No multifocal CIS
🟢 Good bladder function
Big myth busted ⚠️
cT3–4, CIS, hydronephrosis
👉 Worse prognosis ≠ absolute no
The safety net that makes this work 🛟
If local failure happens
👉 Early salvage cystectomy still cures
What is NOT routine 🚫
❌ Partial cystectomy for most
❌ Radical TUR alone
❌ Skipping local therapy after chemo or IO outside trials
One line takeaway 💡
If you never discuss TMT, you are denying patients a real option.
Would you offer TMT to every eligible MIBC patient ❓
📖 Full paper in comment ⬇️
#BladderCancer #UroOncology #OncoTwitter #MedTwitter #EAU
@OncoAlert@myESMO@ESMO_Open@Uromigos