Interface temp rises during lattice-tip PFA vary by site, with RSPV often blunted. Temp rise correlates with lesion depth—real-time feedback? @johnpowermd@jskoruth#Epeeps@VivekReddyMD@DrKeitaW https://t.co/gaULlUTRBY
A paradox of modern ICD therapy:
An algorithm designed to prevent oversensing may create a transient sensing “blind window” and trigger pacing-induced VF.
Proud to share our case in JACC: Clinical Electrophysiology.
https://t.co/OgOkEN0RHG
@drtopaloglu@ACH_epteam@JACCJournals
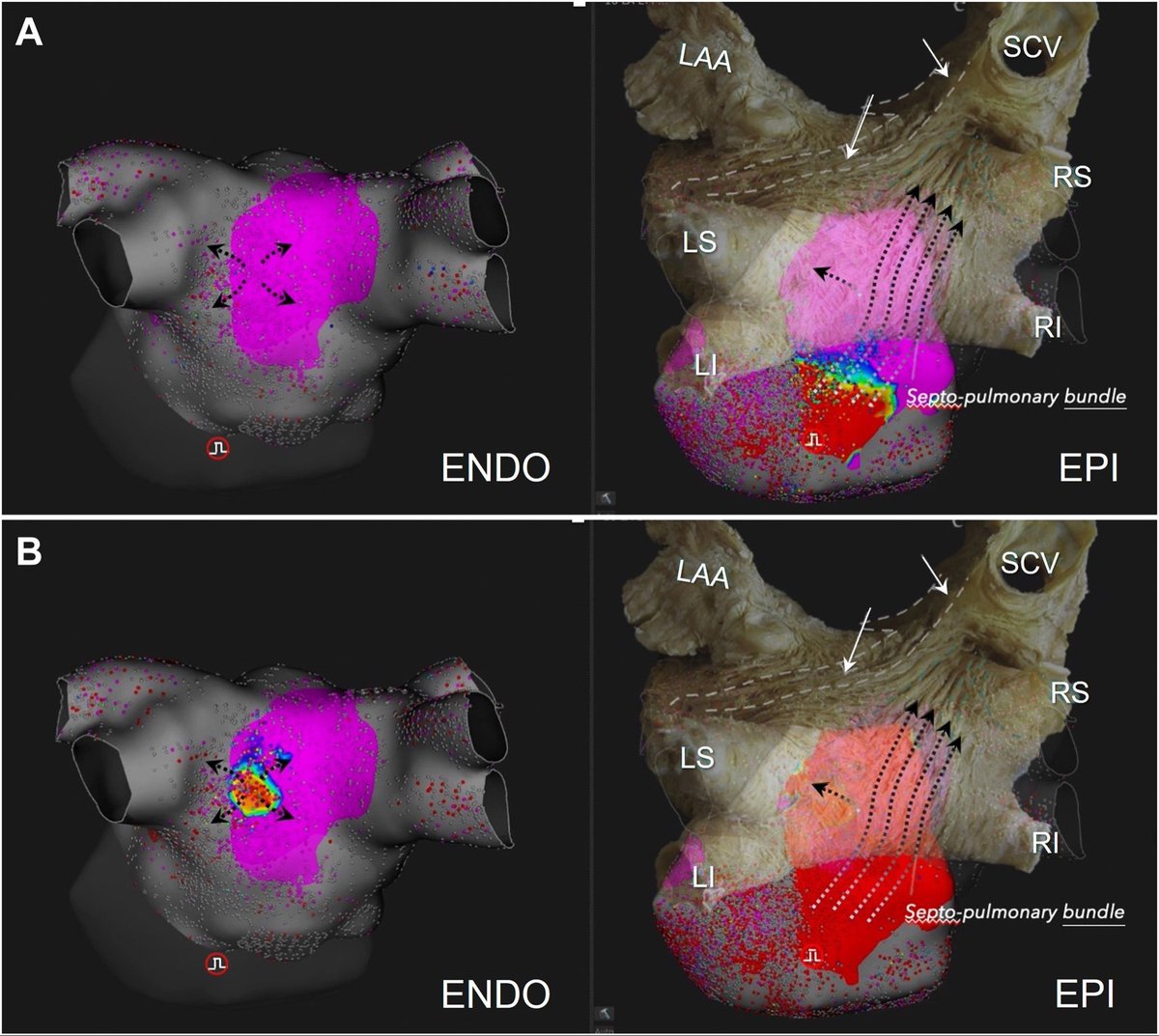
@JACCJournals@DrRoderickTung@davidgzcasal@DamianSanc1955@TomasDatino@AdolfoFontenla Silmultaneous epicardial and endocardial mapping demonstrates clear temporal and spatial dissociation between layers in the posterior wall region. This pattern strongly supports the presence of preferential epicardial or intramural conduction rather than uniform transmural spread
🚨New #FreeRead Review in @JICE_EP
Epicardial Muscle Bundles in Persistent AF: from Overlooked Bystanders to Arrhythmogenic Modulators
🧐📖https://t.co/kPFndaPuX5
by Zheng Zhang, Huilong Qu, Jiayou Zhang & Chun Liang
#EPeeps
Durability of Atrial Linear Lesion Sets Using a Dual-energy Lattice-tip Catheter: Data from Invasive Remapping
@MoritzNies@AndreasMetzner7
https://t.co/hLFNnCbfTR
🚨Latest #FreeRead Article in
@JICE_EP
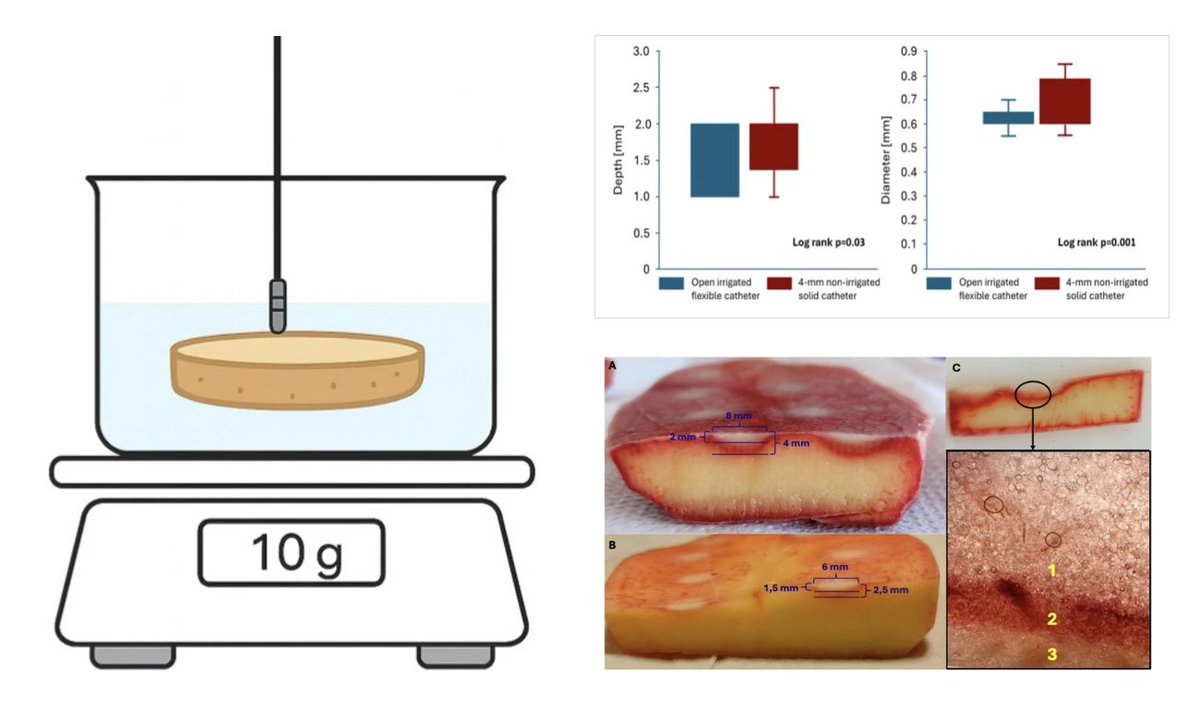
Impact of Catheter Design on Lesion Dimensions during Focal-Bipolar Pulsed Field Ablation: an in Vitro Potato Model Study
🧐📖https://t.co/Xiu9DE0nj8
by Łukasz Zarębski, Agata Wawrzyniak & @ftrae#EPeeps
Bachmann’s bundle architecture, its extensions & clinical implications. Excellent Editorial by @JustinTretterMD & @OCanoPerez highlights framework for BB rightward extensions presented in Part II-III coming soon in JACCCR
https://t.co/Z6aNuV34Uh
https://t.co/N0JlNZnvex
💡"What if a simple gas could make one of #EPeeps' riskiest steps in #VTablation far safer? #CO2#Cardiology"
🧠The latest work from @ClevelandClinic by first author Dr. Koji Higuchi and his team is now featured in RCM!
👉: https://t.co/II1SmEbHeZ
#VentricularTachycardia #EPeeps #VTablation #CO2 #Cardiology #HeartRhythm #CardiacElectrophysiology #CatheterAblation #CardioTwitter #InterventionalCardiology #MedicalResearch #ClevelandClinic
Ventricular pre-excitation is seen in 10–30% of Ebstein anomaly patients, but atriofascicular pathways (<3% of APs) may lack overt signs. As Cone repairs shift to younger ages, awareness of these pathways is key for surgical planning. #JECG#NewOnline
https://t.co/m0ac4SmOK6
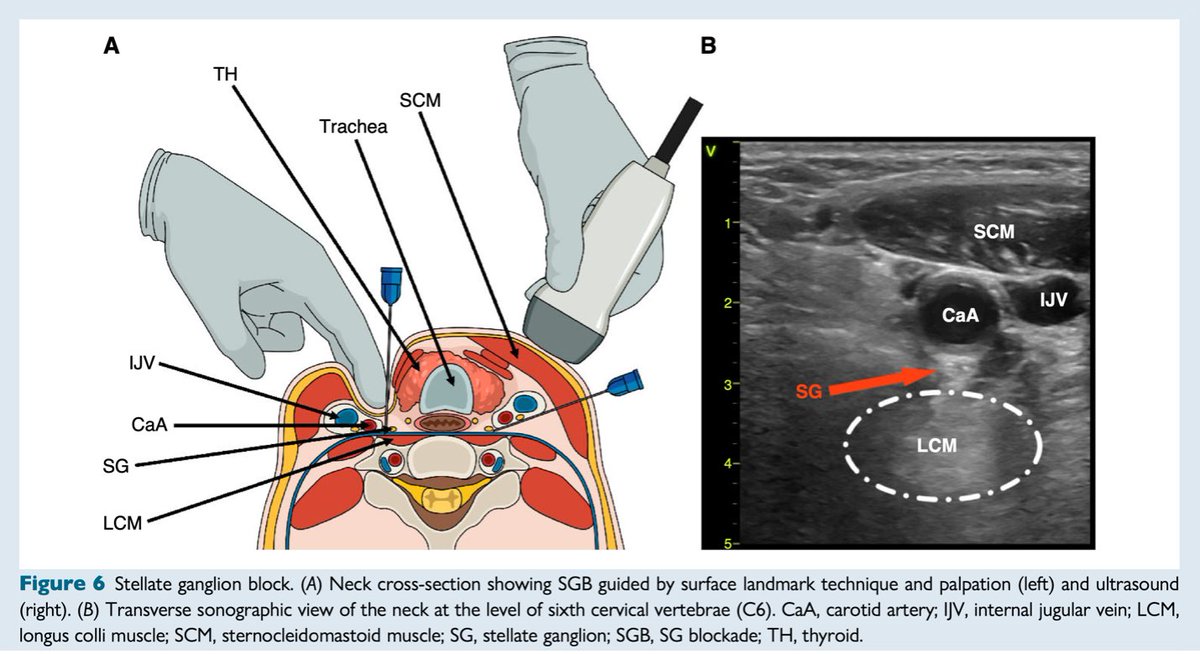
#EHRAtopicweek on electrical storm⚡
What to do when amiodarone and propranolol fail and catheter ablation is not feasible? Stellate ganglion block may be helpful.
Read more #Europace
https://t.co/gLhrxbQX3M
@EuropaceEIC
📢 Focus Issue on PFA interaction with CIED @hrs_journal@HRSonline#EPeeps
➡️ PFA offers myocardial selectivity, procedural efficiency, and an encouraging early safety profile; ➡️PFA interaction with existing intracardiac hardware—remains incompletely understood.
*⃣The May 2026 issue brings together several important real-world observations demonstrating that PFA energy fields can interact with leads, coils, and device circuitry in clinically meaningful ways, underscoring the need for heightened procedural awareness.
🧵below
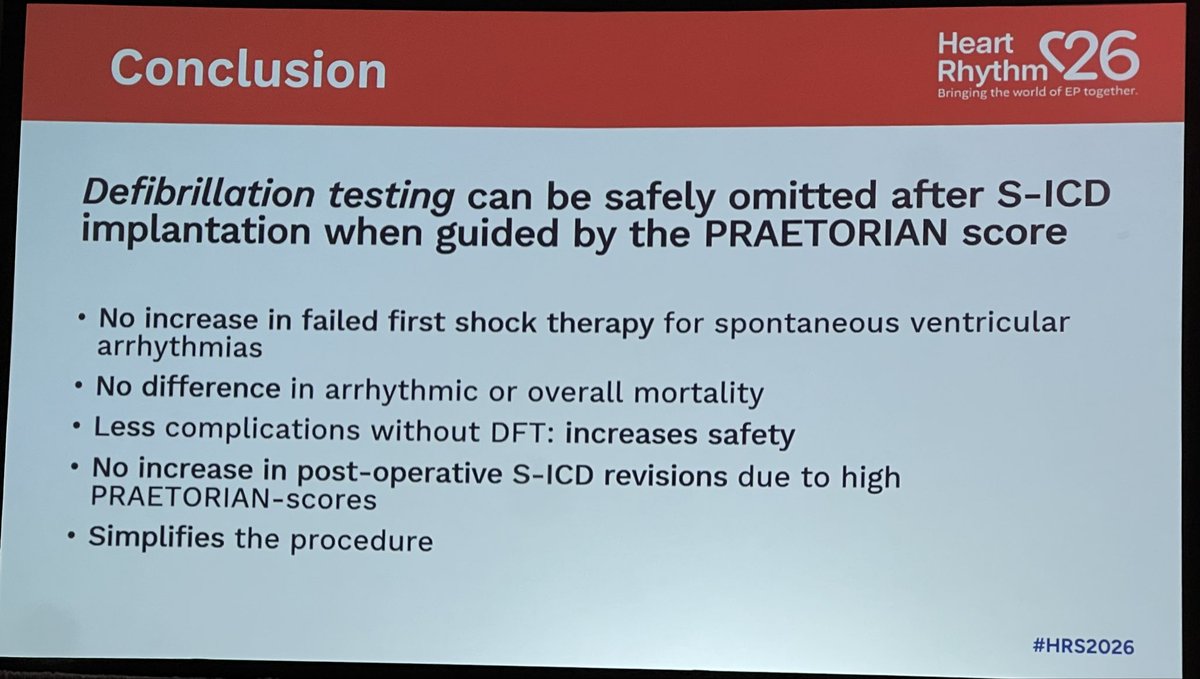
Late-breaker PRAETORIAN-DFT Trial on #HRS2026 by Reinould Knops:
❗️Use of PRAETORIAN Score in non-inferior to DFT Test❗️
➡️no difference in failed first shocks
➡️no difference in all cause and arrhythmic death
➡️less complications without DFT
@HRSonline
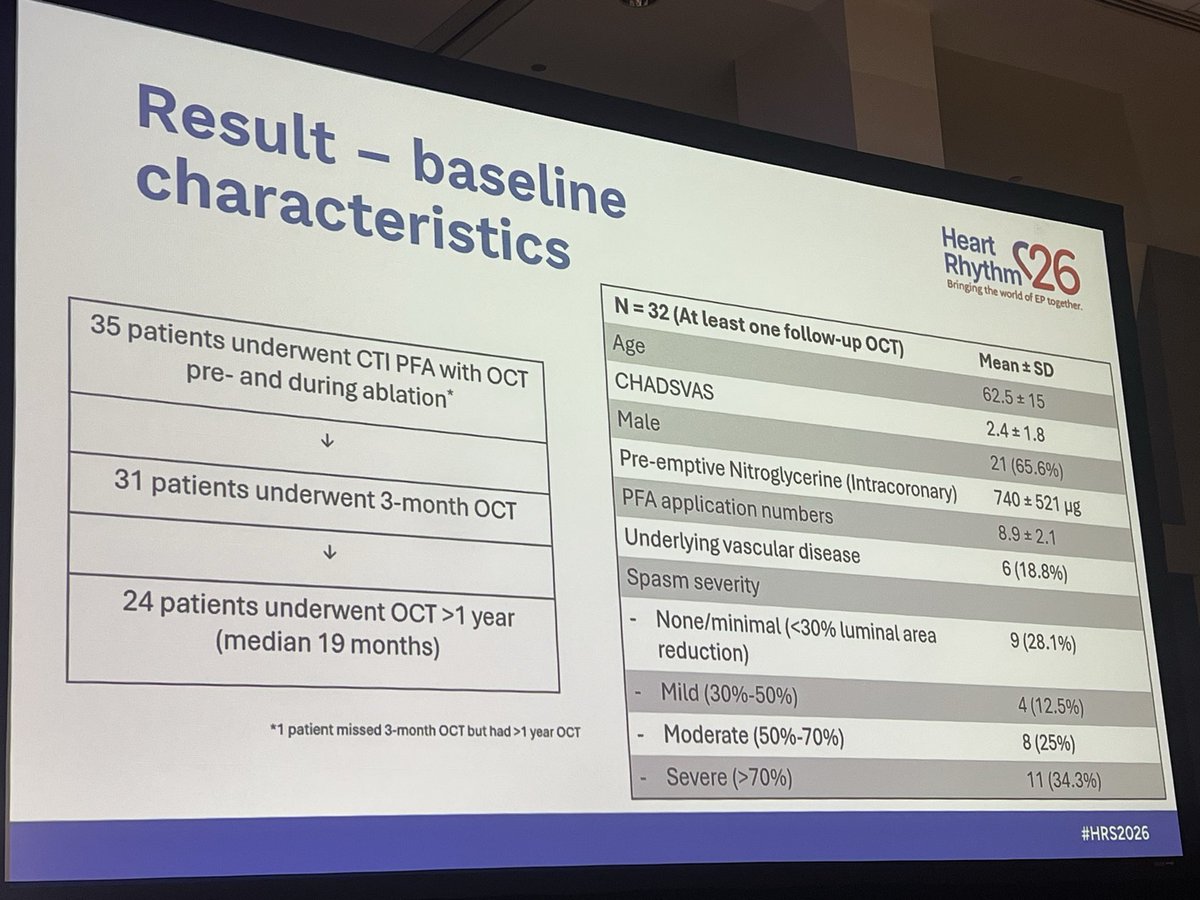
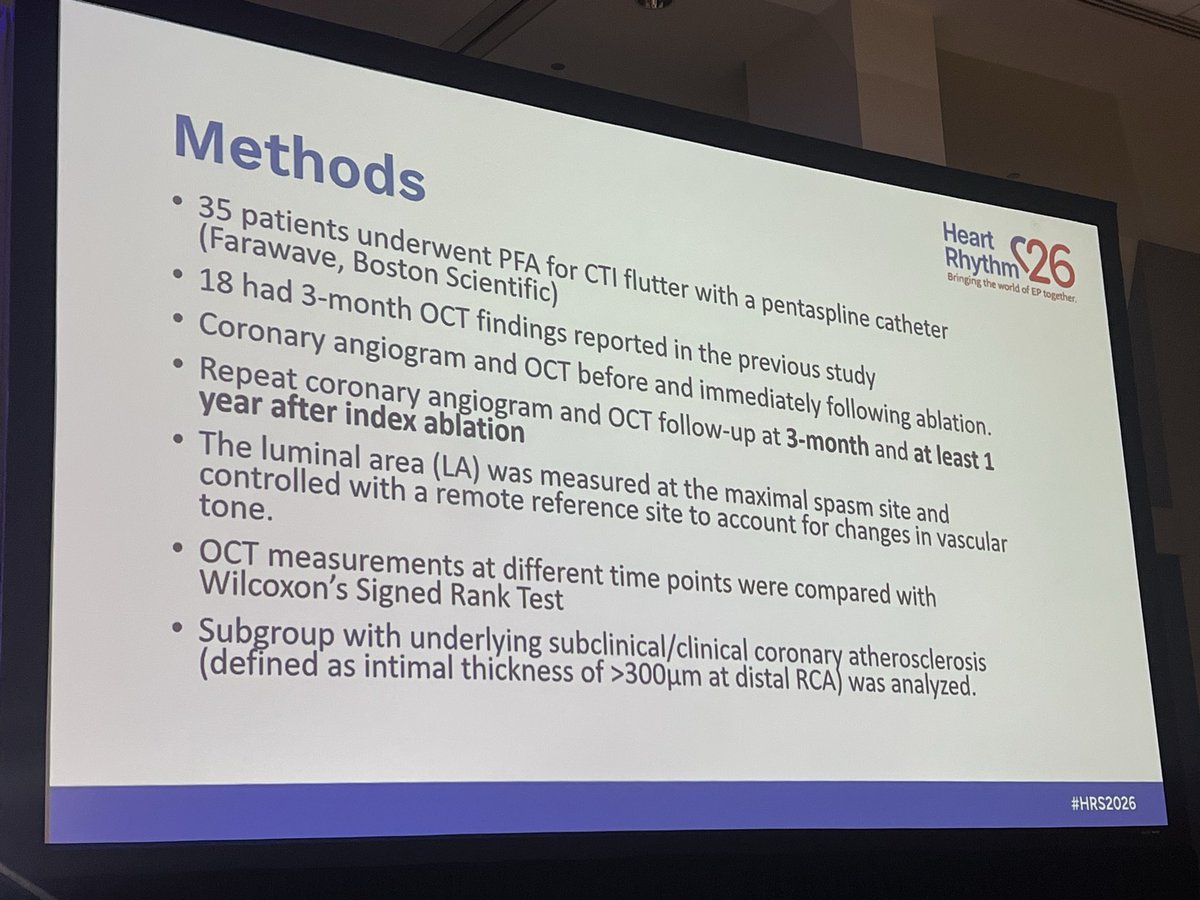
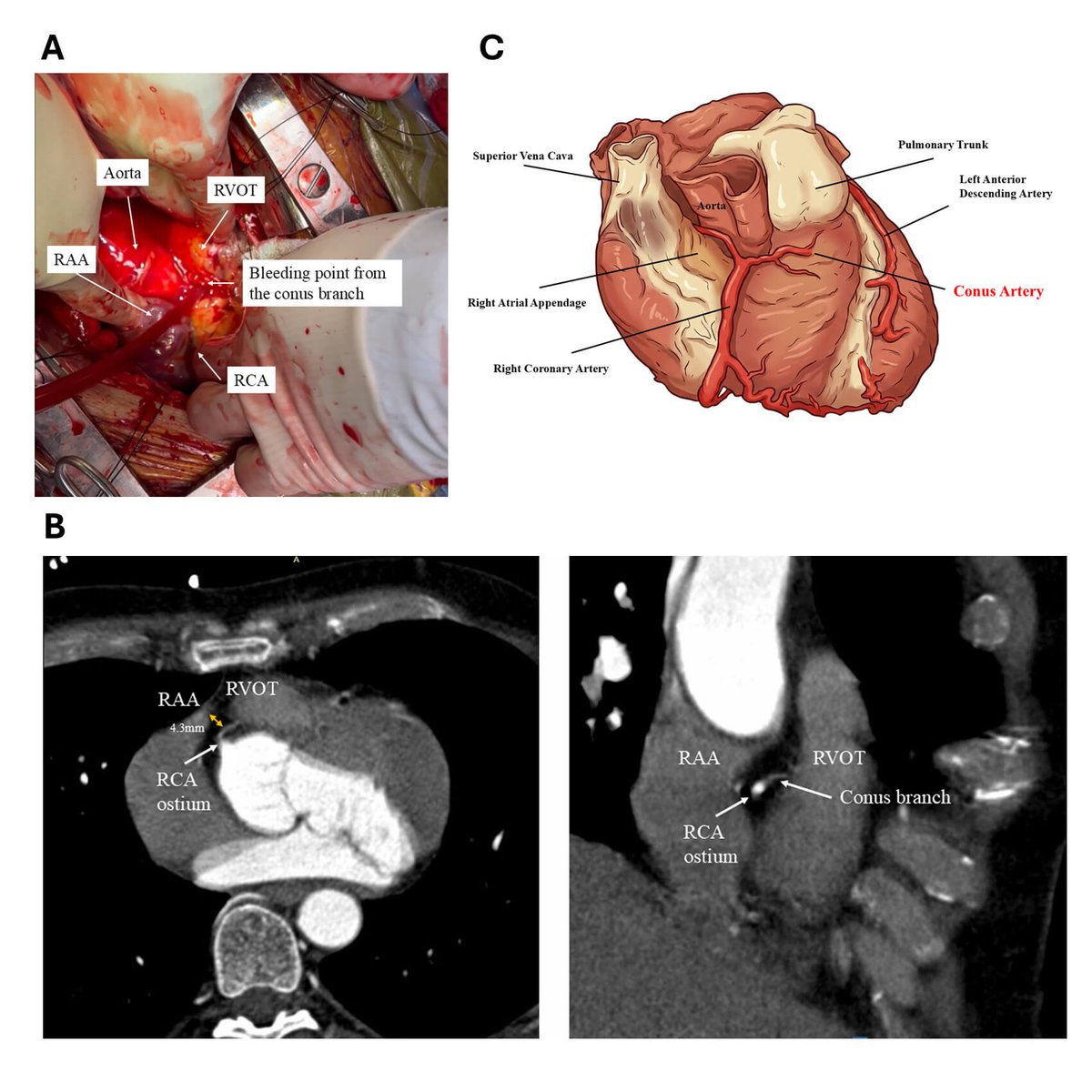
#HRS2026 Long term effect of PFA on coronary arteries: a serial OCT Study
35pts,PFA for CTI with pentaspline catheter
➡️PFA CTI- mild decrease in RCA lumen, no progress between 3 and 19 mo,even in patients with atherosclerosis
➡️Upon 25mo FU none developed coronary ischemia
More than 10 years ago Oussama and I started our journey of investigation, trying to the define the optimal first treatment for patients with atrial fibrillation.
Separately we pursed randomised studies in populations with treatment-naive paroxysmal AF.
Five years ago we presented our RCTs in the paroxysmal AF population, which ended up sitting side by side in the same issue of the New England Journal of Medicine.
https://t.co/DWgHQ2VhiJ
https://t.co/z346xqq0jg
Since then we have been working together to examine the same question of optimal initial therapy, but instead looking at patients with more advanced forms of atrial fibrillation.
Today Oussama presented the results of the AVANT-GUARD study, which definitively demonstrated the value of initial catheter ablation in the treatment naive persistent AF population.
Like EARLY-AF, AVAT GUARD used implantable cardiac monitors to evaluate arrhythmia endpoints
Like EARLY-AF - initial catheter ablation reduced recurrences in AVANT GUARD by about 50%, which was about 25% in absolute terms. To put this another way, only 4 patients need to be treated with ablation to prevent a recurrence of arrhythmia.
However, binary recurrence doesn’t tell the whole story. Because we had loop recorders we were able to assess the time spent in AF (or AF burden). In this regard significantly more patients had none or negligible burden after ablation (<0.1%), with significantly more AAD treated patients having a very high burden (>5%). This is important as AF burden is associated with clinical outcomes such as hospitalisation.
In terms of risk - the rates of any adverse event or serious adverse event were comparable between randomised arms. Highlighting that persistent AF patients with high CHADS-VASc score are high risk irrespective of treatment provided. This is important as we reflect on treatment options as part of shared decision-making.
Congratulations to Oussama for the presentation and leadership, to the co-investigators and study sites for their participation and dedication, and a huge thank you to the Boston Scientific team for their support and commitment to advancing science.
To end, I want to acknowledge and thank Oussama for this shared journey, I’m grateful for our collaboration and friendship, and look forward to what we will do next.
Preexcitación tipo Mahaim. 🫀⚡️
🟥Se debe a la presencia de 2 tipos de vías accesorias:
🔺️Las vías nodo-ventriculares que suelen ser vías anterógradas con conducción muy lenta y decremental, por lo que no suelen registrarse en en ritmo sinusal pero tras una extrasístole auricular pueden desencadenar una taquicardia de QRS ancho antidrómica.
🔺️Las vías fasciculo-ventriculares, mas raras, que en ritmo sinusal suelen tener un patrón de preexcitación en el EKG de: a) PR normal (120-200 ms) y b) complejo QRS ancho con onda delta al principio del mismo y que se caracteriza por no desencadenar taquicardias.
ECG. Vélez, 4ª ed.