Asia-Pacific CardioMetabolic Syndrome Congress (APCMS)にKeynote lecturerとしてご招待頂き講演してきました❗️小保方先生@EchoLab_Gunma と坂本先生@funnybunny81010 と一緒に日本勢🇯🇵として頑張りましたー。最後はboard meeting終わりのKorean Society of Heart Failureの友達も合流してのConrad最上階のバーは最高でした😀
また呼んでもらえるよう頑張ります💪
We talk a lot about HFrEF. But what about HFpEF and HFmrEF?
@mvaduganathan@gcfmd@SJGreene_md@BiykemB@hfcollaboratory@HFA_President@HSkouri
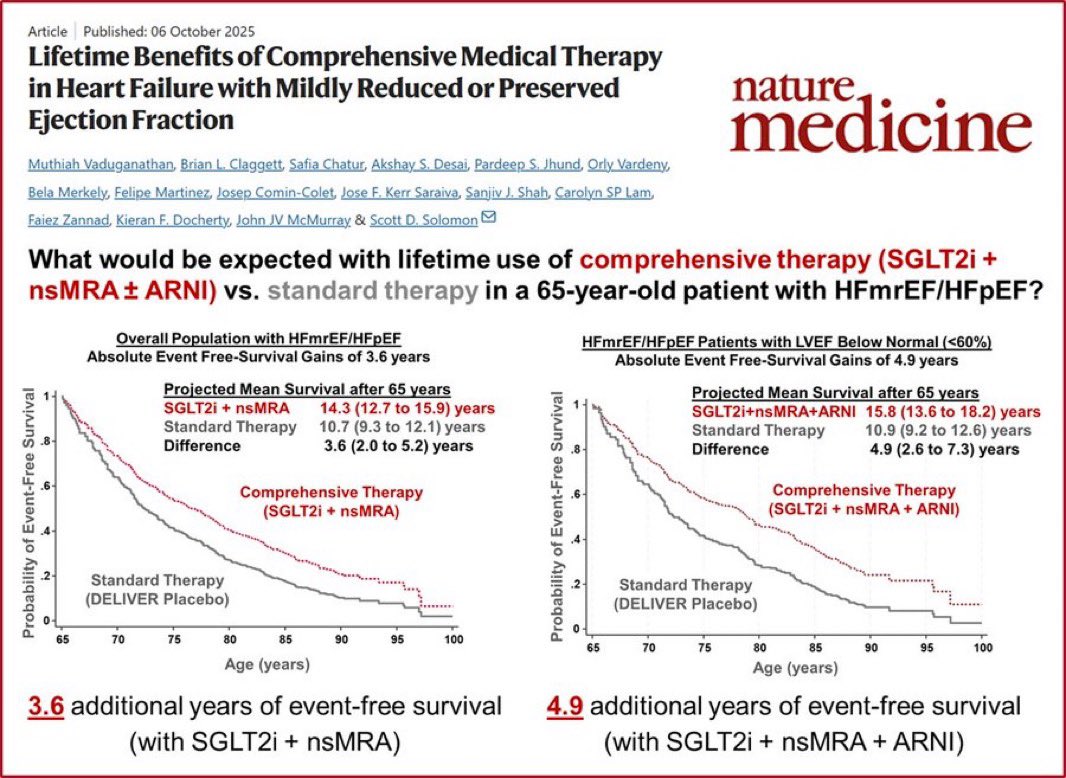
This Nature Medicine study answers the question most patients actually ask: “How much longer will I live?”
For a 65-year-old with HFmrEF/HFpEF:
📌 SGLT2i + nsMRA vs. standard therapy:
→ +3.6 years of event-free survival
📌 SGLT2i + nsMRA + ARNI (LVEF <60%):
→ +4.9 years of event-free survival
Nearly 5 extra years. Not months.
Comprehensive therapy for HFpEF/HFmrEF isn’t optional anymore — it’s the standard.
Vaduganathan et al., Nature Medicine, Oct 2025
#HeartFailure #HFpEF #HFmrEF #SGLT2i #Cardiology #CardioTwitter #MedTwitter
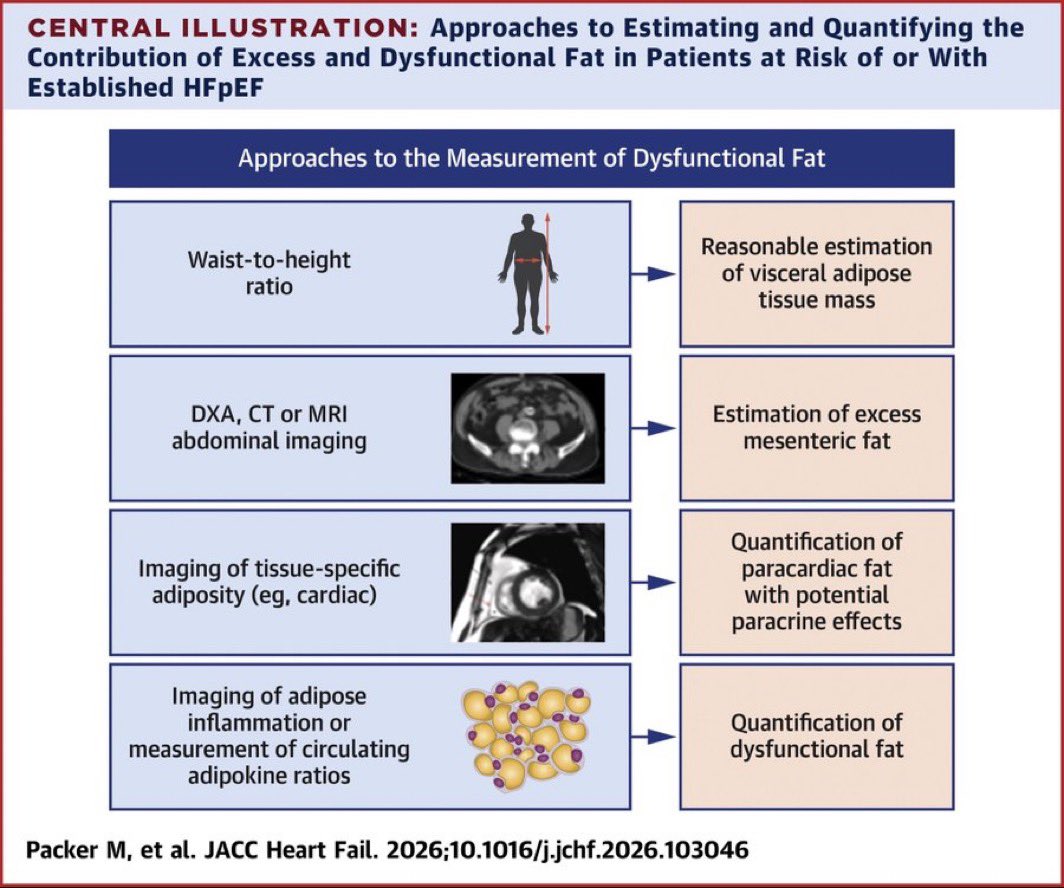
Not all fat is equal — and in HFpEF, the type and location of fat may matter more than total body weight.
New framework from Packer et al. lays out how to actually measure dysfunctional fat — from clinic to imaging to molecular markers 👇
📊 Measuring Dysfunctional Fat in HFpEF:
🔹 Waist-to-height ratio → reasonable proxy for visceral adipose tissue mass (bedside)
🔹 DXA, CT or MRI abdominal imaging → estimates excess mesenteric fat depot (imaging)
🔹 Tissue-specific adiposity imaging (cardiac) → quantifies paracardiac fat with paracrine effects on the myocardium (imaging)
🔹 Adipose inflammation / circulating adipokine ratios → quantifies truly dysfunctional fat — not just excess fat (advanced)
💡 Key distinction: dysfunctional fat ≠ excess fat. Inflamed adipose tissue secretes pro-inflammatory adipokines that directly impair cardiac mechanics — even in patients who aren’t severely obese by BMI alone.
📄 Packer M, et al. JACC Heart Fail. 2026;10.1016/j.jchf.2026.103046
#HFpEF #HeartFailure #Cardiology #Obesity #Adipokines #CardioMet
Can restoring sinus rhythm reverse tricuspid regurgitation? New data says yes — if you succeed. 📁
In 367 AF patients with moderate-severe or severe secondary TR undergoing rhythm control:
• 157 (43%) had NO recurrence → dramatically higher rates of TR improvement to mild or less
• HRs for TR improvement were striking across nearly ALL subgroups
• Female sex showed the strongest effect (HR 11.23)
• Isolated TR etiology also showed large benefit (HR 10.49)
Risk factors for recurrence: older age, chronic/persistent AF, hypertension, no antiarrhythmic meds.
Successful rhythm control = a real shot at TR reversal.
Naser JA, et al. JACC Cardiovasc Imaging. 2026 👇
https://t.co/1Lcfysrkvi
#TricuspidRegurgitation #SecondaryTR #AtrialFibrillation #AFib #RhythmControl
🫀 How do you diagnose HFpEF in 2026? The H₂FPEF score guides the way.
Diagnostic algorithm based on HF probability:
🟢 Low Probability
→ No further testing
🟡 Intermediate Probability
→ Comprehensive Echocardiography
🔴 High Probability
→ Comprehensive Echocardiography
After Echo:
✅ Diagnostic Study → HFpEF confirmed or excluded
⚠️ Nondiagnostic / Equivocal → Diastolic Stress Testing
Key takeaway: Don’t stop at the H₂FPEF score alone — echo is central, and stress testing resolves the gray zone.
Rahi W, et al. JACC Cardiovasc Imaging. 2026;19(2):166–174.
#HFpEF #HeartFailure #Cardiology #Echocardiography #H2FPEF #MedTwitter #JACCImaging