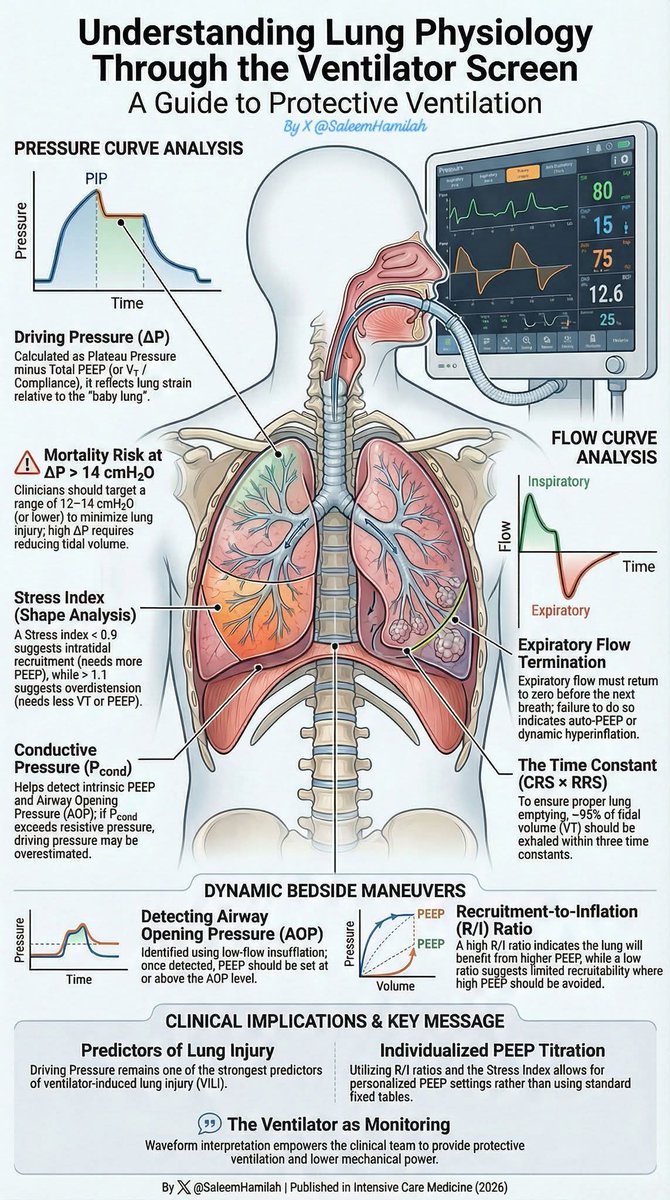
Understanding Lung Physiology Through the Ventilator Screen
💡 The ventilator screen is continuous physiological monitoring.
Interpreting pressure and flow curves allows:
🛡 Protective ventilation
🎯 Individualized PEEP
📉 Lower mechanical power
🫁 Reduced risk of VILI
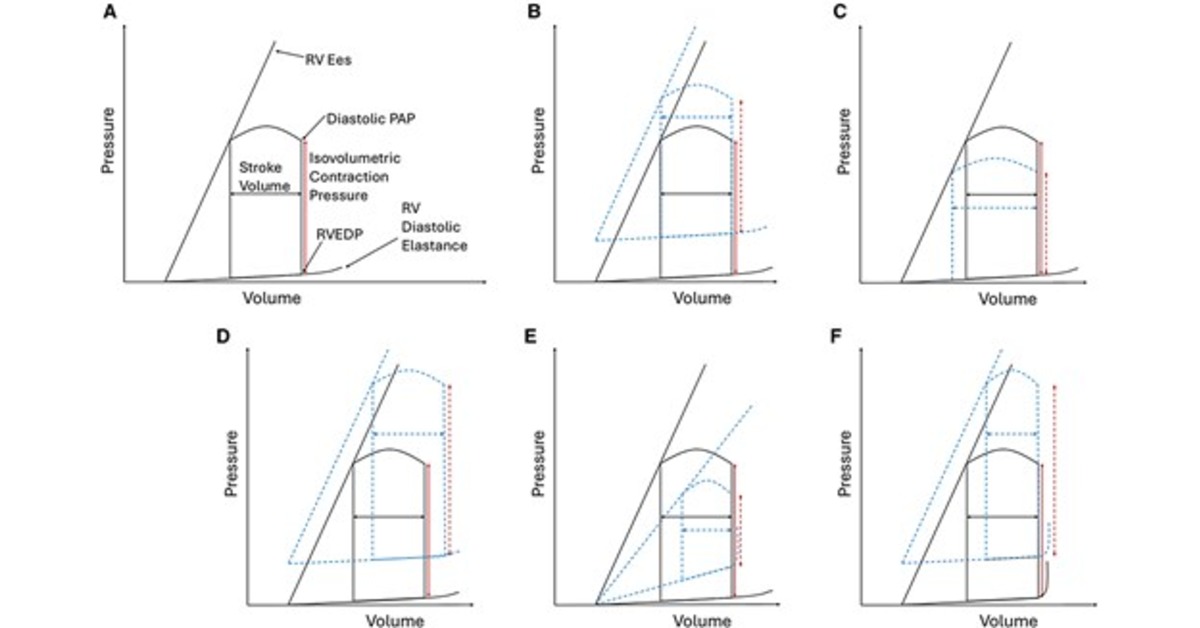
Right Ventricular Hemodynamics in Acute Respiratory Distress Syndrome: Monitoring and Implications for Clinical Management
@atscommunity
🔗 https://t.co/Pd3siasQuC
Expert recommendations for setting and adjusting airway pressure release ventilation based on clinical experience and basic science evidence
CCR Journal Watch
https://t.co/Sp06oA6IDG
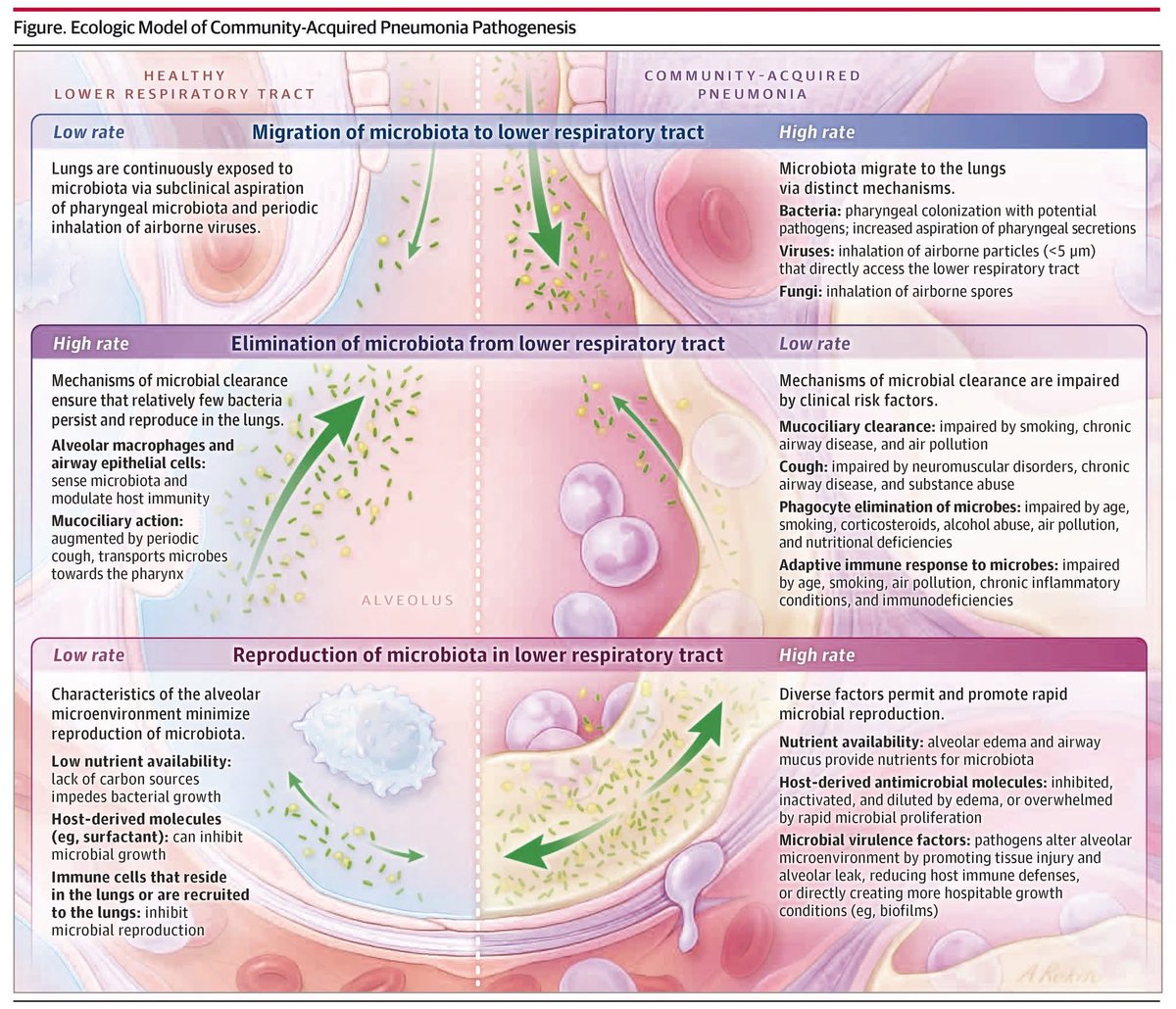
Neumonía adquirida en la comunidad grave: revisión narrativa 🫁🦠
Identifica al grave, antibióticos correctos desde el inicio, desescalar pronto y apoyar la ventilación cuando es necesario.
⏱️Las primeras horas son la diferencia entre alta y mortalidad.
🔗 https://t.co/fmSZQE2RkU
West zones: think in terms of constraints, not targets
West zones are often taught as if capillary pressure is set by a particular pressure.
It’s more accurate to think in terms of boundary conditions.
Zone 3
Downstream constraint = Pv
Pv is a draining pressure
It actively anchors capillary pressure (Pc)
Pc is buffered against changes in Pa
Zone 2
Downstream constraint = Palv
Palv is a collapsing pressure
It does not drain the capillary
It simply prevents Pc from falling below it
So Palv is a floor, but not an anchor.
Why Pa matters in zone 2:
As long as flow is present:
Pc must exceed Palv to keep the vessel open
How far Pc sits above Palv depends on:
• pulmonary arterial pressure (Pa)
• flow
• capillary distension
So Pc is not “set” by Palv.
It is bounded below by Palv and pushed upward by Pa.
That’s why:
• raising Pa raises Pc (eg volume overload)
• raising Palv alone does not raise Pc; it either sets a higher minimum for patency or abolishes flow entirely (in which case Pc and filtration are irrelevant).
Summary:
Zone 3: Pc is anchored to Pv → pressure-buffered
Zone 2: Pc is bounded below by Palv and driven upward by Pa → pressure-vulnerable
In zone 2, alveolar pressure sets a minimum capillary pressure but does not anchor it; capillary pressure floats above that floor in proportion to arterial pressure and flow.
🚨 New @ESICM Guidelines Released!
The 2025 ESICM Guidance on Circulatory Shock & Hemodynamic Monitoring provides 50 expert statements defining what to assess, when to intervene, and how to monitor in adult ICU patients.
Delighted to see IFA Executive Board Members Prof. Xavier Monnet (@Prof_XMonnet) and Prof. @Manu_Malbrain among the contributing authors.
🔹 Key Highlights:
- Emphasis on serial tissue perfusion assessment (CRT, skin temperature, mottling)
- Dynamic predictors of fluid responsiveness (PLR, end-expiratory occlusion)
- Targeted, individualized fluid therapy guided by cardiac output and stroke volume
- Echocardiography as the first-line tool to identify shock type
- Arterial line monitoring for non-responders or those on vasopressors
- Serial intra-abdominal pressure (IAP) monitoring recommended in shock patients at risk of intra-abdominal hypertension
These updated recommendations aim to standardize shock assessment and improve outcomes through physiology-based, multimodal monitoring.
🩺 Monnet X, Messina A, Greco M, et al. Intensive Care Med, 2025
#ESICM #LIVES2025 #CriticalCare #Hemodynamics #Shock #Guidelines #FluidTherapy #Monitoring #Ultrasound
Today's Paper of the Day is:
Pulmonary artery catheterisation
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2025
Diagnostic Criteria of DKA (2024 Consensus Update)
1️⃣ Diagnosis of DKA Needs ALL Three Components
(A) Hyperglycemia or known diabetes + (B) Ketosis + (C) Metabolic Acidosis
Hyperglycemia threshold expanded: ≥200 mg/dL OR prior history of diabetes irrespective of glucose value.
🔷 2️⃣ Euglycemic DKA (EDKA): Don’t Miss It
Seen in ~10% of DKA cases.
Glucose <200 mg/dL, but ketosis + acidosis still present.
Common triggers: SGLT2 inhibitors, pregnancy, fasting, insulin overdose, alcohol, liver failure.
SGLT2 inhibitors are now the leading cause worldwide.
🔷 3️⃣ Ketone Measurement: Beta-Hydroxybutyrate is King
β-Hydroxybutyrate ≥3.0 mmol/L → >90% sensitivity & specificity for DKA.
POCT β-hydroxybutyrate is preferred over urine ketones.
Urine ketones:
Underestimate early (acetoacetate low).
Overestimate later (conversion from β-hydroxybutyrate).
False positives: captopril, valproate.
🔷 4️⃣ Anion Gap: Useful but Not First-Line
High AG (>12) supports DKA, but mixed disorders common.
Normal AG (hyperchloremic) acidosis may appear during recovery—avoid mislabeling as persistent DKA.
🔷 5️⃣ DKA Severity Classification = Guides Location of Care
Mild, Moderate, Severe → Based on pH, bicarbonate, ketones, and mental status.
Helps decide ED vs ICU vs step-down care.
Mild cases may be treated safely with subcutaneous insulin protocols.
🔷 6️⃣ Mild DKA: New Opportunity for Non-ICU Management
Subcutaneous rapid-acting insulin every 1–2 hours is now accepted in selected cases.
Reduces ICU burden and improves patient flow.
🔷 7️⃣ Beware Hyperchloremic Acidosis After Treatment
Caused by saline resuscitation + shift from ketoacids to chloride load.
Not DKA recurrence—avoid prolonging insulin infusion unnecessarily.
🔷 8️⃣ In Resource-Limited Settings
If β-hydroxybutyrate unavailable:
Use urine ketones + anion gap + clinical picture.
But recognize limitations in early and late stages.
🔷 9️⃣ Glucose Level Alone Cannot Rule Out or Confirm DKA
Wide glucose variation possible at presentation.
Diagnosis must rest on ketosis + acidosis.
🔷 🔟 SGLT2i-Associated DKA: Key Red Flags
Often euglycemic—the biggest diagnostic pitfall.
Smell of ketosis, nausea, abdominal pain, tachypnea → Check β-hydroxybutyrate immediately.
Temporarily discontinue SGLT2i during:
Surgery
Fasting
Acute illness
Low-carbohydrate diets
Bonus CME Pearl
🟦 Always Reassess Mental Status
Altered sensorium correlates more with severity than with glucose level.
Early marker of severe DKA → ICU referral.
https://t.co/nnEdFolyj1
Here is the list of some of the advanced airway fellowships available across the globe and open to candidates from outside the institution.
Please feel free to DM us with the details of any other fellowship programmes that are available out there and we can add to the list.
1. University of Michigan Medical School
One year-starting in July
https://t.co/82JrR8GZUB
2. Hamad Medical Centre Doha
One year -starting in September
https://t.co/gKuDAYemK7
3. Mount Senai Hospital, Toronto
One year (Jan/Feb and July/August start)
https://t.co/D9P4W0DxpR
4. Guildford, UK
One year starting in February and August
Application via NHS Jobs website
5. Stanford University Medical Centre
One year with flexible start dates
https://t.co/uJwCL0R4jA
6. Fudan University Eye and ENT hospital, Shanghai, China
3-6 months, rolling application dates.
https://t.co/Pe9I9ms3Po
7. Toronto General Hospital
One year starting in July
https://t.co/w5GHsRr7HJ
8. AIDAA Airway Fellowship, Vadodara, India
3-6months
https://t.co/JdtycGSTXQ
9. St John's Hospital, NHS Lothian, Scotland, UK
April intake.
Application via NHS Jobs website https://t.co/61C8zwxFjI
[email protected]
10. St.James Hospital, Dublin, Ireland
July intake
https://t.co/yoHTwphT3f
@dasresidents@EAMSAirway@Midlandsairway@AirwayHub@AS_Kochi@SafeAirway@ScotAirwayGroup
This is jugular venous distension (JVD) seen with #POCUS. But how can we quantify it at the bedside?
Using the Istrail Method described in The POCUS Textbook, we can estimate the actual right atrial pressure to within about 3 mmHg.
#foamed#meded#Medtwitter#cardiotwitter@nephrop@IM_Crit_@pocuspeek
🧵 THE ULTIMATE VASOPRESSOR + INOTROPE ICU MASTERCLASS
🚨 Shock kills fast. Choosing the wrong pressor kills faster.
Choosing the right one saves a life instantly.
This is the thread every resident, intern and ICU doctor should read today.
#MedTwitter#CriticalCare#FOAMed
🧵 Why you cannot be oedematous and hypovolaemic at steady state
“Puffy but intravascularly dry”?
⚠️The most persistent myth in IV fluid therapy
#FOAMed#physiology#MedX