“Systematic screening for preexisting conditions can identify frailty and inform personalized rehabilitation strategies, improving outcomes and adherence to secondary prevention after CABG.”
https://t.co/uEEimDkWtN
🧠 About 1 in 4 older people in hospital have dementia.
⚠️ But a lot of this has never been diagnosed.
Older people with undiagnosed dementia are frequently admitted to hospital and discharged from hospital without any attempt to make the diagnosis or flag a potential diagnosis and arrange follow-up.
This is a major missed opportunity - to use hospital admission as an opportunity to diagnose dementia where possible, or to flag likely dementia and then arrange follow-up.
In this JAGS paper, Tan and colleagues describe a practical hospital-wide approach combining an electronic health record flag with nurse-administered 4AT and AD8 screening.
Among 11,180 hospital encounters, 83.3% were screened; 18.0% had known dementia, 4.3% screened positive for potential dementia, and 9.0% for cognitive impairment.
That matters because hospital admission is not just a point of acute care, but also an opportunity to identify major cognitive disorders that affect treatment, safety and discharge planning.
The 4AT is useful here. The 4AT is the most validated and used *delirium* tool globally.
But the 4AT also has built-in cognitive tests - so it provides a dual role as a delirium screener but also a tool to assist in detection of dementia.
☑️ This is relevant to the 4Ms - detecting both delirium and dementia/cognitive impairment is necessary - and the 4AT can help with both in the form of one 2-minute tool.
Clinical impact of cardiac magnetic resonance imaging in myocardial infarction with non-obstructive coronary arteries: a prospective multicentre cohort study
https://t.co/G3w2Sq4JJx
Superhuman interpretation AI for medical images, such as mammography and endoscopy, has been proven to improve diagnostic accuracy in multiple randomized trials but mostly not implemented.
But LLMs for clinical decision support have little real world medicine proof, but are getting widely used.
Our new review out today on Testosterone, Creatine, HMB & other anabolic agents in ICU.
❓ Do you use creatine, testosterone, HMB or oxandrolone in your ICU or hospital patients?
🔖 https://t.co/x3lPKByZSt
#ICURehab#FOAMcc#CriticalCare#ICUNutrition@ICUnutrition
A massive Nature study of 27,885 GLP-1 users just dropped some major news about Ozempic and tirzepatide.
Your DNA determines how much weight you lose and how bad the side effects hit.
1 in 3 people see minimal results, and now we know why: (1/9)
The mechanistic link between APOE4 and meningeal lymphatic clearance adds a crucial dimension to the 'drainage' hypothesis of AD. It’s particularly striking how this suggests that Alzheimer's might not just be a proteopathy of production, but a failure of vascular-lymphatic hydraulics. The sex-dimorphism mentioned here could finally explain the disproportionate burden on women beyond just longevity. This shifts the therapeutic horizon: are we looking at the future of 'lymphatic rejuvenation' for APOE4 carriers?
@krishnapatel888 If not “attempted” then EFT cannot be calculated, otherwise if chair rises not “doable” because of weakness or other physical limitations then this component gets a sub-score of 0/2 (when using the EFT important to note reason because differentiates missing data vs. low score)
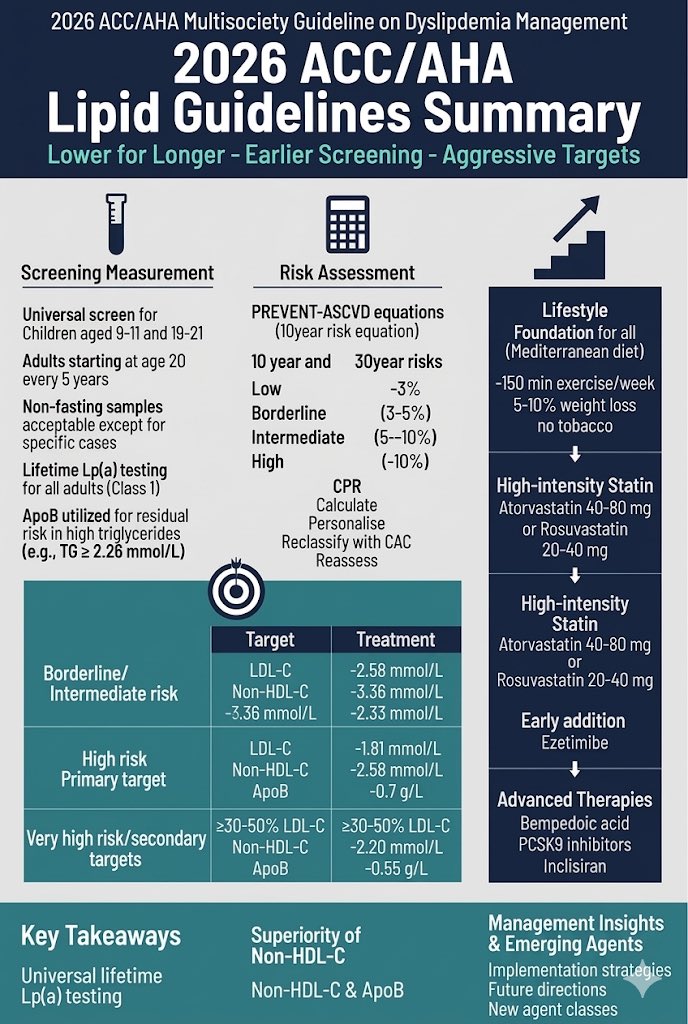
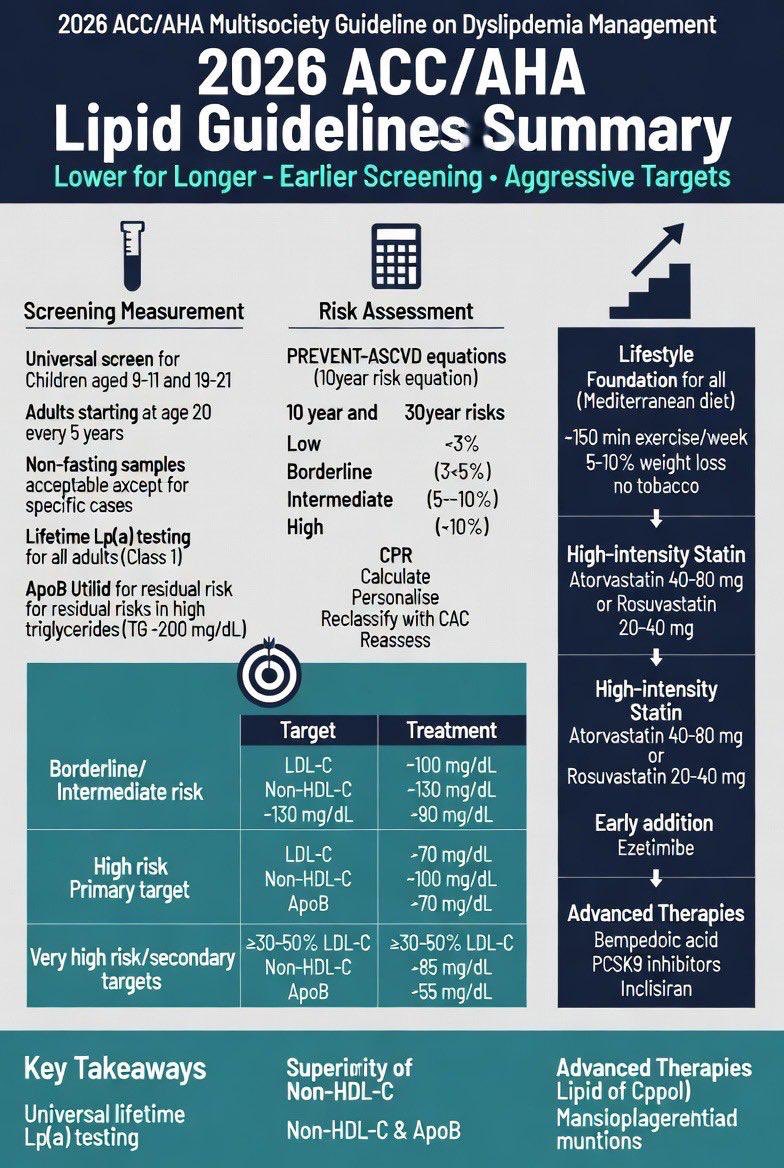
2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
1.Treat dyslipidemia earlier to reduce lifetime exposure to atherogenic lipoproteins; start lifestyle counseling in youth and consider early pharmacotherapy in high-risk individuals (e.g., familial hypercholesterolemia or LDL-C ≥160 mg/dL).
2.Use the PREVENT™ risk equations instead of older models to estimate 10- and 30-year ASCVD risk in adults aged 30–79, applying the CPR approach: Calculate risk, Personalize assessment, and Reclassify if needed (e.g., with CAC).
3.Consider LDL-lowering therapy in primary prevention starting at a 10-year risk of 3–5%, and recommend it more strongly at 5–10%, after clinician–patient discussion.
4.LDL-C and non-HDL-C targets are reintroduced, while maintaining focus on percentage LDL reduction based on ASCVD risk.
5.Apolipoprotein B (ApoB) measurement can help detect residual lipoprotein-related risk, especially in patients with high triglycerides, diabetes, or low LDL-C.
6.Measure Lipoprotein(a) at least once; elevated levels significantly increase ASCVD risk and warrant more intensive LDL-lowering strategies.
7.Coronary artery calcium (CAC) scoring can refine risk assessment and treatment decisions, particularly in men ≥40 and women ≥45 years.
8.LDL-lowering therapy is recommended for adults aged 40–75 with diabetes, CKD stage 3–4, or HIV regardless of LDL-C level.
https://t.co/WEvDXJyoJz secondary prevention, stricter targets are recommended: LDL-C <55 mg/dL and non-HDL-C <85 mg/dL for very high-risk patients.
10.Statins remain the foundation of therapy, particularly in patients with elevated triglycerides; additional therapies may be needed for severe hypertriglyceridemia to prevent pancreatitis.
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@JACCJournals@ACCinTouch@DLBHATTMD@CMichaelGibson@DrMarthaGulati@hvanspall@AndrewJSauer@ESC_Journals@escardio
https://t.co/Sc1gGv1p6y
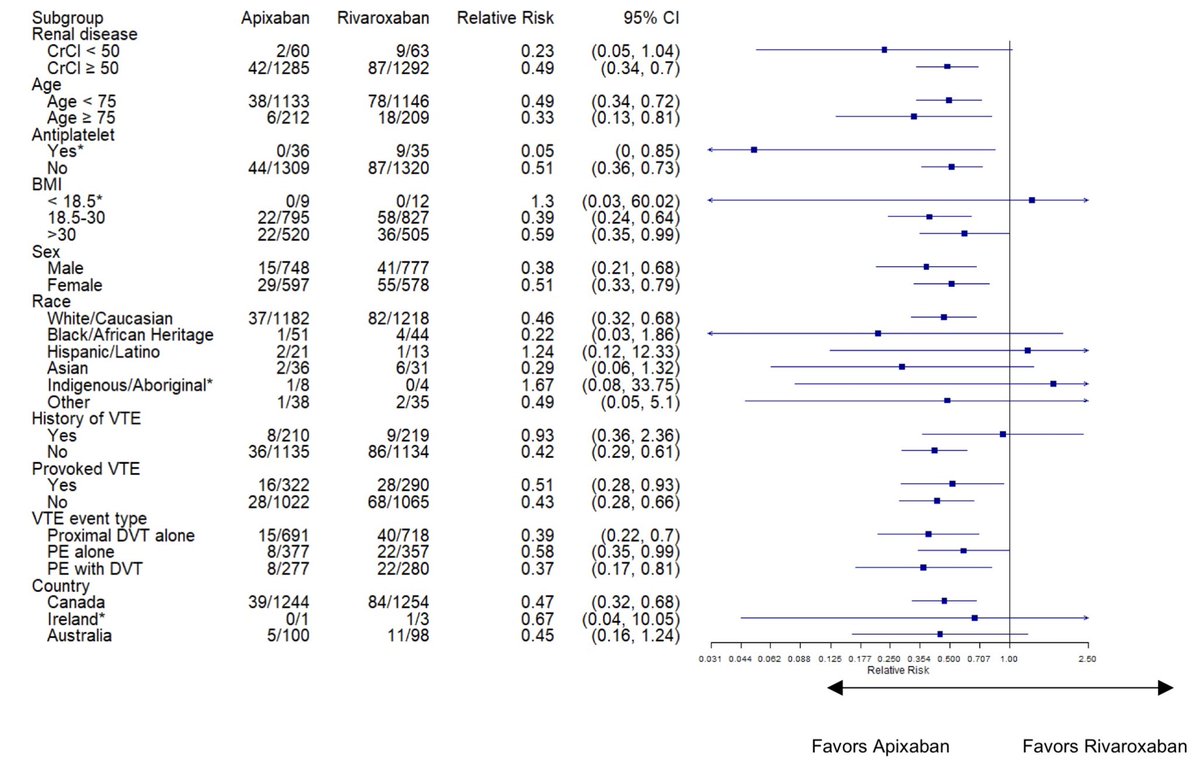
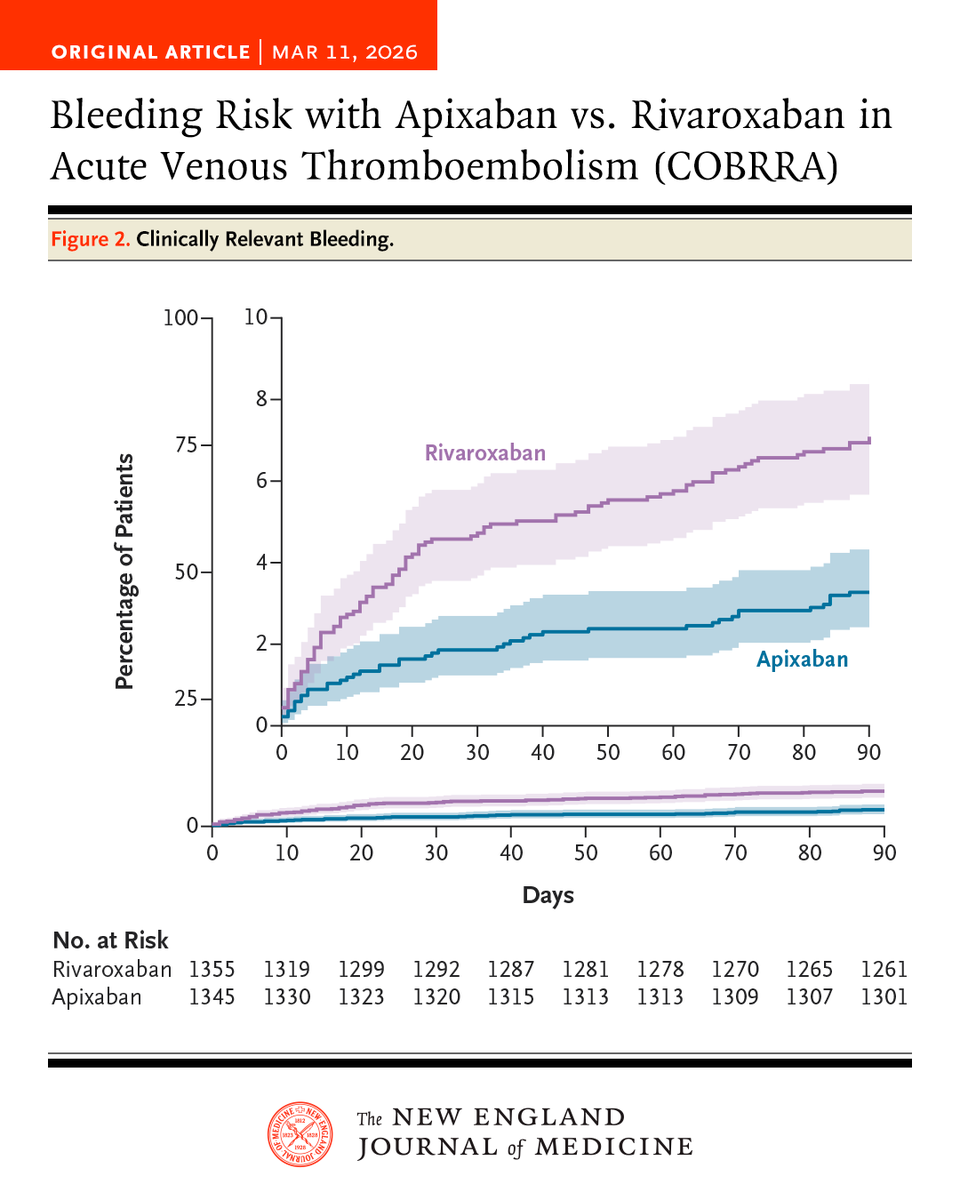
In an international, randomized trial involving patients with acute venous thromboembolism, the risk of clinically relevant bleeding was significantly lower with apixaban than with rivaroxaban during the 3-month treatment period.
Full COBRRA trial results: https://t.co/tvPYrBCWj8
In an international, randomized trial involving patients with acute venous thromboembolism, the risk of clinically relevant bleeding was significantly lower with apixaban than with rivaroxaban during the 3-month treatment period.
Full COBRRA trial results: https://t.co/tvPYrBCWj8
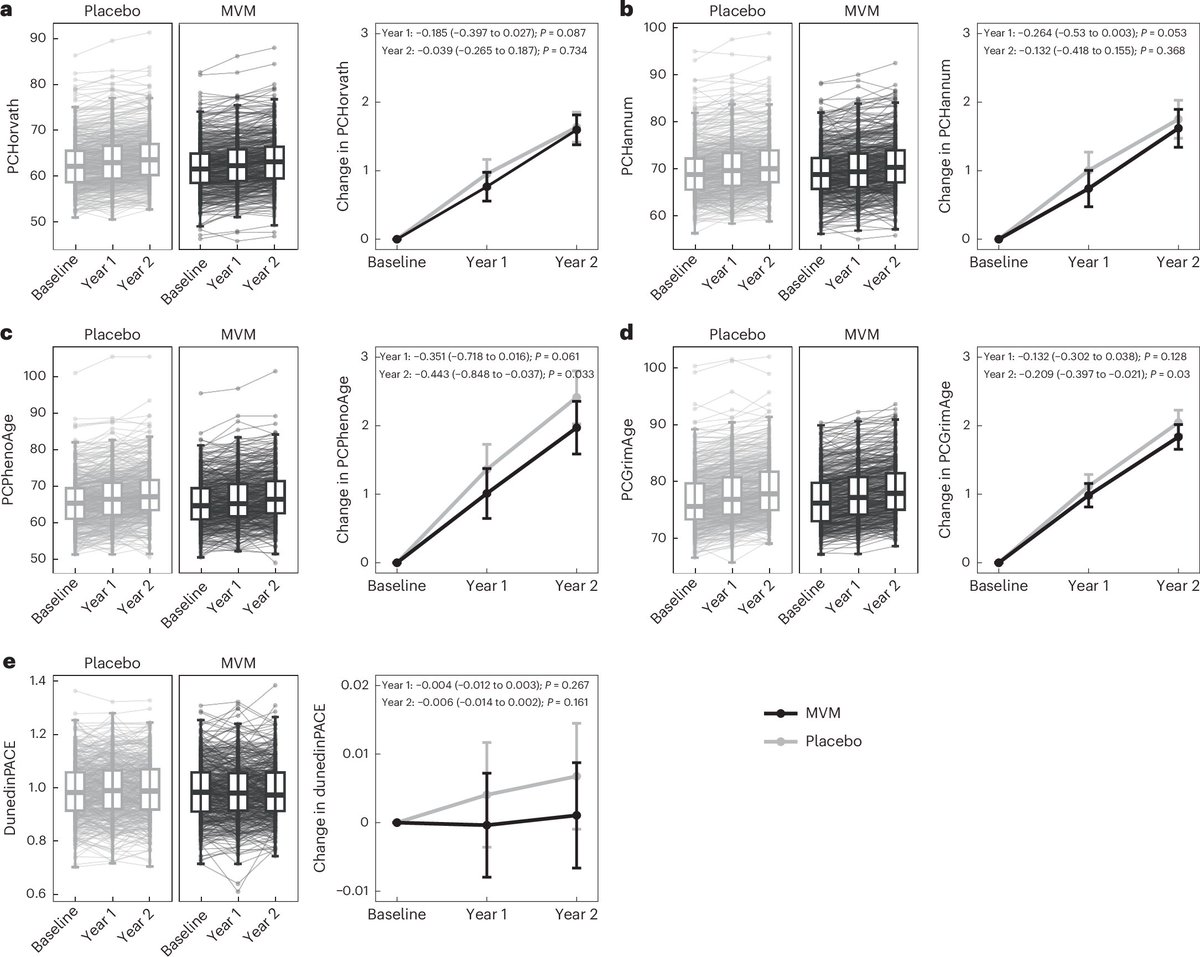
Multivitamin supplementation slows biological aging.
Older adults taking a daily multivitamin for 2 years reduced their pace of epigenetic aging by 0.1–0.2 years compared with placebo. The effect was strongest in people with accelerated biological aging.
Interestingly, cocoa flavanol supplementation showed no effect on epigenetic aging in the same trial.
The effect is small, but it adds to evidence from the COSMOS trial, where multivitamin supplementation improved cognitive function, despite showing no clear benefits for cancer, cardiovascular disease, or all-cause mortality.
The data challenge the idea that multivitamins are “completely useless," even if their benefits appear modest and context-dependent.
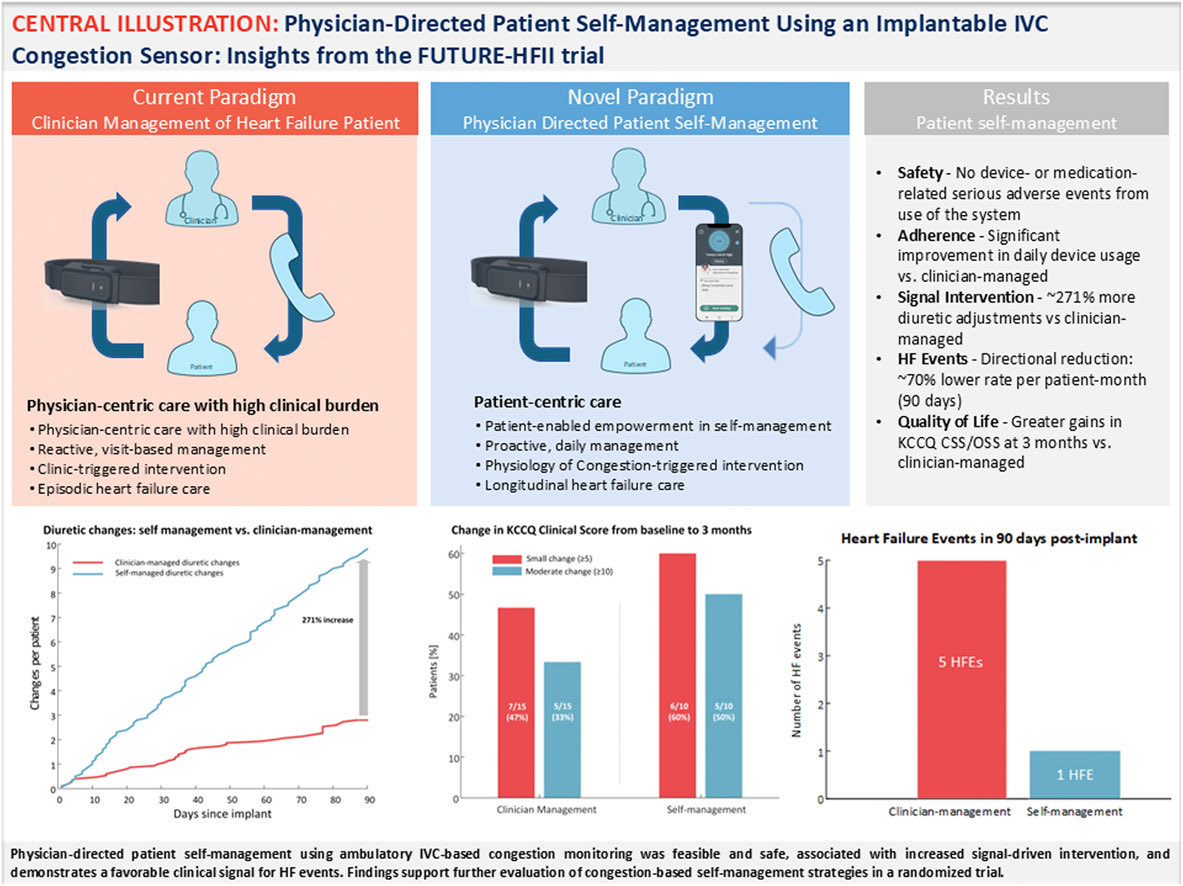
Now in @JACCJournals: Insights from the FUTURE-HFII trial by #HFC members @FudimMarat, Tre Martyn et al. show ambulatory IVC congestion monitoring enabled physician-directed self-management and increased signal-driven interventions.
https://t.co/wXNVvW5hfC
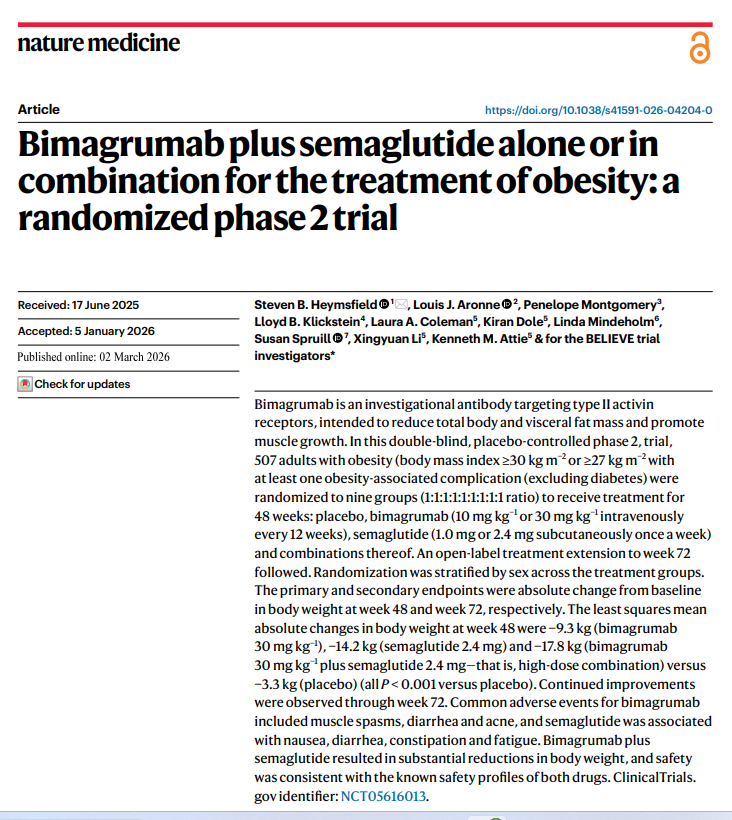
BELIEVE it or not… this obesity trial suggests we may finally separate fat loss from muscle loss.
In the BELIEVE trial (Nature Medicine):
🔹 Semaglutide alone → ~15.7% weight loss
🔹 Combination therapy → ~22% weight loss (~24 kg)
🔹 Total body fat ↓ ~46%
🔹 Visceral fat ↓ ~58%
🔹 Lean muscle largely preserved
For decades, weight loss meant losing muscle + metabolic reserve.
This approach targets appetite AND muscle biology simultaneously.
If confirmed in outcomes trials, this could reshape how we think about:
❤️ cardiometabolic disease
💪 sarcopenic obesity
🫀 surgical risk & frailty
We may be moving from weight loss → body composition medicine.
#Obesity #CardioMetabolic #GLP1 #Semaglutide #Longevity #HeartHealth #PreventiveMedicine #NatureMedicine #MedTwitter #Cardiology #Endocrinology #DigitalHealth #FutureOfMedicine #HealthyAging #PrecisionMedicine
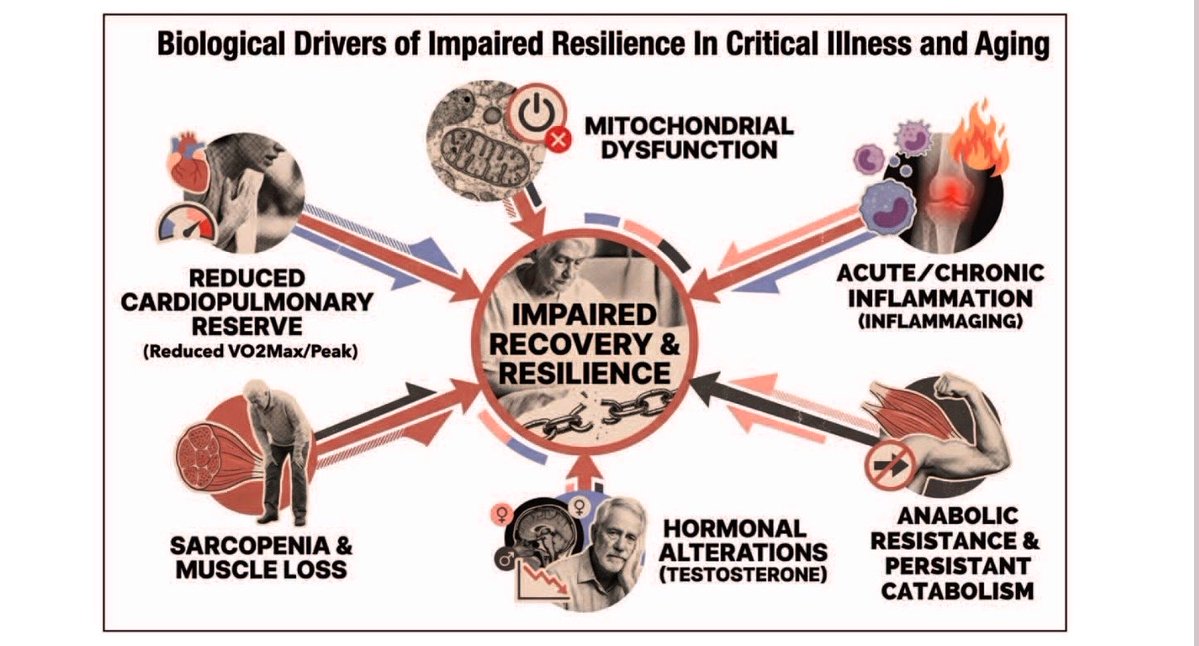
Rethinking frailty, muscle, and protein through the lens of aging biology
The dominant narrative around aging and frailty is deceptively simple and wrong:
eat more protein + resistance exercise → activate mTOR → build more muscle → reduce frailty.
https://t.co/C6g6HPgyze