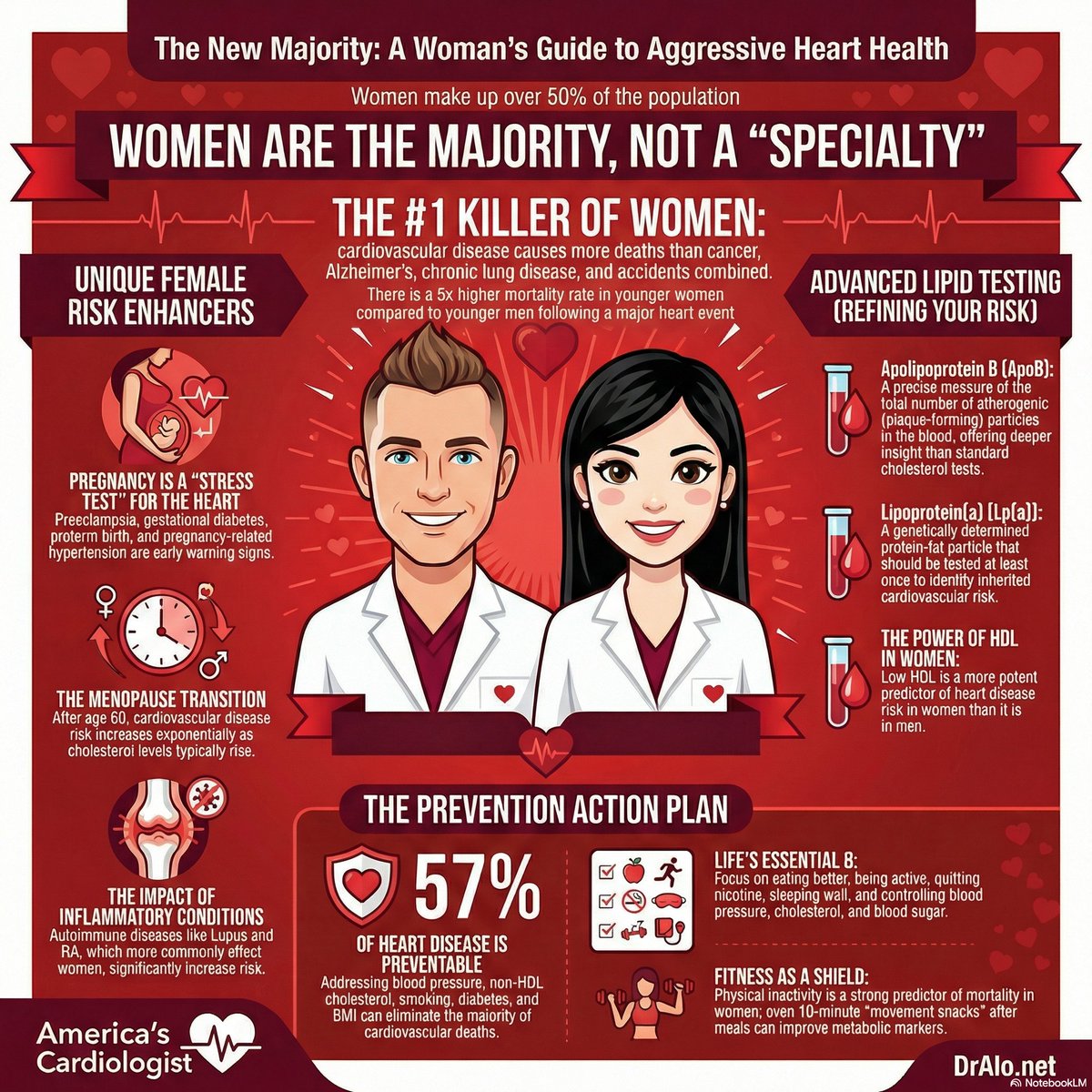
🚨 Heart disease kills more women than all cancers combined.
Every year, 1 in 3 women dies from cardiovascular disease, yet 80% of women still believe cancer is their biggest threat.
The data says otherwise.
🫀 Women's heart attacks do not look like the movies.
No crushing chest pain. No left arm shooting down. Instead, women present with jaw pain, nausea, fatigue, and shortness of breath. Cardiologists miss it. ERs send them home. And women die from a disease they never knew they had.
This is why women need to pay attention.
🔬 Here is what the science actually says.
Women develop cardiovascular disease 7 to 10 years later than men on average. But once a woman has a heart attack, her 30-day mortality rate is higher than a man's. Her symptoms get dismissed 50% more often in emergency settings. She is less likely to receive guideline-directed therapy after an acute coronary event.
That is not a biology problem. That is a recognition problem.
💓 Female-specific risk factors that most doctors never ask about:
✅ Preeclampsia doubles lifetime cardiovascular risk.
✅ Premature menopause before age 40 increases risk by 40%.
✅ Polycystic ovary syndrome triples the risk of heart attack in women under 50.
✅ Autoimmune conditions like lupus and rheumatoid arthritis carry cardiac risk equivalent to smoking.
⚠️ The standard treadmill stress test misses coronary artery disease in women up to 67% of the time.
Women need different testing. Coronary artery calcium scoring, cardiac CT angiography, and stress echocardiography perform far better in female patients than exercise ECG alone.
🩺 Know your numbers. All of them.
LDL cholesterol. ApoB. Lp(a). Blood pressure. Fasting glucose. hs-CRP. Triglycerides.
Lp(a) is inherited, does not respond to statins, and affects 1 in 5 people. Women with elevated Lp(a) face dramatically higher cardiovascular risk after menopause when estrogen drops and inflammation rises. Most women have never had this test ordered.
❌ Hormone replacement therapy alone will not save you.
❌ Calcium supplements alone will not save you.
❌ Wishful thinking about your family history will not save you.
"The tools with the strongest data are unsexy, free, and require your participation."
Blood pressure control. Lipid management. Blood sugar regulation. No smoking. Regular movement. Sleep. These are the interventions that cut cardiovascular mortality in women by up to 80%.
❤️ Bottom line:
Heart disease is not a man's disease. It is the number one killer of women in America, and it is largely preventable.
A woman who knows her ApoB, screens her Lp(a), controls her blood pressure to under 120 systolic, and exercises 150 minutes per week can reduce her cardiac event risk by 80% over the next 10 years.
That is the difference between surviving menopause and dying from a heart attack at 62 that everyone called unexpected.
Ask your doctor for a complete cardiovascular risk panel. Not a basic cholesterol panel. A complete one.
The question is no longer whether women get heart disease. The question is whether your doctor is looking for it correctly.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #WomensHeartHealth #WomenAndHeartDisease #Lpa #ApoB #PreventiveCardiology #WomensHealth
Autoantibody screening in children who are first-degree relatives of people with type 1 diabetes: multicentre prevalence, determinants and post-screening parent–child anxiety #T1D#DiabetesResearch https://t.co/IDlPYN83mT 🔓️
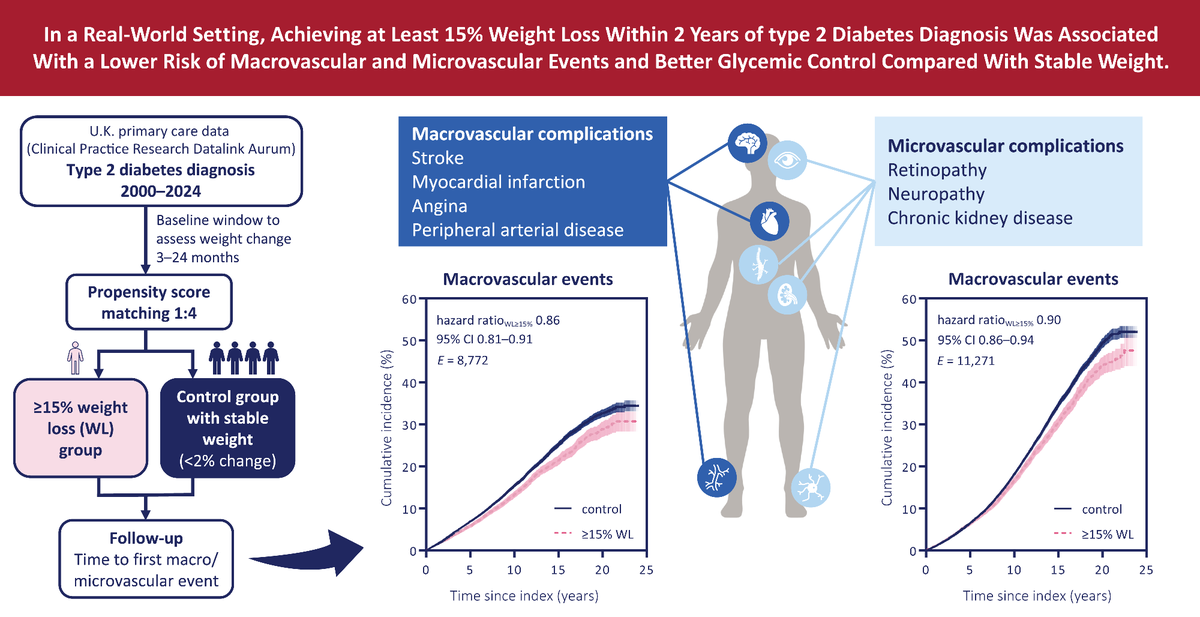
UK real-world data: In adults with obesity, losing ≥15% weight within 2 years from type 2 diabetes diagnosis was associated with lower risks of macrovascular (14%) and microvascular (10%) events.
Read here ➡️ https://t.co/u3gT9akYh8
@AmDiabetesAssn@ADA_DiabetesPro@ADA_Pubs
Two people can be identical on paper, same weight, same insulin resistance, same fasting glucose, and the diet that improves one does nothing for the other. What separates them is not how resistant they are but which organ the resistance is strongest in.
A Dutch team ran the trial precision nutrition usually only promises: 242 adults, randomized, twelve weeks. They measured whether each person's insulin resistance sat in muscle or liver, then assigned two diets, high-monounsaturated-fat or low-fat/high-protein/high-fiber, so one group's pairing mirrored the other's. When the muscle-resistant people got the high-fiber diet and the liver-resistant people got the high-fat one, their insulin sensitivity, glucose control, triglycerides, and CRP all improved more than the reverse pairing. Same diets, same twelve weeks, same baseline resistance. The only difference was matching the diet to the tissue driving the problem.
The pre-registered primary outcome was null, so this lives in secondary markers, it's twelve weeks in adults with a BMI of 25 to 40, and the phenotyping needs a timed glucose tolerance test most clinics don't run.
Proof of concept, essentially. But it tests the actual premise the personalized-nutrition industry sells, that your biology should set your diet, with a real measurable readout instead of a genetic or microbiome guess. That's rare, and it's the version of that claim worth taking seriously.
This free summary can be used to help your patients understand how the @ACPIMPhysicians Clinical Guidelines Committee developed new living clinical guidelines recommending weight management medications for nonpregnant adults with overweight or #obesity. https://t.co/Z7ZLJJCYNO
New study reveals early #glycaemic management is key in #Type2Diabetes. Achieving lower HbA1c levels earlier vs later after diagnosis was linked to a lower long-term risk of #cancer, even if overall glucose burden was similar https://t.co/Vn90UwnRAu 🔓 #DiabetesResearch
In the past 5 years alone, the number of clinical trials studying #obesity medications has increased nearly five-fold and more than 150 potential drugs are currently in the development pipeline https://t.co/IFPyEU8bKn
#weightloss#GLP-1 receptor agonists
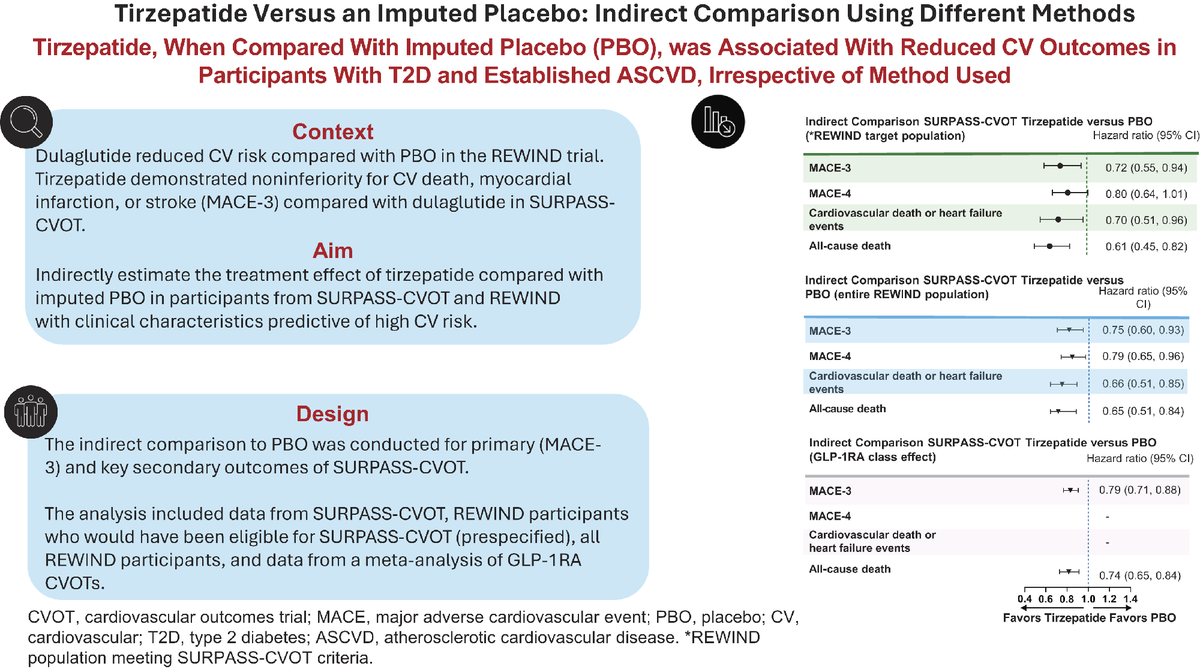
Indirect comparison of SURPASS-CVOT and REWIND suggests tirzepatide reduces MACE-3, CV death or HF events, and all-cause mortality versus imputed placebo in #T2D with ASCVD. #DCare#Article
Read here ➡️ https://t.co/pg6NUygR3B
@AmDiabetesAssn@ADA_DiabetesPro@ADA_Pubs
GLP-1 overdoses have been skyrocketing, with poison centers seeing a nearly 1500% increase in calls related to overdose or side effects of injectable weight-loss drugs since 2019, according to US National Poison Data Center.
Experts suggest that the use of compounded drugs has exacerbated the overdose problem. However, increased utilization of GLP-1s and lack of patient education are also among the contributing factors. https://t.co/wrZdbxvSKP
Gabapentinoids like gabapentin and pregabalin are associated with an increased risk for poisoning, with the highest risk occurring around treatment initiation and when combined with benzodiazepines or opioids.
In a large UK study of nearly 17,000 primary care patients, those who had co-initiation of gabapentinoids and benzodiazepines showed double the risk for hospitalization due to drug poisoning within the first month, whereas those with concomitant opioid use showed a 30% increased risk compared with those who took neither medication. https://t.co/djHDrx5vjQ
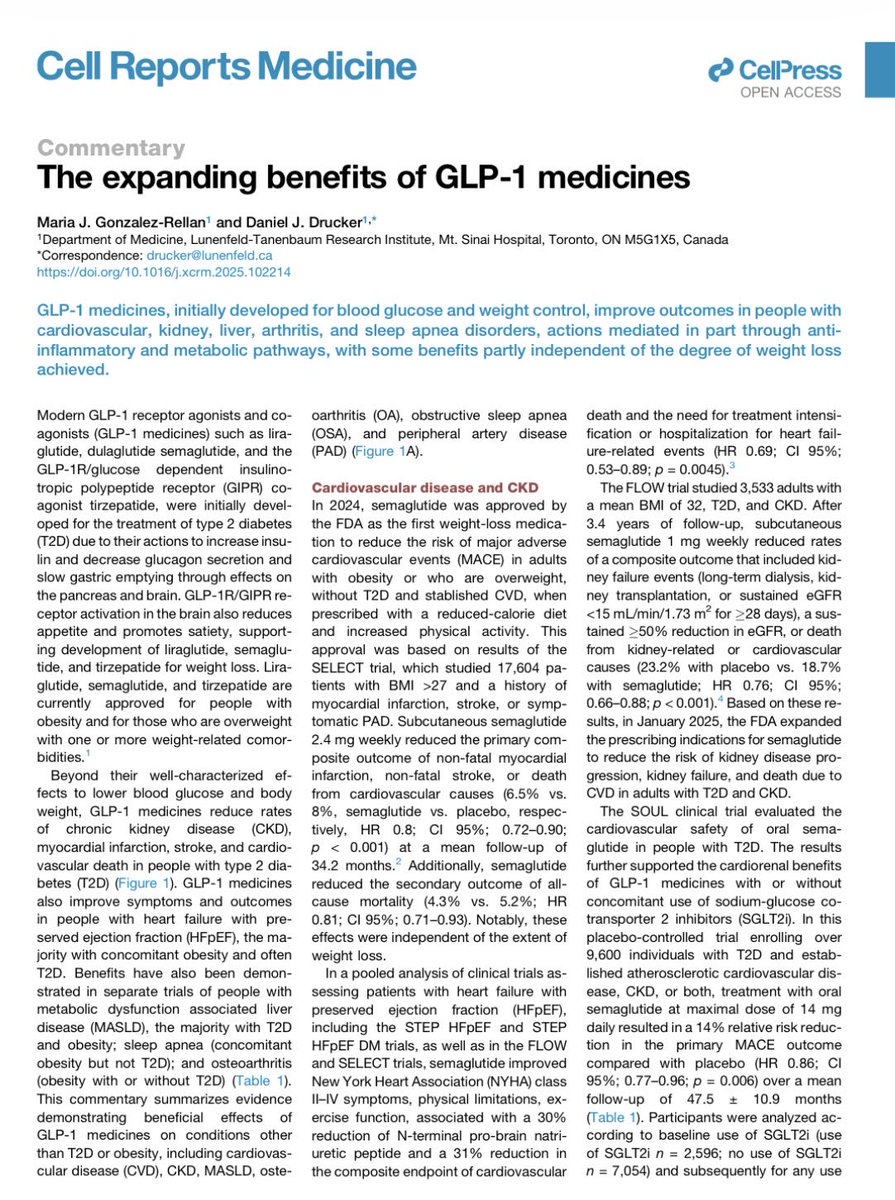
New review by Maria Gonzalez-Rellan & Daniel Drucker focuses on the expanding benefits of GLP-1 meds like semaglutide & tirzepatide. Beyond glucose/weight control: ↓ CVD events, CKD progression, MASLD, OA, sleep apnea (via anti-inflammatory paths) partly weight-loss independent.
https://t.co/hRvaPYBr1X
Our review published
Fixed‑Dose Combination Therapy as a Strategy to Improve Antidiabetic Medication Adherence in People with Type 2 Diabetes
Unfortunately not used much in UK despite their advantages.
led by Patrick Highton
https://t.co/sJfQOp4ztO
Experts share a practical curriculum on how a proactive approach to obesity and metabolic risk can redefine long‑term liver health—identifying early warning signs and enabling timely intervention.
Explore this CME ▶️ https://t.co/ilRTPnnQKD
Findings from an analysis of deidentified electronic health record data from a national database indicate that the prevalence of youth-onset type 2 diabetes has increased substantially during the past decade. Full study results: https://t.co/8H7RiG7PDW
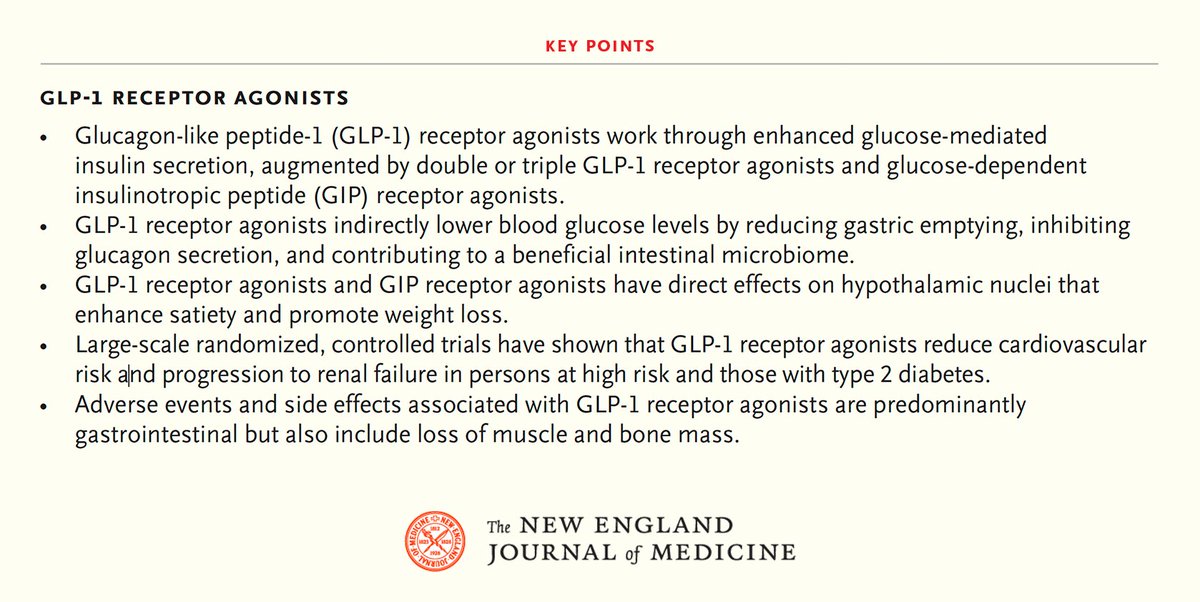
A new review by Clifford J. Rosen, MD, and Julie R. Ingelfinger, MD, describes a new generation of treatment with GLP-1 receptor agonists for persons with obesity with or without diabetes or prediabetes. Learn more: https://t.co/SNdSrVXqWJ