Restoring the Heart of Healthcare → 1. Support for Patients, → 2. Support for Independent Providers, → 3. While We Fight for Justice and Change! #healthcare
Here is a recent story about one of our patients who was switched to Humana Medicare Advantage. She is 75 years old, has a port in her chest, is undergoing chemo for cancer, had a recent surgery, and is homebound—too weak to walk and reliant on a wheelchair.
When she was switched, no one told her that her home health provider and PCP were out of network. Her eligibility now shows "CenterWell Primary Care." This caused an immediate interruption in her care. Now, she has to worry about switching to new doctors. When she finally got an appointment with a CenterWell Primary Care doctor, they told her there was "no need" for home health.
Why would they do that?
Because they collect Medicare dollars regardless of whether they deliver the care or not. The less care they provide, the more money they keep. How is this beneficial to patients? It is criminal.
This patient, like many others, is now trapped in their system where independent providers are blocked out of the network. Patients have no choice and no access to quality care. Humana’s provider lists are full of "ghost providers" or providers with no active contracts who don’t even know they are on the list—most with 1 or 2 stars so people won't call them. (Ask me how I know: I have personally called over 1,200 providers listed in their directory.)
Meanwhile, they list their own agencies 2–3 times—some with addresses that don't even exist, just a phone number routing to a different location. (Ask me how I know; I have all the evidence. In fact, the only reason they finally sent me an offer was that I proved they were locking me out with the false excuse that they met federal network adequacy requirements. "No, you did not, and you never do". But again, no one is doing anything about it, although this has been a problem for years.)
Humana is the worst. Their actions toward patients, VETERANS, and competitors are truly criminal. They should never be allowed to act as competitors to the very providers they pay. In what other industry can your direct competitor tell you who your customers can be and how much you can be paid? They pay themselves 3–4 times more than they offer independents. It is unreal that this is allowed to continue.
We lost 9 patients on January 1st because of Humana. None of them knew they wouldn't be able to continue their care with us. When we checked, all 9 are now trapped with a CenterWell doctor, CenterWell pharmacy, and everything else in that ecosystem.
Every patient they add to their pipeline is just a dollar sign—not just the regular Medicare payment, but the "Quality Bonus" payments. They received $2.5 BILLION in bonuses in 2024! Meanwhile, my 4-star rating gets a slap in the face: an offer 70% below Medicare reimbursement rates, which they sent knowing I could never sign it.
I am in competition with 11 of their home health agencies—19 if I count the GHOST LISTINGS under CenterWell. They have made, and continue to make, every effort to eliminate me as a competitor since they arrived in town 7 years ago. It started with a bogus lawsuit against my agency, which they lost and were sanctioned for (accusation: I am stealing market share! Yes, I am serious.)
I thought it was over, but that was just the beginning; the retaliation has been full speed ever since. I have ZERO PROTECTION AGAINST THEM. They are stealing, cheating, and breaking every law possible, utilizing exemptions that don't apply to us. It feels like I am being robbed daily, but I can't call anyone to the rescue because the regulators seem to be in their pockets. That is our healthcare system.
They never complied with the Price Transparency Act, and now that it's being enforced, they've exited the commercial market to focus solely on Medicare Advantage. Why that bill doesn't include Medicare Advantage is beyond me. Since it’s taxpayers' money, I guess they think it’s none of our business how it’s spent?!
Let's change that! The deadline to submit comments is February 23, 2026. EVERYONE NEEDS TO COMMENT, share, and ask everyone else to comment! (link below)
CMS wrote this proposal in December, before the President's "Great Healthcare Plan" was fully announced in January. They are out of sync. Your comment must bridge that gap. You need to tell CMS: "You must amend this rule to include Medicare Advantage plans immediately, to align with the President's January 15th directive."
Regardless of whether you like Trump or not, if you want the best for people, taxpayers, seniors, VETERANS, and independent providers, demand MA to be included. This can help end a lot of fraud in Medicare Advantage and help expose the anticompetitive tactics used by these monsters against others. (BTW IT INCLUDES DRUG PRICES AND REIMBURSEMENTS TO PHARMACIES, PBMs, AND WHAT THEY REIMBURSE THEMSELVES...)
@CMSGov@DrOzCMS@RobertKennedyJr@mcuban@GmOrr9000@SecScottBessent@SusieWiles
LINK: https://t.co/QkWMkoFkZk
Business owner raised huge amounts of money from private equity firms
He then bought dozens of hospitals and bankrupted them. Many are now closed
He and his partners walked away with millions. He bought a $40 million dollar yacht
Private equity firms are destroying America
“The weird thing is, even though the hospital chain collapsed, a lot of people at the top still walked away with enormous amounts of money. You're supposed to get a big payout like that when you succeed, not when you fail.”
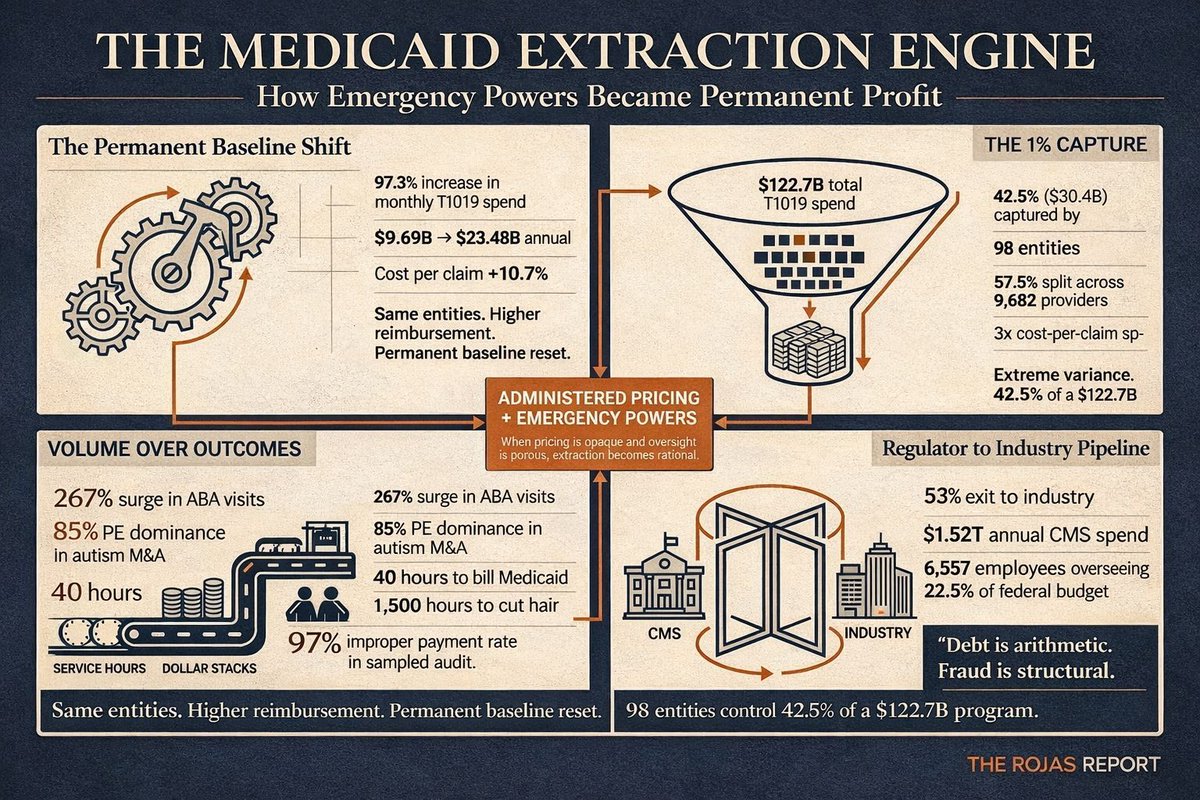
𝐓𝐡𝐞 𝐔𝐧𝐢𝐭𝐞𝐝 𝐒𝐭𝐚𝐭𝐞𝐬 𝐝𝐨𝐞𝐬 𝐧𝐨𝐭 𝐡𝐚𝐯𝐞 𝐚 𝐝𝐞𝐛𝐭 𝐩𝐫𝐨𝐛𝐥𝐞𝐦.
It has a fraud problem.
For years we have been told the national debt is the unavoidable byproduct of entitlement math, demographics, and fiscal gravity.
An aging population.
Rising healthcare costs.
Structural deficits.
But the HHS Medicaid data release last Friday tells a different story.
Improper payments measured in the hundreds of billions.
Programs that doubled in size and never returned to baseline.
Provider counts barely moving while per-claim costs exploded.
Oversight mechanisms that appear ornamental rather than operational.
This is not abstract macroeconomics.
This is administrative failure at industrial scale.
A nation can survive debt.
History proves it.
Britain exited the Napoleonic Wars with debt exceeding 200 percent of GDP and endured.
The United States financed World War II at levels that would terrify today’s deficit hawks.
What nations do not survive is systemic erosion of trust.
When taxpayers suspect that billions are siphoned through incompetence, indifference, or fraud, the social contract weakens.
When lawmakers debate marginal tax rates while ignoring structural leakage inside federal programs, credibility collapses.
Debt is arithmetic.
Fraud is culture.
And culture, once corrupted, is far harder to repair than a balance sheet.
If even a fraction of what this data suggests proves actionable, then the debate in Washington is misframed.
The question is not simply how much we borrow.
The question is how much we tolerate.
We have submitted names.
We have submitted addresses.
We have submitted amounts.
Now we will see whether oversight in America is theater or governance.
IT’S AMAZING WHAT YOU CAN AFFORD WHEN YOU DON’T PAY TAXES.
A nonprofit hospital in Philadelphia just bought naming rights to the Eagles’ practice facility.
It lost $201M in six months.
Laid off 650 employees.
All three credit agencies:
Negative outlook.
When physicians leave independent practice for hospital employment, Medicare costs per patient per year increase by $1,327.
When they move to models that preserve the practice structure, costs decrease by $963.
Consolidation does not reduce spending.
It increases it.
The data is not ambiguous.
https://t.co/AFedwlyoWB
Dear @POTUS@realDonaldTrump@SecKennedy@RobertKennedyJr & @DrOzCMS@DrOz You have the power to radically lower healthcare costs in the USA by ENDING the ridiculous 2-tier payment system where the SAME clinic owned by a “hospital” gets paid 2-3x for the SAME visit.
Where does that $ go? Not to doctors. To hospital CEOs/leadership.
CEO of @UCLAHealth - a STATE institution - made nearly $2.5 MILLION in 2024!
Hospitals have exploited this by buying non-hospital clinics, calling them hospital outpatient centers, and raking in the cash. And they build massive outpatient facilities that regular docs cannot compete with.
End this today and I promise healthcare costs will plummet.
There is no enforcement, and they post the information in such large files that they can't be downloaded. We looked into getting the data through a few companies where it's available; I did a demo, and in the end, accessing nationwide pricing would have cost over $100K. That’s not a typo. It was supposed to help people see prices and allow independent providers to fight for fair rates, but instead, it became another tool for large healthcare systems and private equity firms to use for their own benefit.
.@DrOzCMS: “Loneliness has become a real problem as we’ve been discussing at this agency for quite some time. @SecKennedy has been highlighting this issue as he tries to address some of the challenges with mental health and anxiety and depression that are plaguing so many Americans.”
The largest U.S. health insurance companies aren't just insurers anymore. They diagnose, treat, dispense drugs, set prices, and decide coverage-all while legally obligated to prioritize profits over patients.
One entity now controls almost every step of your healthcare journey.
They own hospitals, employ doctors, run clinics, operate pharmacies, and control pharmacy benefit managers (PBMs) that decide which drugs you can get and how much you pay.
This is the reality. Independent providers hire people who care and fight for their patients to get the care they need. What will happen when we are all gone—because our politicians won't change the policies and don't stop the giant health insurance companies from eliminating us? They will be the only providers left controlling your care, and it will never be about what you need, but about what generates the most profit for them. They hire people who obey and fight for their bottom line, not for the patients. Patients won't even realize they could have had the medication, the tests, or the treatment that would have saved their life—or their loved one's life. @FTC@OIGatHHS@HouseCommerce
“A nurse records herself begging UnitedHealthcare to approve care for her patient.”
She’s had authorization for OVER A MONTH — and they still won’t provide the service.
Delay after delay, denial after denial — that’s the state of American Healthcare.
Same here. I've recorded them a few times acting like I'm an old lady. They're scamming elderly people by offering $250 in groceries and a gas card. I don't understand how these people can't be stopped when they make millions of calls daily. I get at least 10 calls a day. If you talk to the AI, it transfers you to live person (probably overseas). Calling me as I am typing.
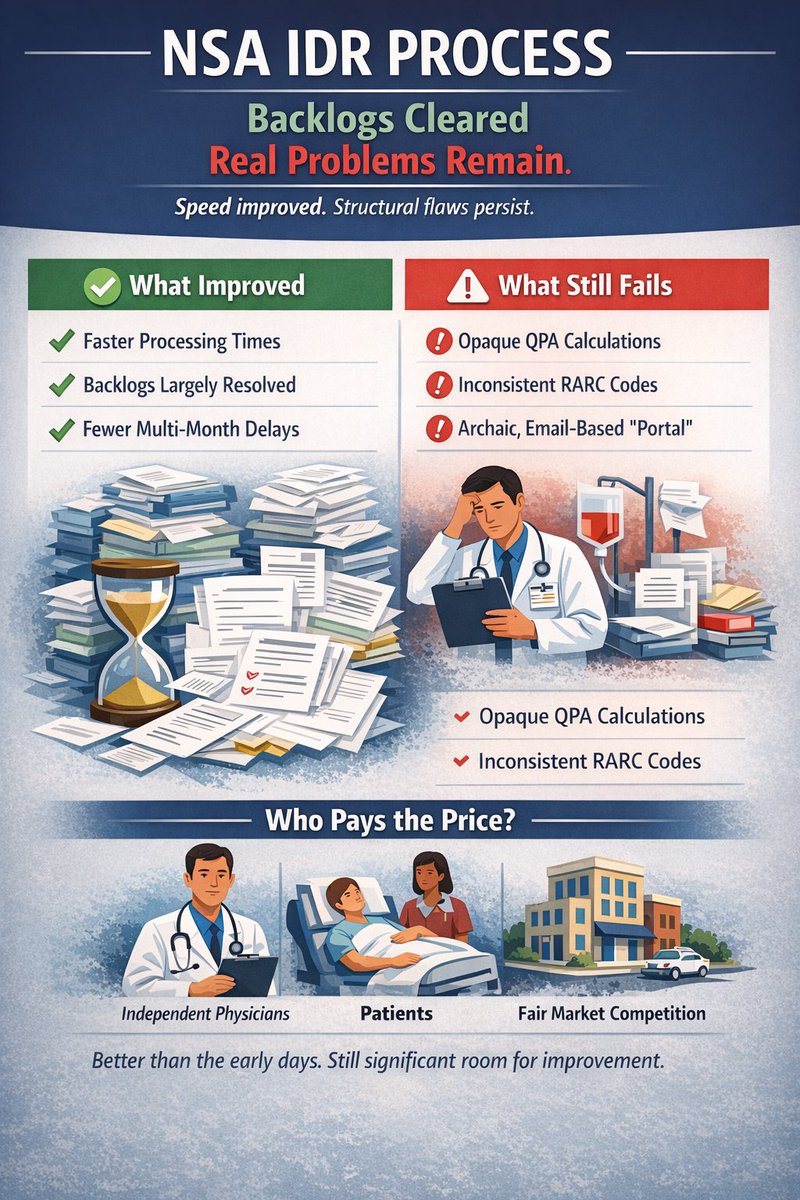
This Week’s Focus: The NSA IDR process backlogs have cleared but real problems remain.
After more than three years of implementation, the No Surprises Act Independent Dispute Resolution process has finally turned a corner on the massive backlogs that once defined the system. Processing times have improved substantially, and most disputes are now moving forward without the months long delays we saw in 2023 and 2024. The latest Cassidy and Hassan letters rightfully acknowledge this change.
That progress matters. Unfortunately speed does not necessarily equal success.
The IDR system still suffers from serious operational and structural flaws that make it unnecessarily complex, costly, and unfair, particularly for independent physician practices that lack the scale and infrastructure of large corporate players.
This week, we’re taking a hard look at the issues that continue to undermine the intent of the No Surprises Act, including:
- Opaque and often non compliant Qualified Payment Amount calculations and updates
- Inconsistent and inadequate use of RARC codes, creating widespread eligibility confusion
- An archaic, email based communication system instead of a true unified portal
The No Surprises Act was designed to protect patients and create a fair, efficient dispute resolution process. Today, it is much better than it was in the early days, but there is still significant room for improvement. The consequences land squarely on physicians and, ultimately, on patients.
Tuesday through Thursday, we’ll break down the operational pain points. Friday, we’ll focus on concrete policy fixes and enforcement actions that could actually make this system work as intended.
@Humana can you explain this?
@DrOz@realDonaldTrump@SecKennedy@mcuban
When will we make the madness stop?
What about glyburide requiring a PA?!?
GW and the patriots started a revolution over similar tresspasses.
BlackRock/Vanguard/State Street in all of them... they run the show. They are the biggest investors in the PE firms that collude with the health insurance companies to pick up the independent providers they force out for pennies on the dollar, then they give them big contracts to make big profits and then flip to the insurance companies. This is how they get around the antitrust laws. But the same big boys get their cut in all of it. But if an independent doctor gets a burger paid for by someone that they may refer some patients to, they go to jail. (Okay, maybe I exaggerated a little on the doctor lunch, but not much.)
The total Medicare and Medicaid dollars handed over to health insurance giants in 2025: $1.05–1.15 trillion (using midpoints like ~$540 billion for Medicare Advantage and ~$550 billion for Medicaid managed care).
YOUR TAX DOLLARS ARE BIG BUSINESS TO THE HEALTH INSURANCE CARTEL! You know—the ones that deny your care and meds, put independent providers out of business, and celebrate when they make you so poor that you need Medicaid, so they can get more money from our government!