Chief🫀fellow @OHSUCardFellows 🔜 Cardiac Crit Care @OHSUCardio | IM @BCM_InternalMed | MD @CayetanoHeredia 🇵🇪. Interest in walkability and urban planning.
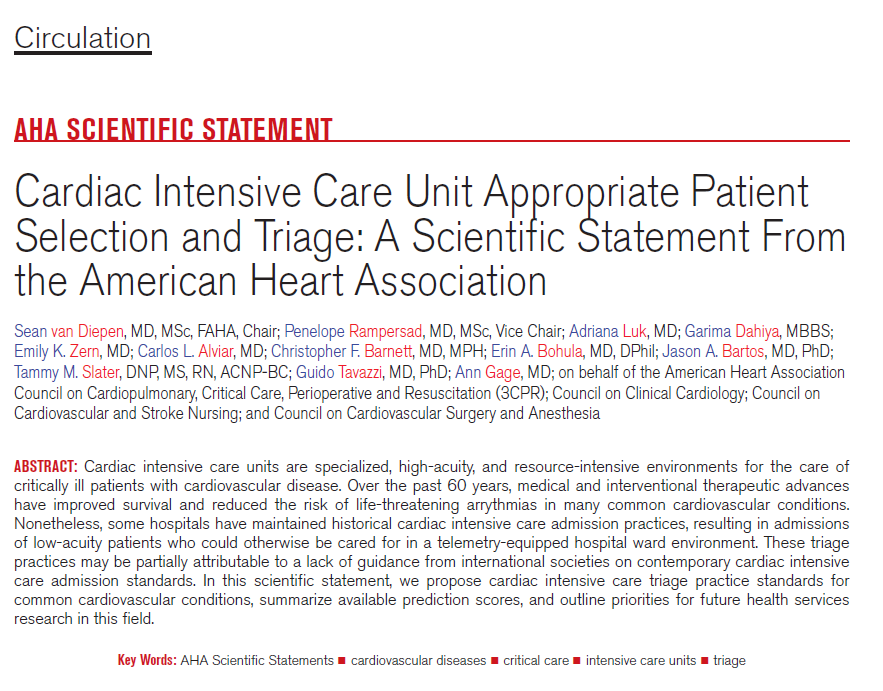
This Scientific Statement suggests a framework for CICU admission decisions based on the potential beneficence of critical care restricted monitoring or therapies, patient goals-of-care, and the risk of early adverse cardiovascular events among common cardiovascular admission diagnoses.
✍🏼 @seanvndiepen @PennyRampersad@AnnGageMD@AdrianaCLuk
ICU care saves lives but it's resource intensive.
US healthcare produces ~8–9% of total US carbon emissions; that's more than all of 🇯🇵!
A single day of ICU care for septic shock may generate ~170 kg of CO₂, equivalent to driving a gasoline car >400 miles.
How can we do better?
A @OnePagerICU, a @CritCareTime Podcast episode, and a thread!
1/
“I never thought of that.”
That was the most common reaction to our poster at #ACC26.
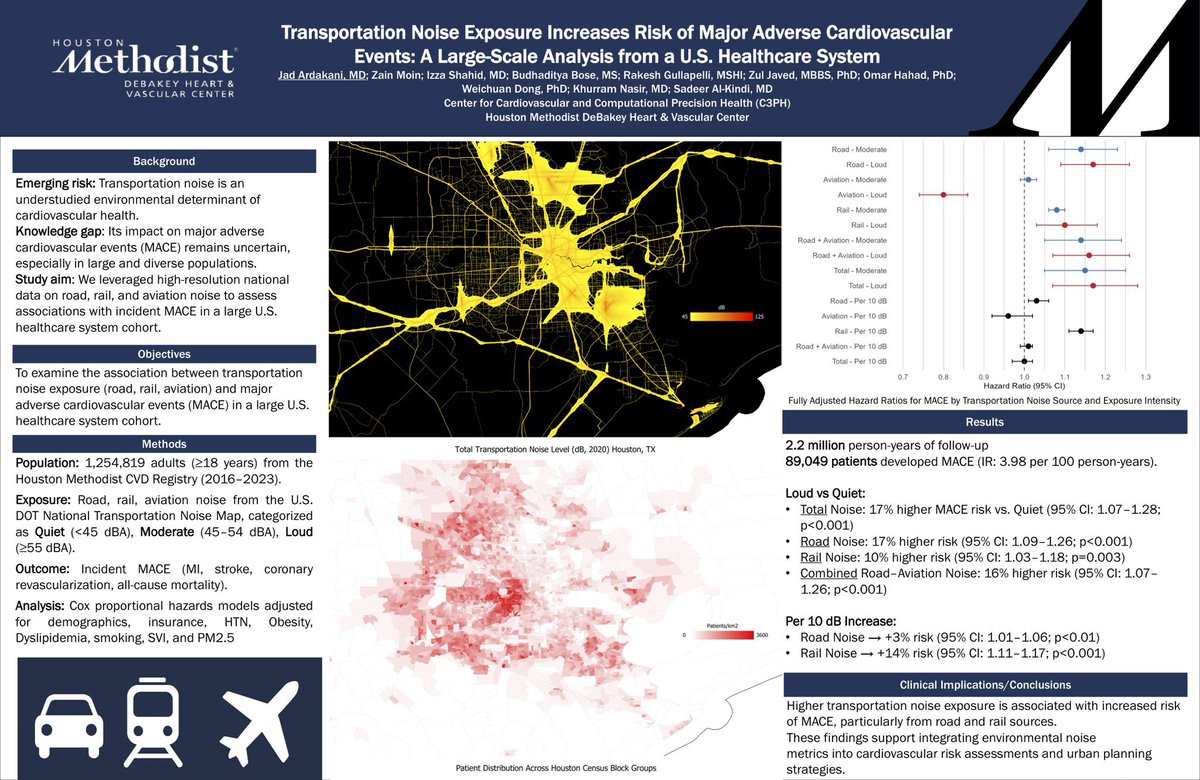
Transportation noise and cardiovascular risk aren’t typically mentioned in the same sentence, but they probably should be 🚗✈️🚆
Transportation noise at the residential level is an underrecognized environmental risk factor, capturing the chronic exposures people experience where they live.
In a large U.S. healthcare system cohort (n=1.25M+), we found:
• Higher noise exposure → higher MACE risk
• Total noise: +17% risk (HR 1.17)
• 🚗 Road noise: +17% risk
• 🚆 Rail noise: +10% risk
📈 Per 10 dB increase:
• 🚗 Road noise → +3% risk
• 🚆 Rail noise → +14% risk
These findings align with a growing body of literature linking transportation noise to cardiovascular risk through established biological pathways, including chronic stress and sleep disruption.
This study has important implications, from how and where we choose our homes, to how we design and build living environments, to how individuals optimize their sleep and reduce noise exposure at home.
Looking forward to publishing this work very soon.
Grateful to my mentors @Sadeer_AlKindi & @khurramn1 and collaborators for their support.
This almost impossible in many parts of the country and in many cities where safety is an issue.
And unfortunately those struggling to make ends meet are the ones disproportionately affected by lack of safe neighborhoods or are in rural areas where driving is essential.
I saw responses to this tweet: how walking everywhere is not possible in the USA. While I agree with that sentiment/ I know where Martha is coming from- population health is not personal—it’s engineered by the environments we create around us.
Singapore is a perfect example of this. The “newest” (hu)man made blue zone. The government has deliberately made car ownership extremely expensive (>$100K and limited via permits) and invested heavily in public transport—so walking and transit is the way of life. They’ve even built infrastructure like the Park Connector Network—a nationwide system of connected walking and cycling paths
Daily movement is built into life—even in a hot, humid climate( yes much worse than Houston)
This is essentially a “policy-driven Blue Zone”: not just culture or diet, but environment + incentives shaping behavior of the masses.
So Martha my friend- I applaud you for walking everywhere and having the courage to post something futuristic yet inspiring that currently doesn’t look possible in USA!
I don’t think Longevity is just about individual choices—it’s about systems, urban design, and political will.
Photos from Singapore last visit- walk/hike with family 😎
We need people to get more active not less. This means addressing the global issue of climate change. One thing people can do is stop driving everywhere. Can you walk to the store? Can you walk to an appointment? Can you walk to work? Can you get rid of a car? Or have no car at all? #hearthealth #climatechange
(& yes I have no car & walk everywhere to do my part!)
One of the most satisfying “prescriptions” I ever wrote was for a program that matched dogs in need of homes to patients with cancer, but required a doctor’s signature
Lots of confounders here, of course, but I can heartily endorse the companionship of man’s best friend
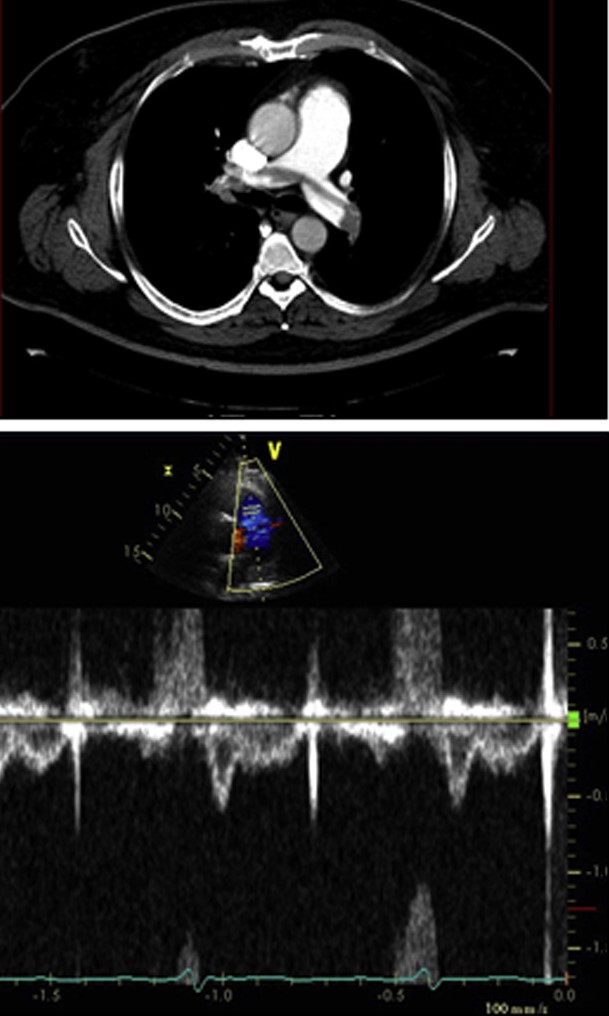
One of the important echo studies highlighting the importance of EARLY systolic notching of RVOT PW Doppler signal in patients with pulmonary embolism. This finding is present in >90% of patients with significant pulmonary embolism but it is uncommon in low risk/low thrombus burden patients. It is more prevalent than other well known echo phenomena, such as McConnell's sign, 60/60 sign, etc
https://t.co/XzlgiVm304
another patient death due to mythological fears about contrast dye.
modern contrast dye for CT scans doesn’t harm the kidneys.
definitive imaging saves lives.
get a contrast CT, save your patient’s life, don’t get sued.
https://t.co/yhnS0V9Hy9
A very important imaging study, which a substudy of POET trial, on residual vegetations after non-surgical treatment of left-sided endocarditis.
At the end of antibiotic treatment, more than half of patients have residual vegetations on TEE. Among these patients, most vegetations are unchanged in size compared to initial TEE.
More importantly, neither the presence nor size of the residual vegetations is associated with adverse outcomes, including embolic events, up to 4 years.
https://t.co/Sp9QQ4ubt8
Another round of applause to our current 3rd Year Fellows who have matched into their subspecialty fellowships!! 🎉🎊 We are so proud of your hard work paying off!! @OHSUCardio
If systemic hypotension was the sole cause of ischemic hepatitis, every patient in the MICU would have ALT >500
But the incidence is 1 in 50
You need right heart failure, congestion, that exceeds portal pressure. Then the systemic bp drop can be transient or relative