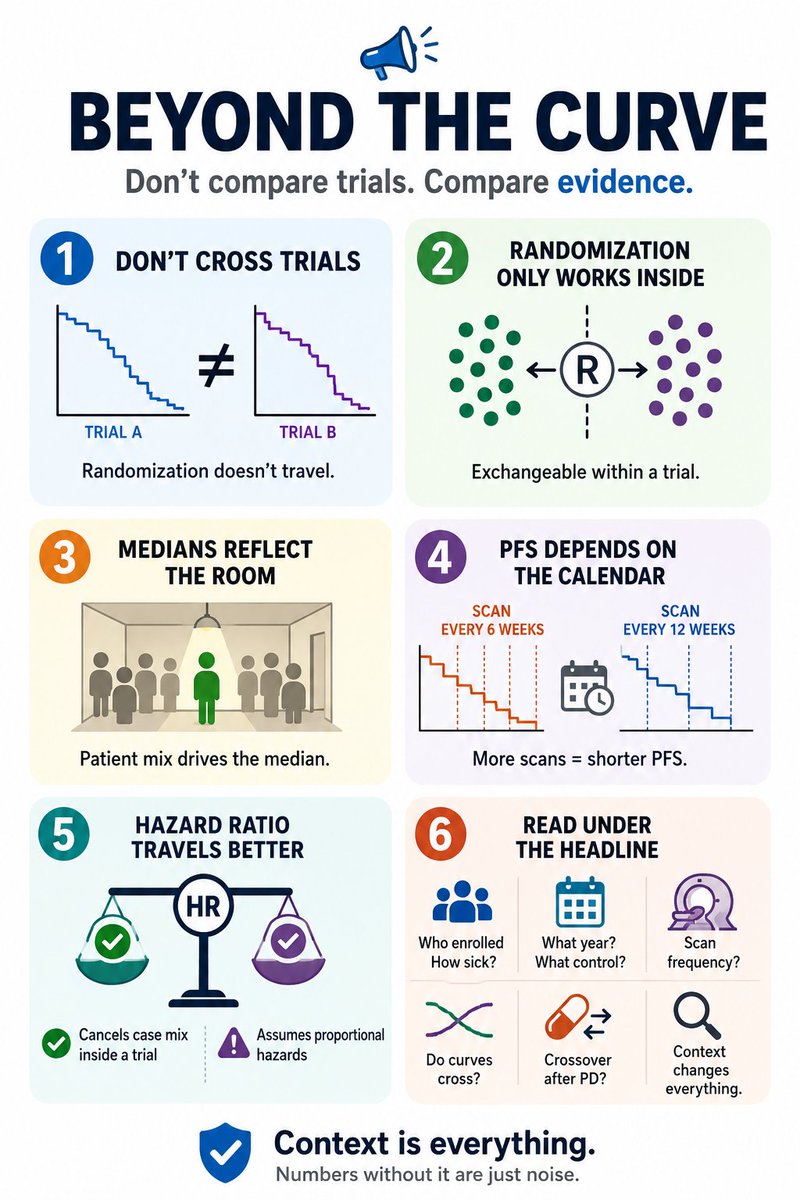
1/ #ASCO26 starts tomorrow. By Friday your feed will be full of survival curves, and the temptation will be everywhere: cross-trial/study comparison.
Before you do so, A few caveats worth keeping in mind
When Kaplan–Meier Curves Fool You 📉
A flat survival tail can look exciting…
but sometimes it reflects very few patients remaining under follow-up.
The curve alone is never enough.
Always check: • Number at risk
• Censoring patterns
• Follow-up maturity
• Late-tail denominator
A “long-term survivor plateau” is meaningful only when enough patients are still being observed.
One of the most important lessons in interpreting immunotherapy trials.
#Oncology #MedEd #Biostatistics #Immunotherapy #ClinicalTrials #KaplanMeier #MVOnco
🚨 FDA’s take on SERENA-6 is basically this:
“Nice data… but are we helping patients?”
Let’s break it down 👇
🧠 Problem 1: Wrong question
Trial asks:
👉 Switch early vs don’t switch
But real-world question is:
👉 Switch early vs switch later
FDA:
❌ “You didn’t answer the real question.”
⏱️ Problem 2: The PFS illusion
PFS looks great (16 vs 9.2 months)
But… it starts from:
👉 ESR1 mutation detection (not progression)
FDA:
❓ “What does this PFS even mean clinically?”
🧬 Problem 3: Biology mismatch
We assume: ESR1 mutation = resistance
FDA says:
👉 Not so fast
Patients may still benefit from AI + CDK4/6i
even AFTER mutation appears
👉 Early switch = stopping a working drug
🔁 Problem 4: No second chance
Control arm never got camizestrant later ❌
So we don’t know:
👉 Early vs delayed use
FDA:
❌ “This comparison is incomplete”
📉 Problem 5: Where is survival benefit?
OS = immature
Final data → years away
FDA:
👉 “Without OS, paradigm shift is risky”
⚠️ Problem 6: Not risk-free
QT prolongation
Bradycardia
Rare TdP
👉 Not a harmless switch
🎯 FDA’s real message:
“Just because we can act early…
doesn’t mean we should.”
🔖 Save this - this is how regulators think
📖 Full FDA briefing in comment ⬇️
#OncoTwitter #MedTwitter #BreastCancer #ESMOBreast26
@OncoAlert@myesmo@esmo_open@asco@OncBrothers
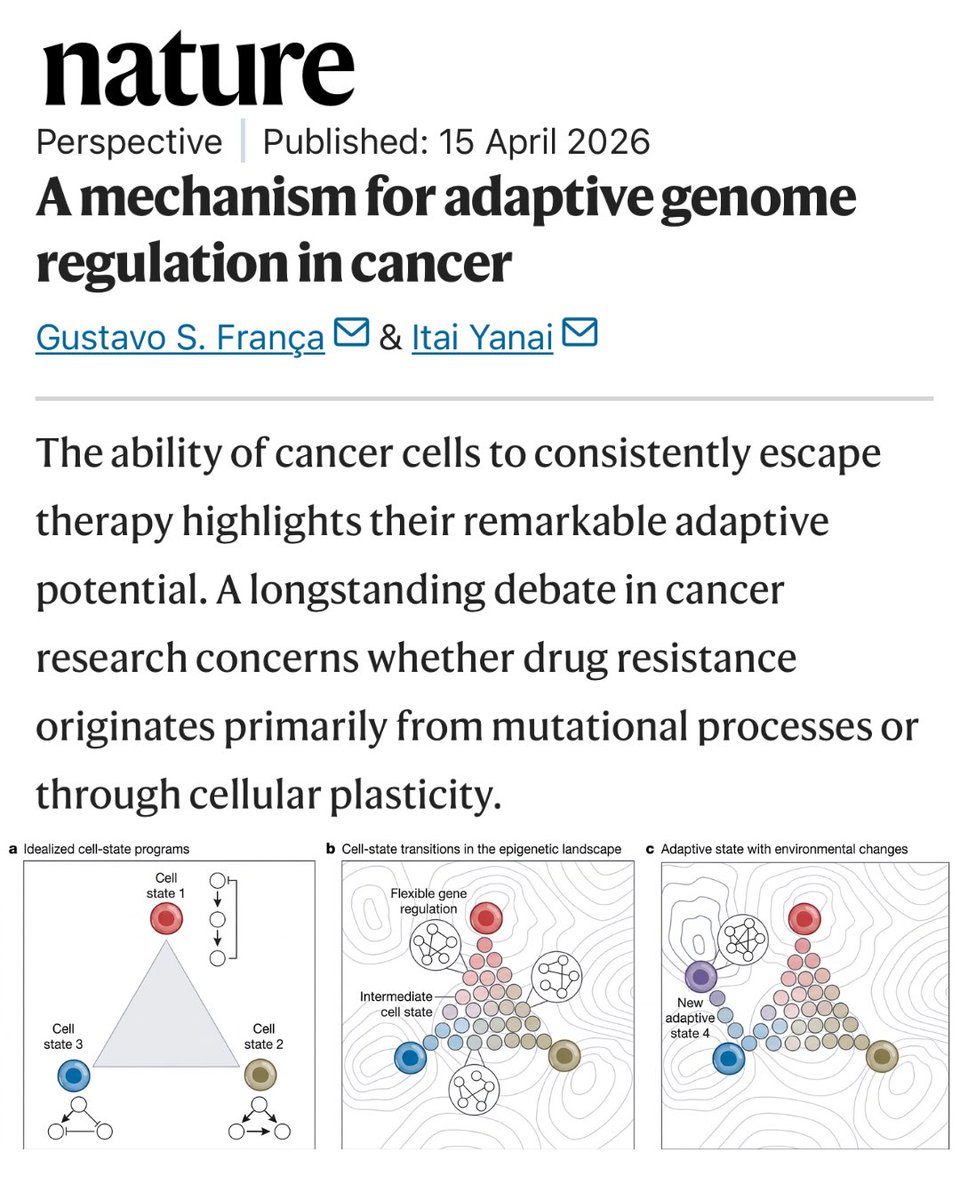
New research in Nature suggests cancer cells can learn to resist therapy, not by mutating, but by reprogramming themselves.
In #lungcancer, resistance to targeted treatments is a significant challenge. Understanding how this happens is an important step in the search for better treatment
🔗 https://t.co/RvSA6FljUj #LCSM
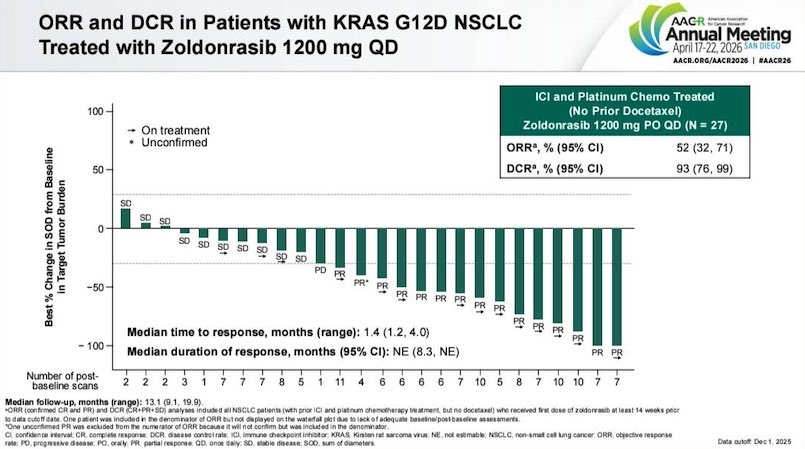
RevMed absolutely stole the show at AACR with their Pan-RAS and G12D inhibitors.
First line panc, second line NSCLC, even in early trials this is extremely compelling data.
2L NSCLC anti G12D (early data):
PFS: 11 months
ORR: 52%
G3 AEs: 13%
(Now compare that to 10 months with Osimertinib in 2L NSCLC)…
This can’t be FDA approved soon enough.
@OncoAlert@TheGutOncLab
This is a great article. Happening now with ADCs all w/ same payloads, PD1xVEGF bispecifics…what we really want is lots of high-risk, uncorrelated bets with high payoffs for patients. What we get is lots of similar, low-risk bets all competing for statistical mirages
🔥💉 Immunotherapy timing does NOT impact survival - morning 🌅 vs afternoon 🌙 makes no difference #ELCC26
LBA2 - i-TIMES answers a long-standing chronotherapy question in lung cancer 👇
🧬 Study population
Advanced/metastatic NSCLC
Pooled from 8 international RCTs 🌍
PSM cohort: 1550 pts
💊 Comparison
🟢 Early ICI <12 PM 🌅
🔵 Late ICI ≥12 PM 🌙
📊 Key results
•Median OS
➤ Early: 17.3 mo
➤ Late: 16.0 mo
•HR (late vs early): 1.04 (95% CI 0.93-1.17)
•✅ Non-inferiority met (margin 1.18)
👀 What stands out
📉 KM curves almost identical
💡 Clinical takeaway
⏰ Timing within the day is NOT a survival determinant
⚡ Real-world impact
✔️ Flexible scheduling is safe
✔️ Less pressure on morning infusion slots
📖
#OncoTwitter #MedTwitter #LungCancer #Immunotherapy @OncoAlert@myesmo@esmo_open@asco
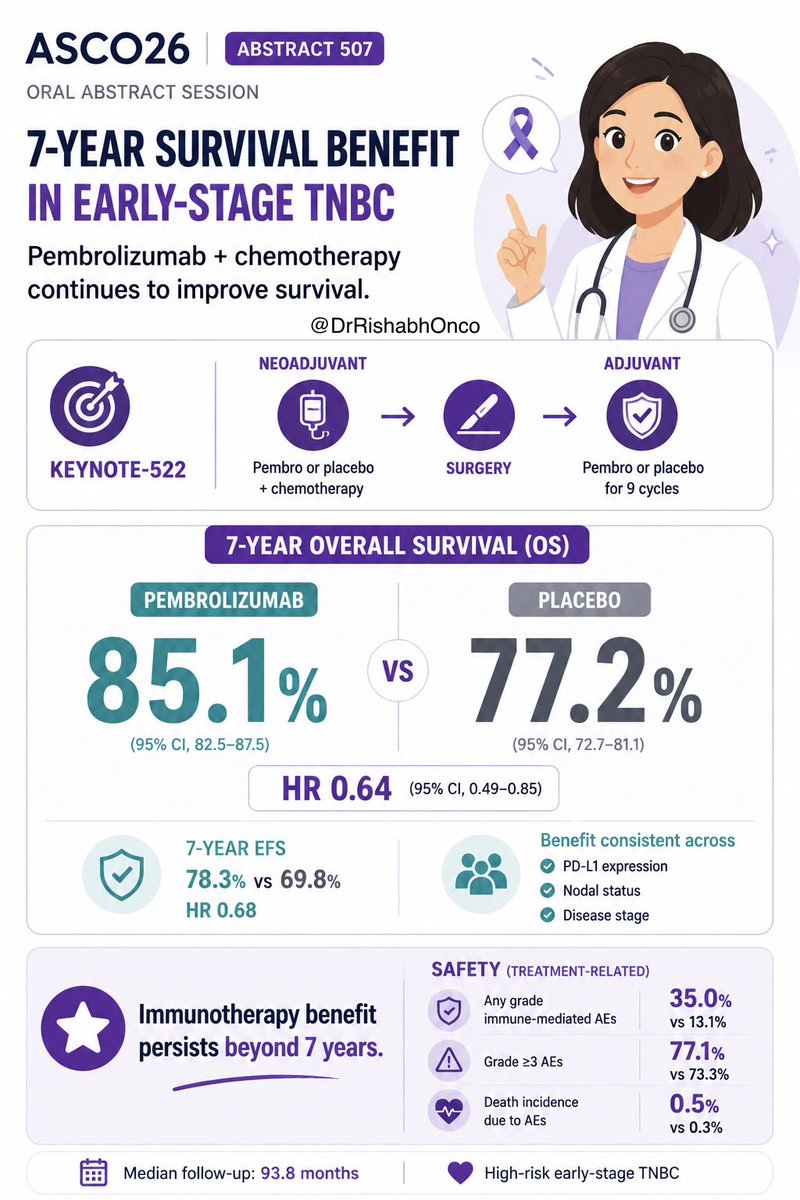
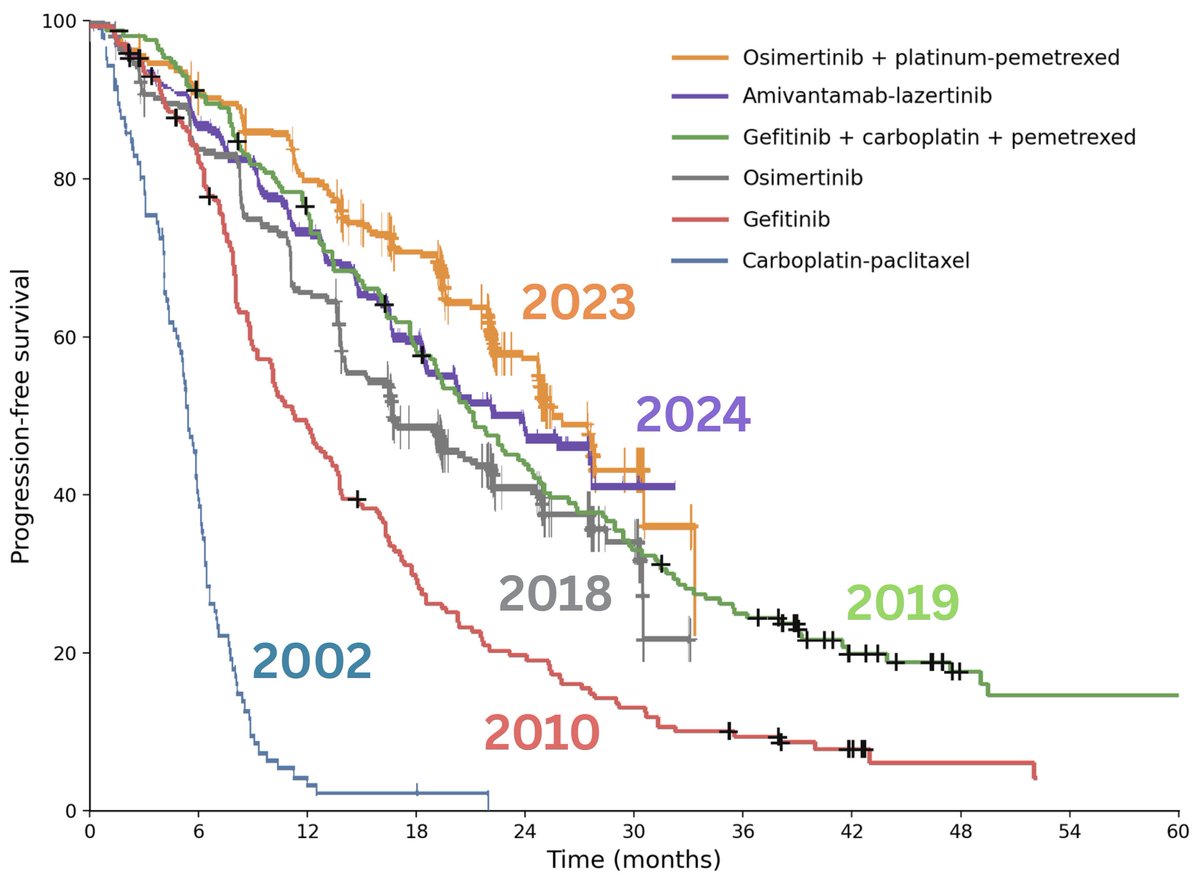
This is not just about EFS anymore.
We are finally seeing OS signals with neoadjuvant + perioperative IO in NSCLC 👀
📊 CheckMate-816 → HR 0.72
📊 KEYNOTE-671 → HR 0.74
📊 RATIONALE-315 → HR 0.65
Different strategies, different designs…
👉 same direction.
#ELCC2026@myESMO@OncoAlert@OncoReporte@MedwatchKate @MedicalwatchHQ
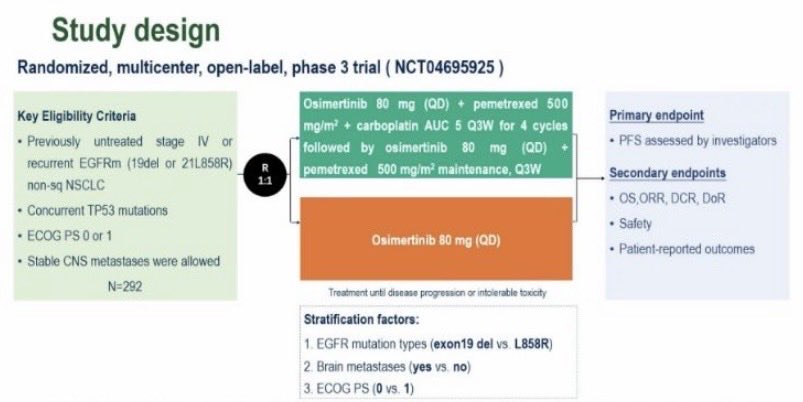
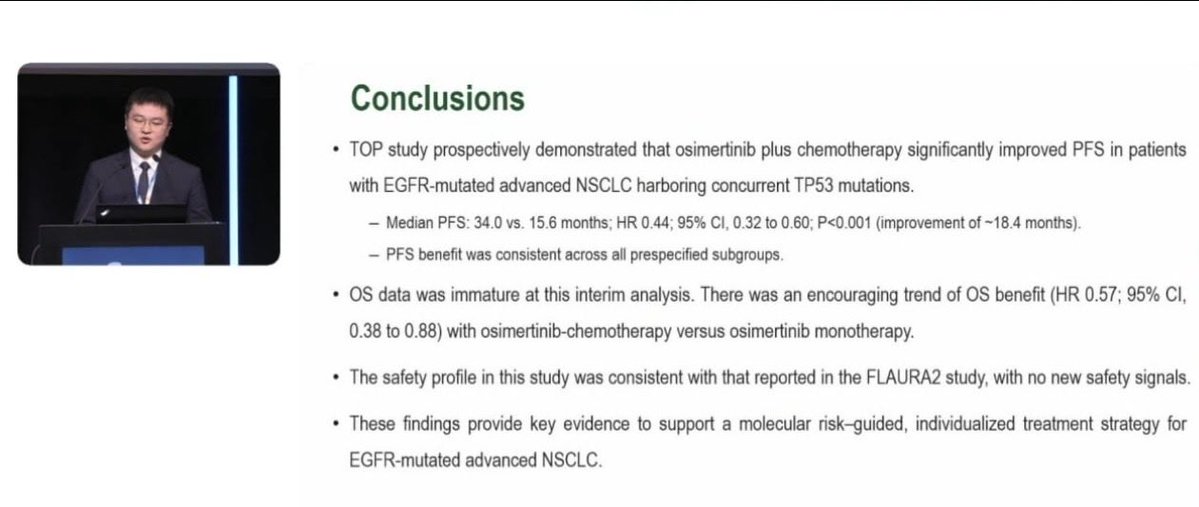
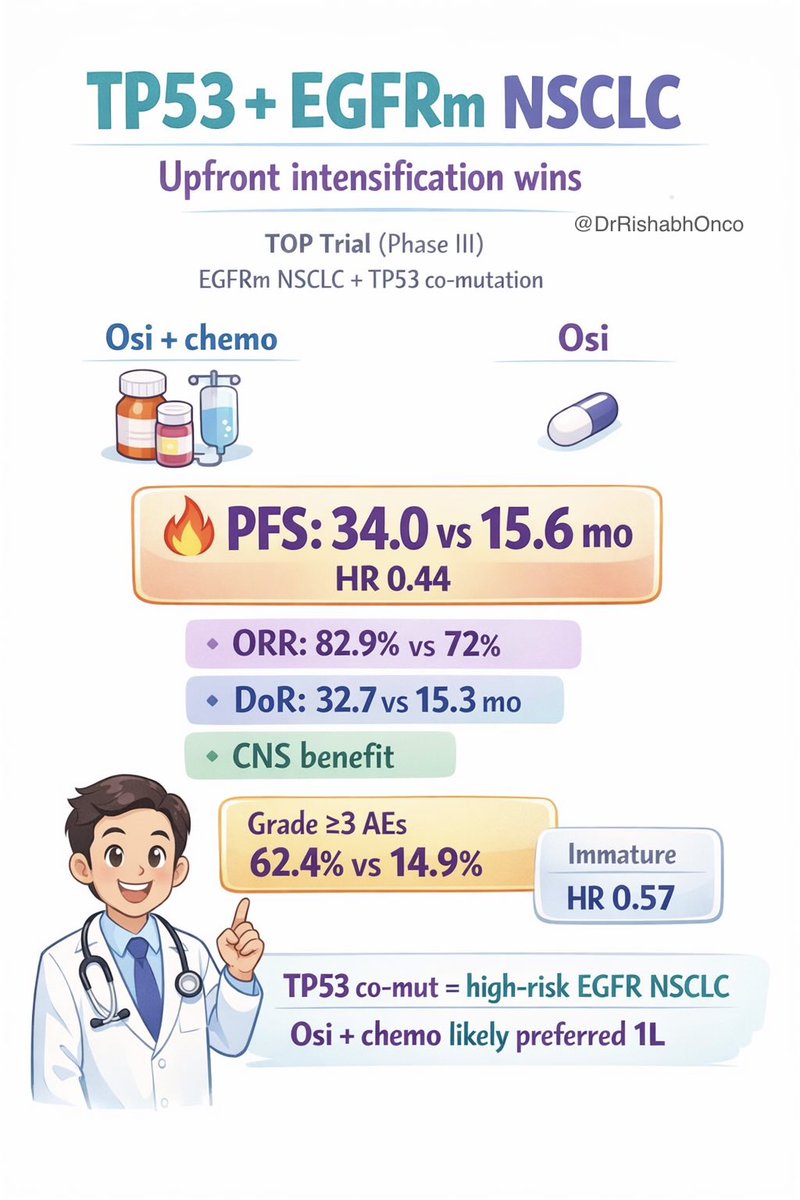
Not all EGFR NSCLC is the same… TP53 co-mutation changes the game
#ELCC26
Phase 3 TOP trial
🧬 EGFR + TP53 mutated advanced NSCLC
⚔️ Strategy tested
🟢 Osimertinib + chemo
🟠 Osimertinib alone
📊 Signal is hard to ignore
• PFS: 34.0 vs 15.6 mo
→ HR 0.44
• OS (immature):
48.4 vs 36.5 mo
→ HR 0.57
🛡️ Toxicity
Expected chemo-related ↑ modifications, no new safety flags
💡 Clinical thought
TP53 co-mut = biologically aggressive EGFR disease
👉 upfront chemo + TKI may be the better default
📖 Full paper awaited ⬇️
#LungCancer #OncoTwitter @OncoAlert@myesmo@esmo_open@ASCO@larvol
Global pooled analysis of 8 RCTs including >3000 patients shows NO impact of time of day on the efficacy of ICIs. Which is consistent with the PK and MoA of these drugs. The outlier appears to be the LungTIME-C01 trial — for which a note of caution was posted on @NatureMedicine .
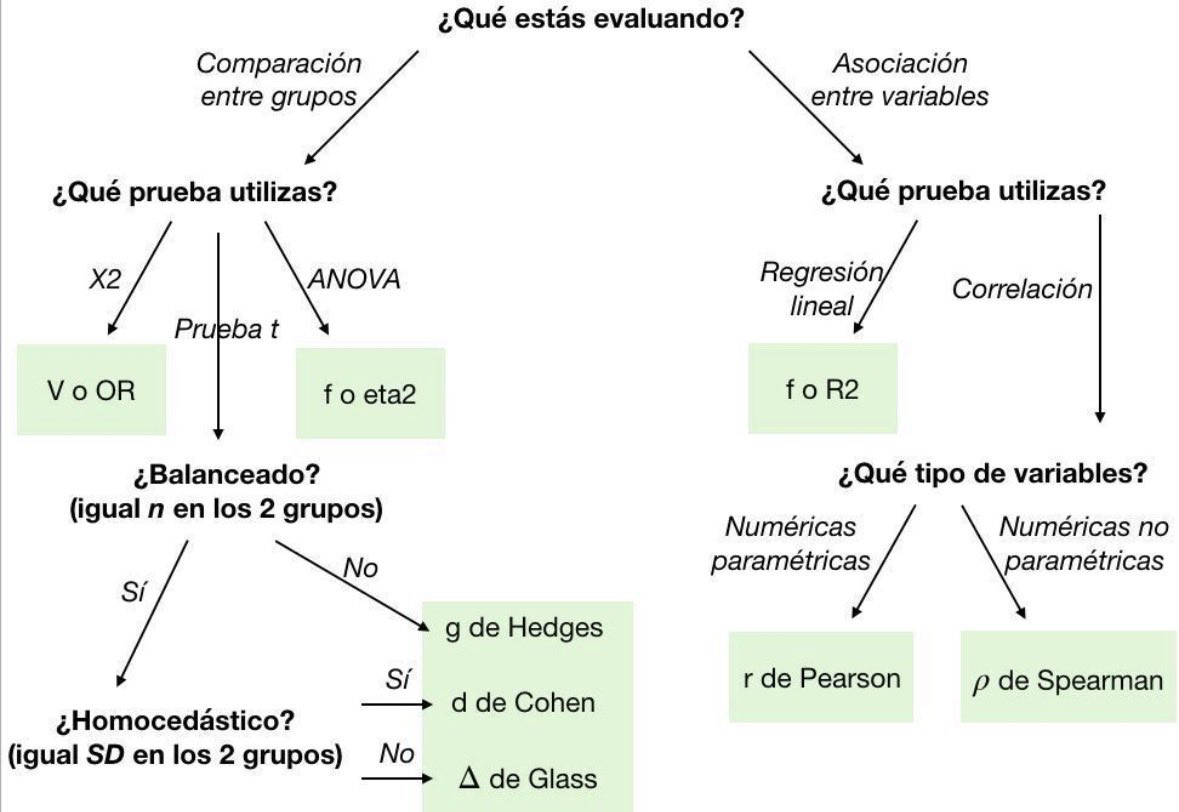
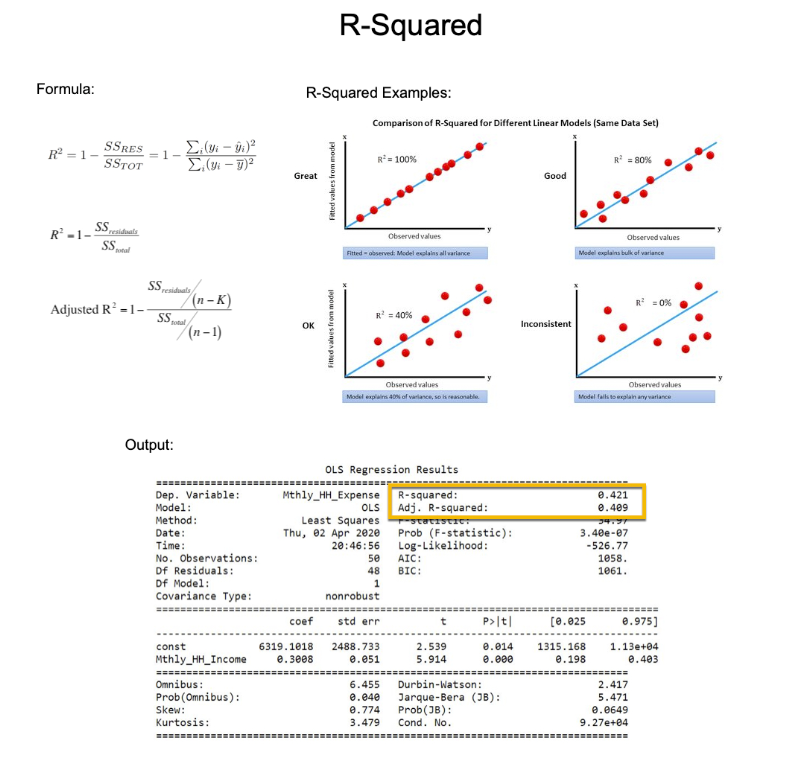
R-squared is one of the most commonly used metrics to measure performance.
But it took me 2 years to figure out the mistakes that were killing my regression models.
In 2 minutes, I'll share how I fixed 2 years of mistakes (and made 50% more accurate models than my peers). Let's go:
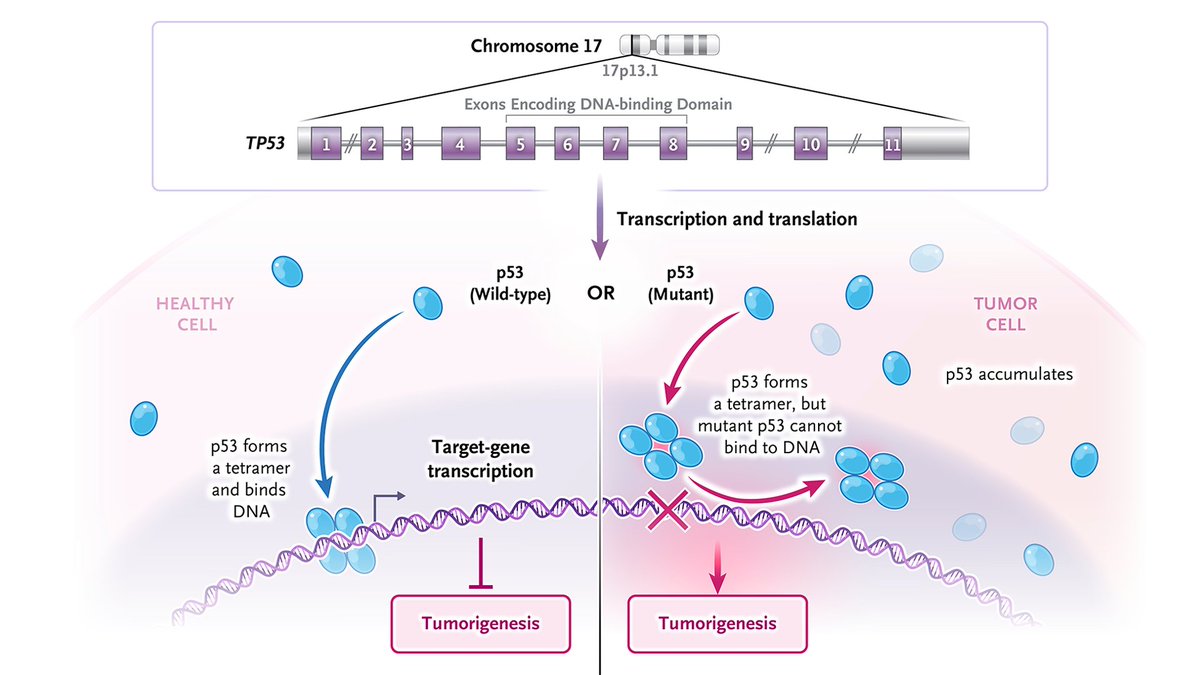
𝐓𝐏𝟓𝟑 is the gene that encodes the tumor-suppressor protein p53. It is commonly mutated in human cancers, and as with other tumor-suppressor genes, loss of function in both alleles (i.e., two "hits") is required for tumorigenesis. Wild-type p53 protein is short-lived and expressed at low levels. Mutant p53 often has an extended life span and accumulates in cancer cells. The p53 protein is a transcription factor that controls the expression of hundreds of target genes by binding and activating specific target genes that, once transcribed and translated, suppress tumorigenesis. Mutant p53 has limited or no tumor-suppressive function because it cannot bind and activate target genes.
To learn more about this NEJM Illustrated Glossary term, read the editorial “Restoring Function to a Variant of p53 in Solid Tumors” by Xin Lu, PhD, from @Ludwig_Cancer: https://t.co/5Ox6Kuax6Q
Explore more terms: https://t.co/kobNxmaQrY
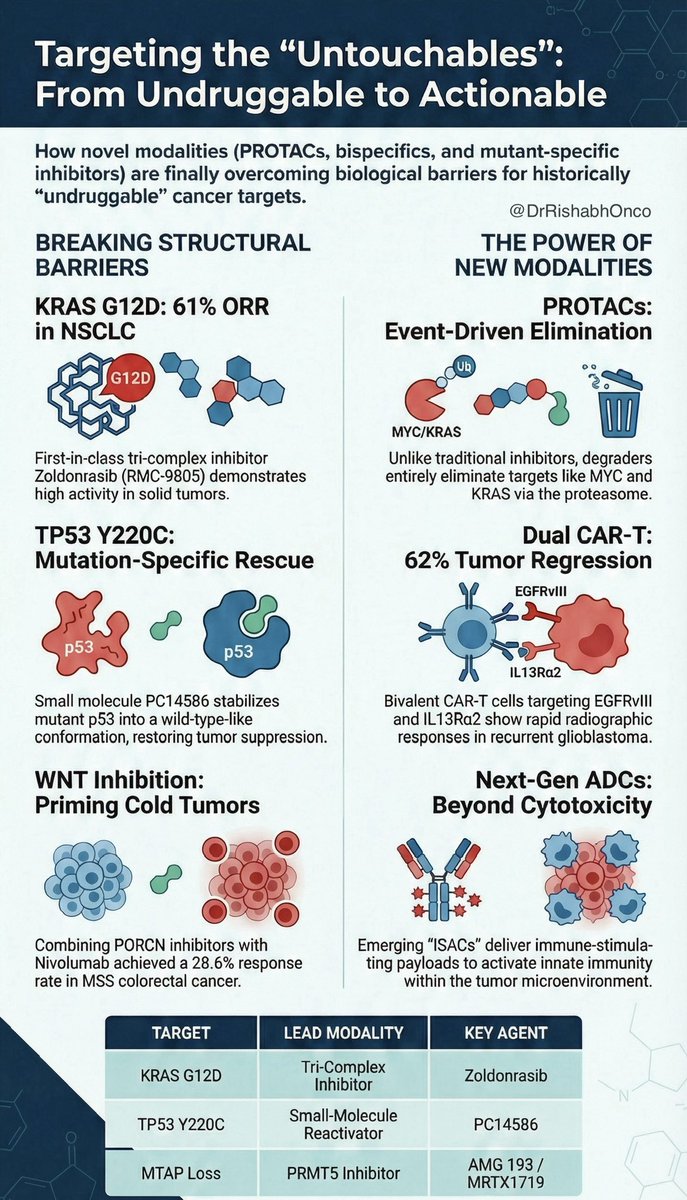
For decades, KRAS, MYC, TP53, WNT were called “undruggable.”
That era is ending.
This Annals of Oncology review shows how platform science is cracking them:
tri-complex inhibitors, PROTACs, mini-proteins, bispecific immune redirection.
🔓 KRAS G12D
Zoldonrasib (RMC-9805) shows striking early activity in NSCLC
ORR ~60% in evaluable pts, high disease control, manageable toxicity.
🧠 MYC
Still the final boss, but no longer mythical.
OMO-103 blocks MYC–MAX interaction and delivers first real proof-of-concept in humans.
🧬 TP53 & WNT
Progress is not about one magic pill.
It is mutant-specific reactivation, degradation, or smart immune targeting.
Key shift:
Precision oncology is no longer just target selection.
It is target + modality + biomarker.
🔖 Save this. The next decade of oncology drug development is being written here.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #DrugDevelopment #TargetedTherapy
@OncoAlert@myesmo@esmo_open@asco
Is it sexy? No.
Is it incredibly important for how we treat patients? Absolutely 🧠🧬
For over 20 years, 6 months of oxaliplatin plus a fluoropyrimidine has been the default for stage III colon cancer, and often high-risk stage II and rectal cancer. The cost has always been cumulative neuropathy that can follow patients for life ⚡️🖐️
The SCOT trial, the largest study in the IDEA collaboration, gives us long-term clarity with nearly 6,100 patients and more than 6 years of follow-up:
📊 5-yr DFS identical with 3 vs 6 months: 72.9% vs 72.9%
📈 5-yr OS identical: 82.4% vs 82.4%
✅ Noninferiority for OS formally met for 3 months
Where this really matters clinically:
🟢 CAPOX clearly supports 3 months
🟢 Low-risk stage III shows no OS penalty
🟡 Even high-risk disease sees only tiny absolute OS differences
⚠️ Meanwhile, neuropathy nearly doubles when oxaliplatin is extended to 6 months. Many patients pay a lifelong price for minimal benefit.
SCOT also uniquely included rectal cancer patients treated with upfront surgery, and here too, 3 months held up. This fits perfectly with modern TNT strategies 🧩
Takeaway:
This isn’t flashy, but it’s foundational. For most patients with localized colon or rectal cancer, 3 months of adjuvant CAPOX is enough. Six months should be the exception, not the rule, and always a shared decision 🤝
Sometimes the most important advance is knowing when to stop.
@OncoAlert@TheGutOncLab
#GI26
https://t.co/geX09H4ltq