🚨 STAMPEDE: AI biomarker may help select who needs abi intensification in VHR localized #prostatecancer
Just out in @Annals_Oncology
🧬 >1k pts w/ non-metastatic very high-risk PCa from 2 randomized STAMPEDE phase 3 abi trials.
🤖 Multimodal AI using routine H&E + PSA/stage/age
📉 MMAI very high-risk: abi + LT-ADT markedly improved MFS: HR 0.47. 5-yr MFS 81% vs 62%.
🎯 MMAI standard high-risk: benefit was limited: HR 0.83. 5-yr MFS 84% vs 82%. Interaction P=0.02.
🧠 Signal in both node-negative & node-positive pts
⚖️ Implication: intensify where benefit is ⬆️, spare overtreatment/toxicity where benefit is ⬇️.
🔗https://t.co/3FxTzaQumu
@PCFnews@PCF_Science@urotoday@UrologyTimes
Introducing Artemis III.
Four astronauts. Three launches. Two dockings. One splashdown.
In 2027, the Artemis III mission will practice docking the Orion spacecraft with two lunar landers in low Earth orbit — the capability we need to return humanity to the Moon’s surface.
There are 3 billion fewer birds in North America than there were in 1970.
This data is from a 2019 Science paper that combined 48 years of citizen-science bird counts with continent-wide weather radar tracking nighttime migration.
The losses are concentrated in the birds people see most often: grassland birds (down 53%, 700 million gone), forest birds (1 billion gone), and shorebirds (down 37%). Even common species (blackbirds, swallows, warblers) are vanishing.
Habitat loss is the biggest reason, but the rest of the list is short and largely fixable for the average person.
1. Pesticides killing the insects birds eat.
2. Outdoor cats kill an estimated 2.4 billion US birds annually.
3. Window collisions killing roughly a billion more. Lawn chemicals.
4. Light pollution disrupting migration.
What you can do, ranked by impact: keep cats indoors, treat your windows for bird strikes, plant native trees and shrubs, stop spraying pesticides, leave the leaves and seed heads through winter, and turn off outdoor lights at night during spring and fall migration.
No one person killed 3 billion birds, obviously, but your yard can be a part of the solution that rebuilds their numbers.
Good math, but not all quite there:
First, SpaceX pays fairly average, but for more than a decade they have offered regular (~bi-annual) liquidity to employees. To live comfortably (especially to have a family) in LA County, most employees would have sold a little bit here and there, if not a lot (e.g., if they were the sole earner in a household).
Second, critically, because there is no double trigger (in order to facilitate the liquidity), most people default to "sell-to-cover" — i.e., ~40-50% of their holdings are immediately sold to cover the taxes on vest. Remember these vests are W-2 events. In order to not do this, the employee would need to come up with significant cash (because the taxes are paid against the price at vest, not the price at grant) — especially later on.
However, two things make SpaceX particularly awesome IMO:
1. They gave employees the option to choose stock or options along the way. Someone who took options and paid the taxes with cash would have done very well.
2. They gave stock to everyone. There are a bunch of highly skilled workers that we on X never think of, like Tube Benders, Orbital Tube Welders, Cleanroom Technicians, etc. that are going to make significant fortunes.
Maybe it's overly quixotic, but this last point is underrated part of @elonmusk attacking physical problems, not just software ones, with 100x thinking: a bunch of people in the types of jobs America needs and romanticizes (for good reason) will be rewarded with the kind of wealth that really would not be possible at any other company they would have chosen.
An incredibly positive story that, if you can't see it in that light, you should look inward.
Thoughtful review of the PROTEUS trial by @DrSpratticus
First, real credit to the investigators. Pulling off a phase 3 perioperative RCT in localized prostate cancer is a massive undertaking, and easy to forget when you're critiquing from the armchair (mea culpa, I don't run trials like this).
That said, Daniel is essentially pointing out (I think 🤪) that PSMA-PET catches BCR so early that "metastasis-free survival" is really just biochemical recurrence in disguise, and EFS is a lousy surrogate for OS (see his tweetorial for the reasons).
The part that confuses me most: this isn't compared to standard of care. We don't give ADT with prostatectomy. So what are we supposed to do with this information?
https://t.co/JbdeXwbnLj
@DrSpratticus@adamkibel_uro@uretericbud@daviesbj
@urogeek@dr_coops No argument posted Dave. Was merely saying patients may avoid RP if people blindly follow that all men need 1 year of doublet tx. Yet 20% were cured in control arm…back to whole adjuvant RT story all over. Tx everyone blindingly = bad strategy.
@DrSpratticus Great analysis, Dan. Except #11. Not everything is a battle between RP and RT! :)
Real Q should be how to use correlative markers to guide high-risk ("real" high risk) patients to the right combinations of tx based on their biology and predicted oncologic and QOL response.
#ASCO26
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the placebo group)"
VERY IMPORTANTLY: "No significant between-group difference was observed in metastasis-free survival assessed with conventional imaging alone (hazard ratio, 0.84; 95% CI, 0.67 to 1.07)"
Not only does MFS cross 1, but the HR also crosses the surrogate threshold effect (0.81).
@urotoday@PCF_select@US_FDA
Congrats to Dr Taplin, all @DanaFarber_GU@DanaFarber and #PROTEUS team on a new frontier in high-risk prostate cancer.
Now officially in @NEJM !
https://t.co/36dUY9OUBN
Lets think about this.. Biologically 🧬 speaking this makes 0 sense
🇧🇷BCG is not tumor ablative ( this has been tried and failed miserably), 3 treatments (78% of pt) & we know maintenance is critical
⚽️pCR 68% is huge leap from previous GC+atezo alone(pCR 41% w/o rBCG (without n1)...
and lets not forget 11% of this cohort was N1 and majority not fully resected. The results are provocative but I would love to see this replicated ( I am keeping an open mind)
some reads >> pCR 41% with GC atezo https://t.co/AmEBOIO0GU
BCG in mibc> https://t.co/vtBGJs9PuY
Can genomic data, not just PSA or MRI, guide your next prostate cancer treatment plan? Dr. Ruchika Talwar and Dr. Udit Singhal discuss biomarker tests and how they can supplement traditional testing strategies to reveal hidden molecular heterogeneity, inform prognosis, and predict treatment response in real-world practice.
Watch the full episode here:
https://t.co/nR1WgrGbIM
This podcast is supported by Veracyte.
#URO301 #ProstateCancer #Biomarkers #GenomicTesting
Hospital prices have skyrocketed 281% over the past 25 years; outpacing inflation, wages, housing, and childcare.
Meanwhile, government distortions like 340B abuse, provider tax schemes, and bans on physician-owned hospitals have weakened competition and driven up costs for taxpayers.
https://t.co/Li68MpIUk0
⚡️ Phase 3 KEYNOTE-B15/EV-304 at #ASCO26: perioperative EV + pembrolizumab vs gemcitabine/cisplatin in cisplatin-eligible MIBC.
EFS HR 0.53. pCR 55.8% vs 32.5%. OS HR 0.65.
First regimen in 25 years to surpass cisplatin-based neoadjuvant chemotherapy in MIBC.
@mattgalsky@ASCO #BladderCancer
https://t.co/7zGdhVKvdD
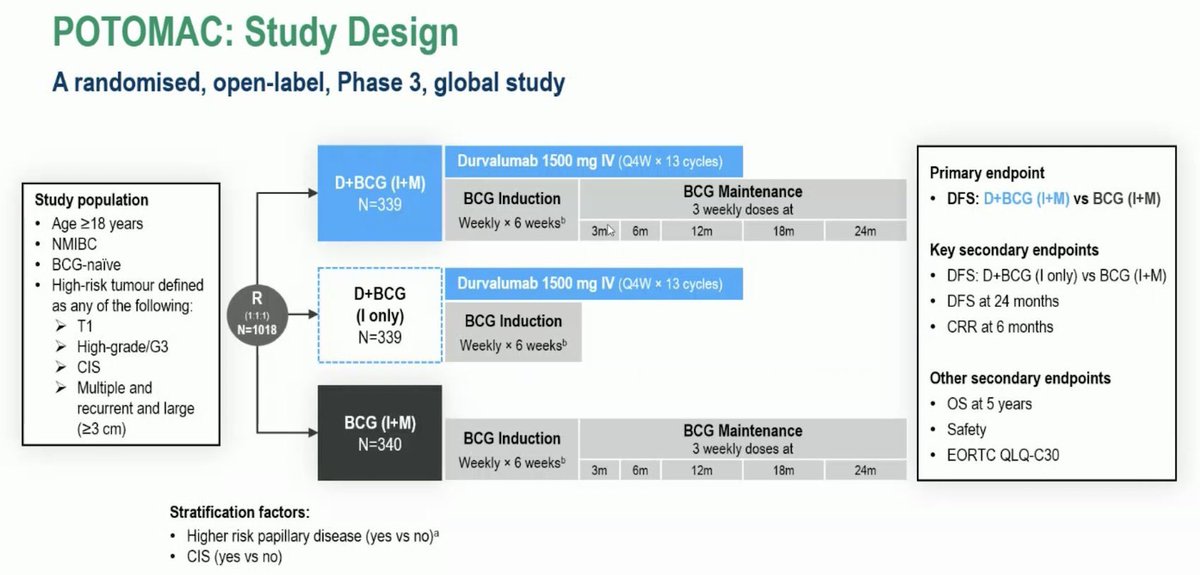
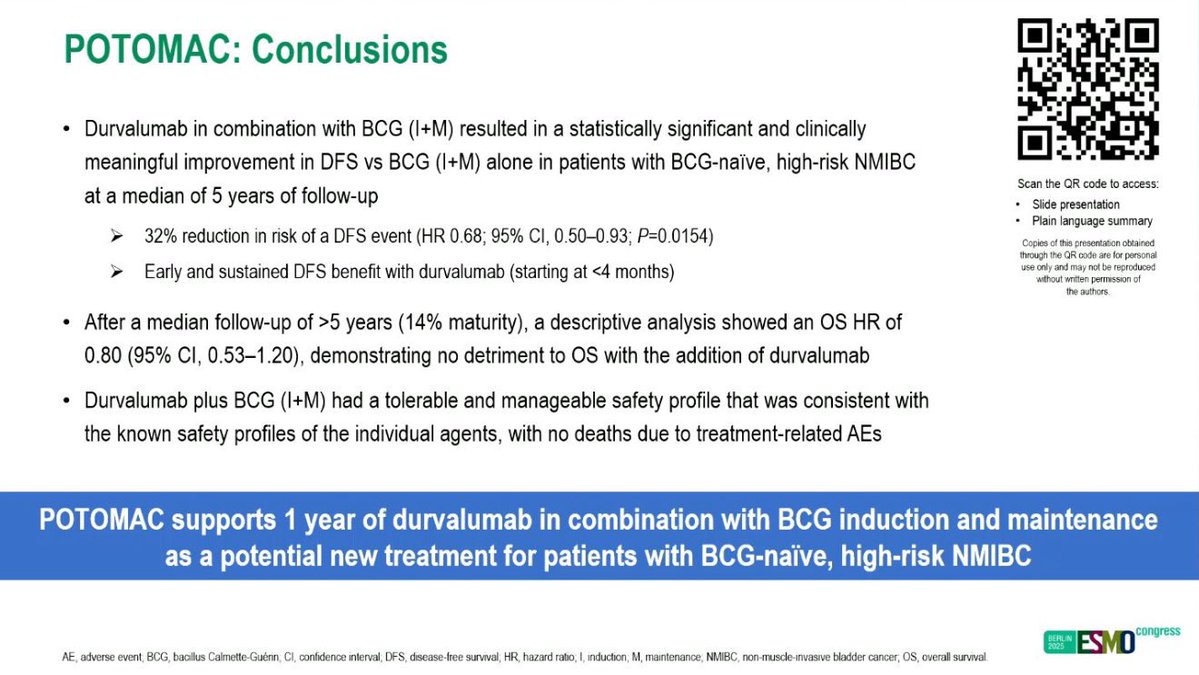
Durvalumab now @US_FDA ✅ for Non-Muscle Invasive Bladder cancer based off #POTOMAC: PhIII, BCG + Durvalumab vs. BCG alone in BCG naive HR-NMIBC:
- DFS waiting maturity (HR: 0.68)
- 3yr mDFS 82% vs 77%
- MedOncs will now see HR-NMIBC
#gusm#OncTwitter
Really like this Cell paper from Stanford group - TURBT results in molecular clearance in 39% NMIBC. And those patients do really well. Lots of good stuff in the paper... non-molecular responders could get new agent earlier, not just maintenance BCG
https://t.co/xfpYbbZZIX
Insurance companies’ ownership of pharmacies and hospitals is raising consumer costs, but economic competition can counter inflating expenses, according to bipartisan legislation from Sens. Josh Hawley, R-Missouri, and Elizabeth Warren, D-Massachusetts.
“We need more competition. We need protections for patients. We need better and cheaper health care,” Hawley told The Lion in an exclusive interview Thursday.
Hawley and Warren reintroduced The Patients Before Monopolies Act last week to counter the monopolized medical field, in step with their second bipartisan bill, The Break Up Big Medicine Act. The Patients Before Monopolies Act prohibits pharmacy benefit managers (PBMs), the middlemen between pharmacies and insurance companies, from owning pharmacies and hospitals, Hawley explained.
“What’s happening is more and more of these insurance companies are buying up everything,” Hawley told The Lion. “They’re buying up the pharmacies. They’re buying up the doctor’s offices. They’re buying up the hospitals.”
@HawleyMO
Read full story: https://t.co/XqTHsgh1mD