بصفتي مدير برنامج زمالة أمراض الجهاز الهضمي في مستشفى الملك فيصل التخصصي ومركز الأبحاث، أفخر بهذا الإنجاز التاريخي.
بعد تقديم 25 ورقة بحثية من أطباء الزمالة في مؤتمر أسبوع أمراض الجهاز الهضمي 2026 في شيكاغو، تم قبول 25 ورقة بحثية أخرى لهم لتقدم في المؤتمر السنوي للكلية الأمريكية لأمراض الجهاز الهضمي 2026 في ناشفيل، ليصل إجمالي الأوراق البحثية المقدمة هذا العام إلى ٥٠ ورقة بحثية من برنامج التخصصي بالرياض في اكبر المؤتمرات العلمية.
هذا الرقم من الابحاث للمتدربين هو الأعلى في تاريخ برامج زمالة الجهاز الهضمي في منطقه الشرق الاوسط، ويؤكد أن مستقبل التخصص في المملكة واعد بفضل طموح أطباء الزمالة وتميزهم.
الوافد مكسب قصير المدى لسوق العمل ، لكنه لا يصنع اقتصادًا مستدامًا وحده. التوازن الصحيح يكون بربط استقدامه بنقل معرفة حقيقي، وتكلفة عادلة، ومسار واضح لإحلال الكفاءة الوطنية دون تعطيل لسوق العمل .
@atmghn Great thread.. How do you determine early on that the anterior-only approach won’t hold? Are you looking for early fusion signs? Or hardware issues? Do you follow these patients differently than your other degen cases? Does the same apply for two-level corpectomy?
One of the hardest calls we’ve made as a team… placing a venous sinus stent in an 18mo w/ vein of Galen malformation. Very rarely described option.
Life saving neonatal embo → normal milestones → progressive 1-sided transverse sinus thrombosis → brainstem congestion, drop in mobility and consciousness.
Urgent angio > Multiple high flow AV shunts = not possible to embo in one stage. Only way to buy time → venous stent. Restored flow → less congestion → child improved + went home.
Proud to be part of this amazing team.
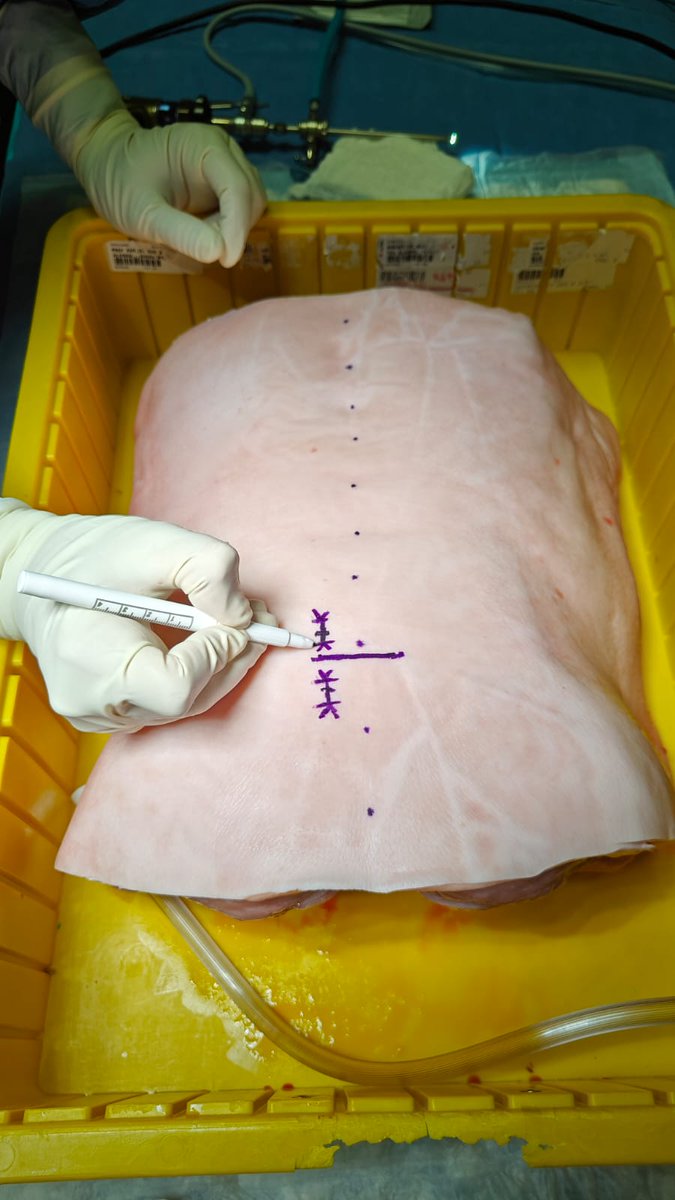
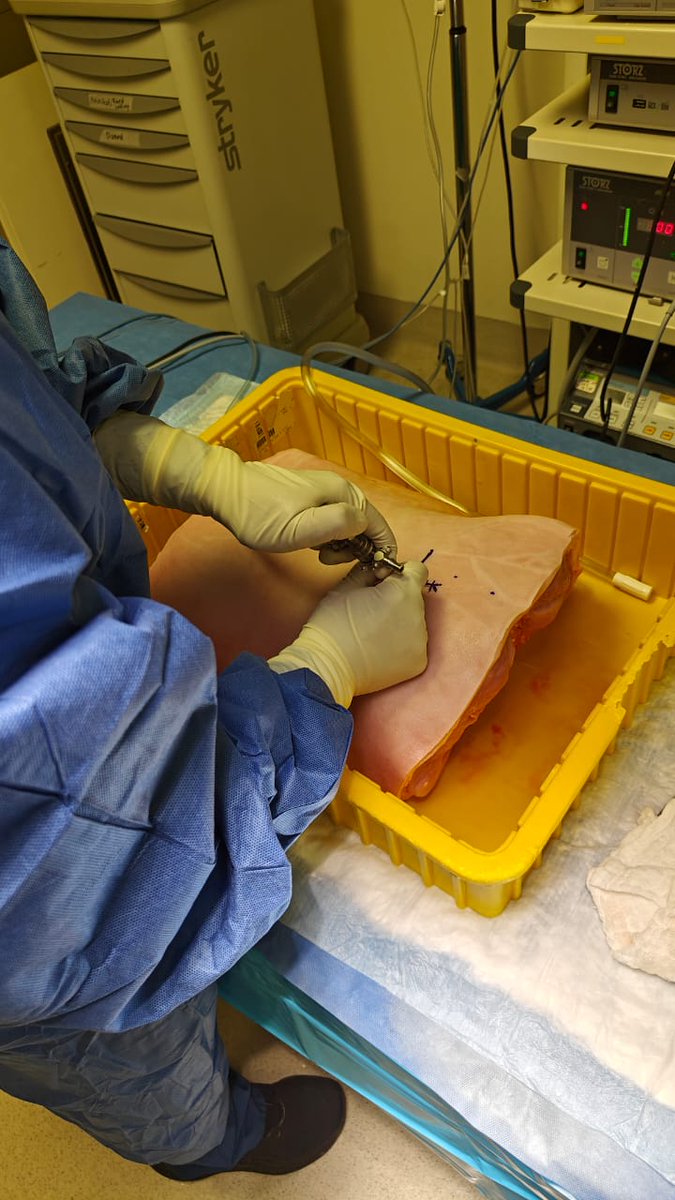
Endoscopic spine surgery is a field with tremendous potential, but also a steep learning curve. One way to bridge that gap is through simulation outside the O.R.
Over the past few weeks, I was able to practice Unilateral Biportal Endoscopy (UBE) using ex vivo porcelain models. I found these models to be an excellent platform for practicing triangulation, drilling, and decompression techniques in a controlled and reproducible way. They offer valuable realism and haptic tissue feedback. Despite some anatomical differences, they provide a cost-effective alternative to cadaveric labs.
The more we innovate in simulation, the better we can prepare the next generation of spine surgeons for safe and effective endoscopic practice.
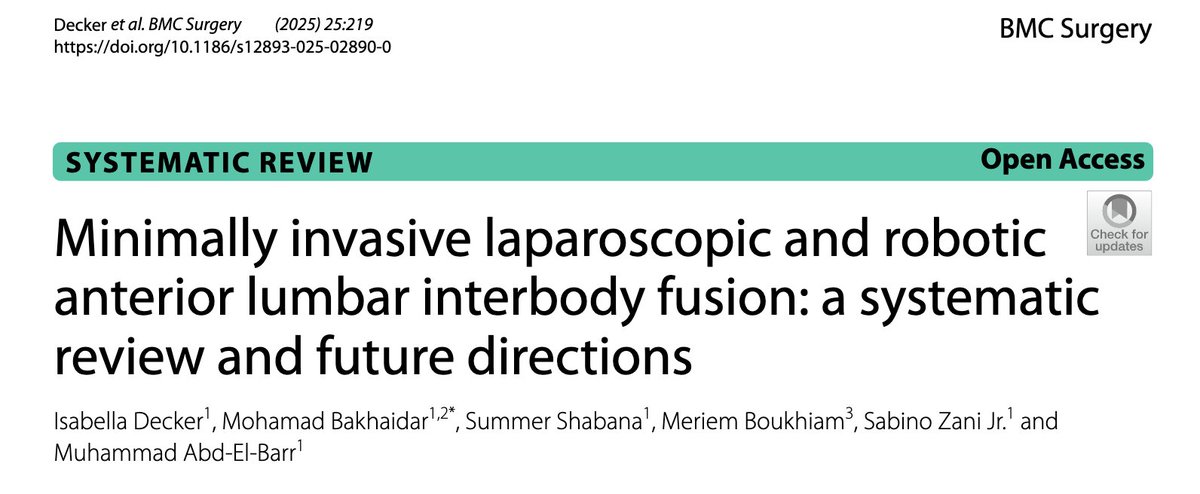
New pub:
https://t.co/0pLd6oORXv
Minimally invasive laparoscopic and robotic
anterior lumbar interbody fusion.
In quest to minimize the ‘surgical footprint’, these techniques may help.
@DukeMedSchool Isa Decker
@MBakhaidar , Summer Shabana, Meriem Boukhiam, Sabino Zani
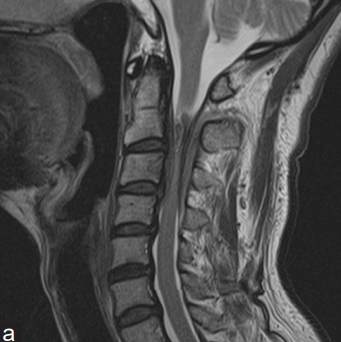
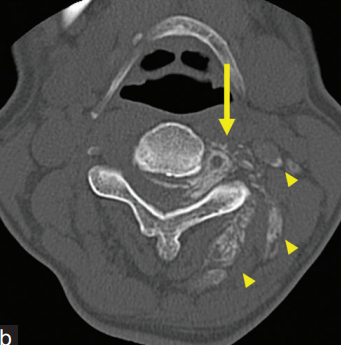
🧔♂️51-year-old woman with progressive limb weakness and sensory deficits over six months.
😣Symptoms worsened to the point of impaired fine motor skills and spastic gait.
🕵️♂️What’s your diagnosis?
من اسباب عدم الرضى بنتائج الاجراءات الجراحية هي عدم توضيح النتائج المتوقعة من الطبيب المعالج. عندما تجري عملية وتتوقع النتيجة تكون ١٠٠٪ وتطلع ٩٥٪ تركيز المريض دائما يكون على ال٥٪ المفقودة. لكن إذا كان الشرح واضح ان النتيجة غالبا بتكون ٩٥٪ رضى المريض قد يصل إلى ١٠٠٪. وصلت الفكرة؟
Spinal aneurysmal bone cyst ABC; sclerotherapy, RF ablation, and filling with bone graft substitute. Faint epidural contrast (epidural block), allows for same day discharge with minimal pain.
I encourage anyone interested in new advances in spine surgery to join us at the Bass symposium (live or remotely) on March 1st. Talks will appeal to hospital employees, LVNs, RNs, and a full spectrum of residents and physicians from primary care to surgery.@UTSWMedCenter @utswspine
Building a Spine Program: Lessons from My Journey in Employed & Private Practice
I’ve learned the hard way that the biggest mistakes happen when surgeons defer responsibility or ownership and focus on the wrong things too soon.
The key to success?
Be incremental, Build the right team, optimize workflows, and scale only when demand supports it.
1️⃣ Build the Right Team First—Everything Else Depends on It
Your team determines your efficiency, surgical outcomes, and growth potential.
🔹 Clinical & Office Team: PA/NP for clinic & surgery, MAs for efficiency, a surgical coordinator to optimize OR scheduling, and a billing/coding expert (critical for private practice).
🔹 OR Team: A consistent scrub tech, a skilled first assist, and anesthesia that understands spine cases are game-changers for surgical efficiency.
🔹a strong relationship with the specialty coordinator is vital to navigate things like th VAC committee and bringing in new products
2️⃣ Optimize Clinic & OR Workflows Before Expanding
A practice that runs smoothly will always outpace one that just looks impressive on paper.
✅ Same-day consults build referral loyalty.
✅ Telemedicine follow-ups improve efficiency.
✅ Standardized pre-op/post-op protocols reduce cancellations and complications.
3️⃣ Build Referral & Direct-to-Patient Pipelines Before Investing in Expansion
A fancy office means nothing if your referral stream is weak.
✅ Primary Care & Pain Specialists are your biggest referral sources—build those relationships.
✅ Physical Therapists & Chiropractors trust surgeons who respect conservative care first.
✅ SEO, Google Reviews & LinkedIn Presence matter—patients research their spine surgeon before booking.
4️⃣ Delay Heavy Capital Investments Until Demand Supports It
The biggest mistake?
Spending on expansion too early. Each capital expenditure is political and financial influence spent.
Only invest when the probability of meaningful return is high.
5️⃣ Financial Optimization Is the Difference Between Thriving and Struggling
Spine surgery is high-reimbursement—if you’re doing it right.
Whether private or employed take the time to understand the finances…
✅ Negotiate payer contracts to maximize collections.
✅ Monitor denial rates & revenue cycle KPIs—leaving money on the table is common.
✅ Offer cash-pay models—many high-deductible patients prefer transparent pricing.
6️⃣ Expand Only When Patient Volume Justifies It
Once your team, workflows, and referral base are strong, then consider growth.
✅ More office space? Only if you’re at capacity.
✅ ASC investment? When outpatient case volume supports ownership.
✅ Ancillary services (MRI, PT, Biologics, DME)? When it’s financially beneficial to bring them in-house.
💡 Key Takeaways from My Experience
✅ Your team is your foundation—build it first.
✅ Optimize patient flow before adding services.
✅ Develop strong referral & marketing systems before expanding.
✅ Delay big investments until the numbers justify them.
I’ve learned this through experience—the wins, the failures, and the lessons in between.
Amazing 3 days @SaudiSpine Society!Impressed with young spine surgeons’ thirst for knowledge- that’s what keeps me young:)
Shared work on machine learning for the triage of patients @ChristineGoertz@AndreasSeas
AI session with Drs. Ahmed Aoude,Zeeshan Sardar,Mai Aldera.
Honored to have presented our work on simulators at @CNS_Update. So grateful to @MBakhaidar and @SamShabaniMD for their exceptional mentorship and support!
#OnlineFirst: Do expandable cage size and number of cages matter in transforaminal lumbar interbody fusion at L5–S1? A comparative biomechanical analysis using finite element modeling. https://t.co/YPzjHpJtoE
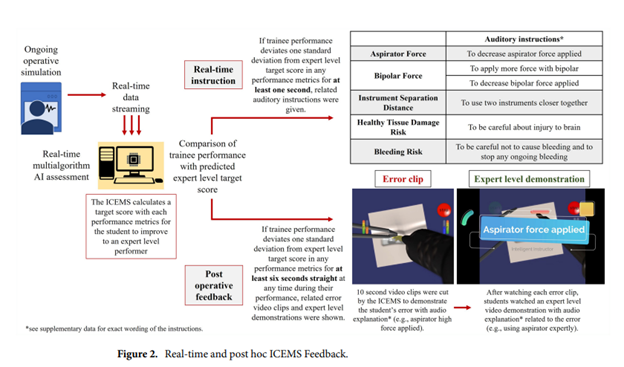
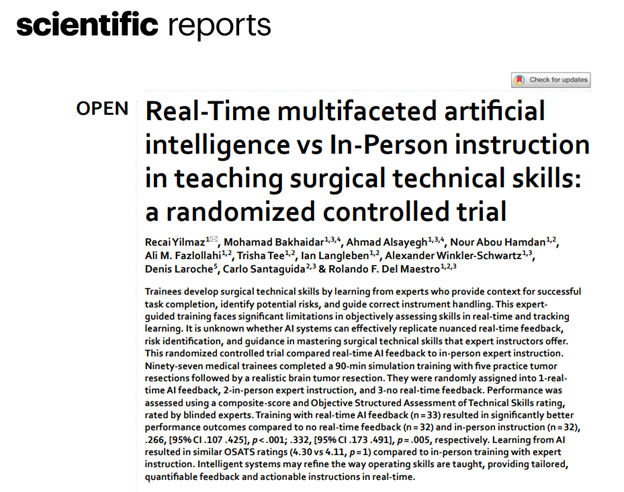
@AI_SimCentre congratulates co-authors for their article entitled:Real‑Time multifaceted artificial intelligence vs In‑Person instruction in teaching surgical technical skills: a randomized controlled trial just published in Nature Scientific Reports.
10.1038/s41598-024-65716-8
Great anatomic tips for T1 freehand pedicle screw technique @CAS_Spine published now @NeurosurgeryCNS: Midpoint of C7 Lateral Mass Serves as an Accurate Reference for T1 screws. I use a similar technique allowing T1 to easily line up with cervical screws.
@CNS_Update@DKondziolkaCNS
https://t.co/7V3VkNNtb7
Outstanding presentation by @SamShabaniMD on tractography, U/S, and SCI! An exciting peek into the future of their application in SCI research.
@MCWNeurosurgery@spinesection