🧬 T-Cell Fitness vs T-Cell Exhaustion
⚖️ Tumor Biology vs Immune Biology
For decades, we focused on the cancer cell.
Perhaps the next frontier is the T cell.
Cancer cells are smart. They evolve, mutate, and develop multiple escape mechanisms.
But disease progression may not simply reflect tumor growth.
It may reflect failure of durable immune surveillance.
T-cell redirecting therapies have taught us an important lesson:
🧬 Not all T cells are created equal.
A fit T cell expands, persists, and maintains immune control.
An exhausted T cell may still recognize cancer, but lacks durability.
Perhaps the next frontier is not simply Tumor Biology.
Perhaps it is Tumor Biology + Immune Biology.
The goal is not just to kill cancer.
The goal is to build an immune system capable of controlling it.
In Biology We Trust.
👇 More to see in the figure.
#myeloma #lymphoma #CART
During induction chemo for AML, why do we give continuous IV cytarabine, instead of bolus dosing like in consolidation?
Cytarabine is a pyrimidine analog that inhibits DNA synthesis. The chemo kills cells that are undergoing active DNA replication, making cytarabine "S-phase specific". But leukemia cells are constantly in flux in the cell cycle. They are not all uniformly in the same cell cycle phase. In active AML, leukemia blasts are slowly entering S phase over days, and cell kill is enhanced when they are getting continuously exposed to IV cytarabine
Once patients achieve remission, we do high dose bolus cytarabine to consolidate that remission. Bolus dosing generates high peak plasma concentrations and elevated intracellular levels of cytarabine metabolites (Ara-CTP) to overwhelm resistance mechanisms that characterize residual AML. Bolus dosing produces high peak concentrations, but exposure is transient as plasma cytarabine has a short half life (10-15 min) due to rapid deamination
So continuous IV yields low peak concentrations but prolonged duration above effective concentration, vice versa for bolus.
Effectively, one should think of continuous IV and bolus dose cytarabine as TWO DIFFERENT DRUGS WITH RADICALLY DIFFERENT MECHANISMS OF ACTION!
Administration of IV iron therapy during acute infections was associated with improved 14- and 90-day survival #hematology@BloodPortfolio@CAMCHemOncIAM https://t.co/X7ad8vDvyl
PFS is not always OS.
One of the biggest misconceptions in oncology is assuming that delaying progression automatically means patients live longer.
Many strategies consistently improve:
• PFS
• depth of response
• MRD negativity
…but OS often barely moves.
Examples:
• Upfront vs delayed AutoSCT
• Lenalidomide maintenance
• HD melphalan intensification
• Many maintenance strategies in lymphoma
Why?
Because:
• crossover therapies matter
• salvage therapies work
• toxicity matters
• resistant clones survive
• biology evolves
A longer remission is meaningful.
But it is not always a longer life.
The critical question is no longer:
“Did the curve separate?”
The question is:
“What happened to OS?”
#MultipleMyeloma #lymphoma #CART #Hemtwitter
Dr. Fun + G
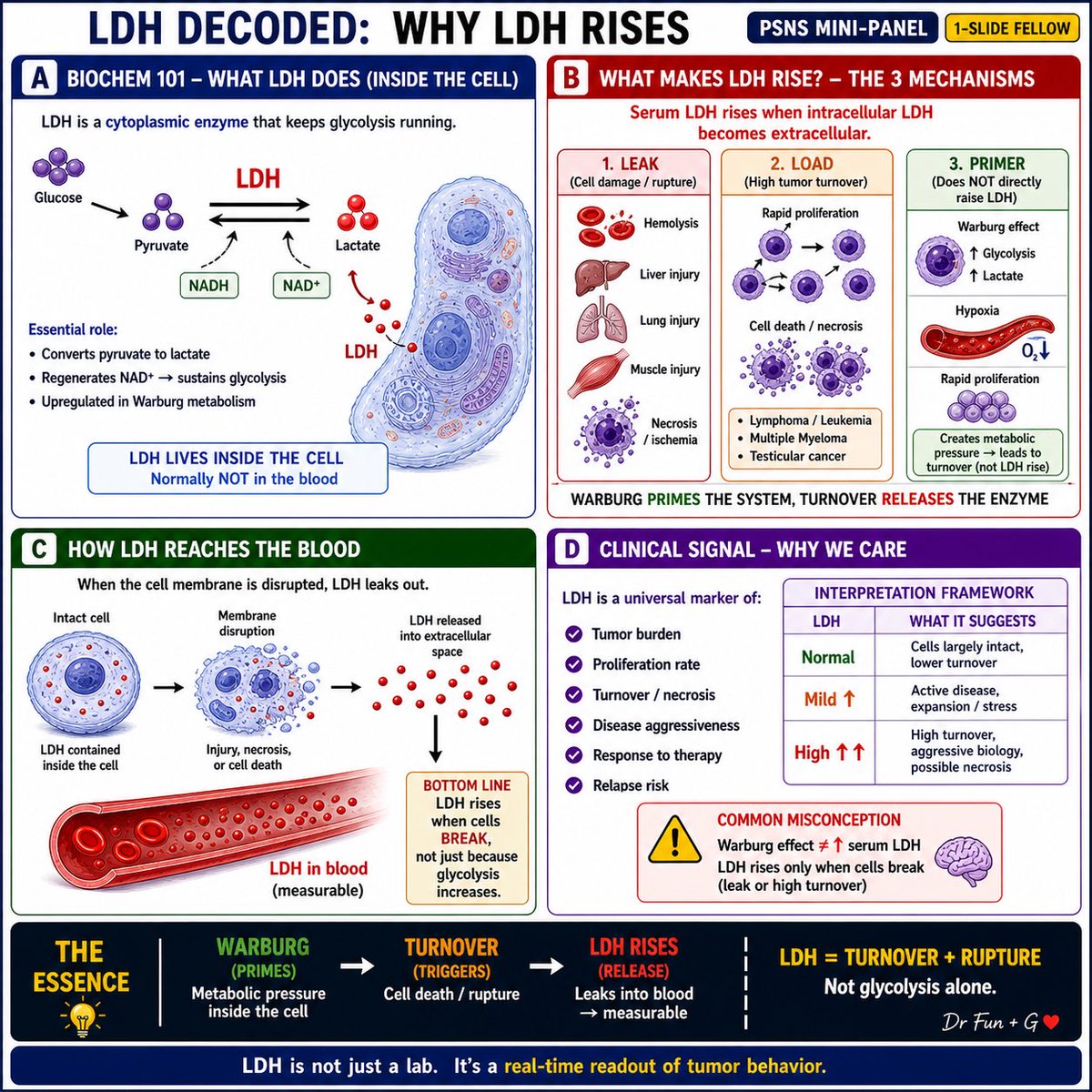
Why we obsess over LDH?
Because it shows what the tumor is doing right now.
Not mutation
Not pathway
Behavior.
↑ LDH = turnover + cell death
Warburg ≠ serum LDH
LDH = leak + load
✍️ Dr Fun + G
#myeloma#lymphoma#Hemetwitter
كان الروس في الحرب العالمية الثانية ينشدون أنشودة تقول:
إذا فقد الجندي ساقيه في الحرب، يستطيع معانقة الأصدقاء.
إذا فقد يديه، يستطيع الرقص في الأفراح.
وإذا فقد عينيه، يستطيع سماع موسيقى الوطن.
وإذا فقد سمعه، يستطيع التمتع برؤية الأحبة.
وإذا فقد الإنسان كل شيء، يستطيع الاستلقاء على أرض وطنه.
أما إذا فقد أرض وطنه .. فماذا بمقدوره أن يفعل ؟
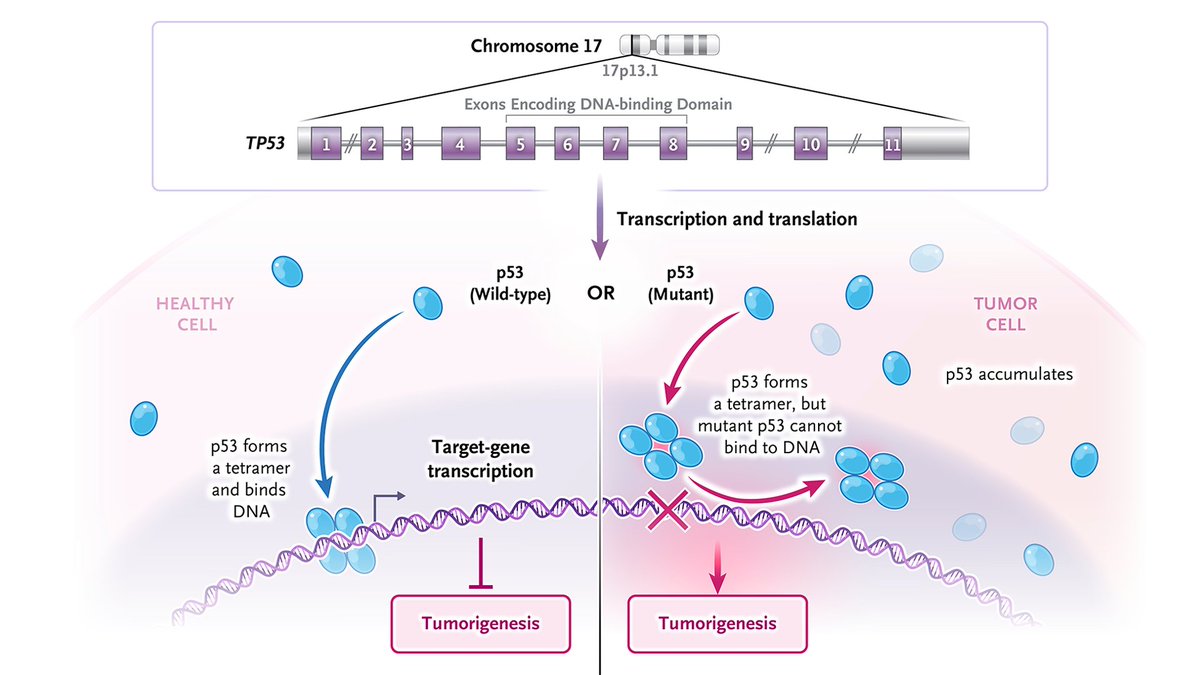
𝐓𝐏𝟓𝟑 is the gene that encodes the tumor-suppressor protein p53. It is commonly mutated in human cancers, and as with other tumor-suppressor genes, loss of function in both alleles (i.e., two "hits") is required for tumorigenesis. Wild-type p53 protein is short-lived and expressed at low levels. Mutant p53 often has an extended life span and accumulates in cancer cells. The p53 protein is a transcription factor that controls the expression of hundreds of target genes by binding and activating specific target genes that, once transcribed and translated, suppress tumorigenesis. Mutant p53 has limited or no tumor-suppressive function because it cannot bind and activate target genes.
To learn more about this NEJM Illustrated Glossary term, read the editorial “Restoring Function to a Variant of p53 in Solid Tumors” by Xin Lu, PhD, from @Ludwig_Cancer: https://t.co/5Ox6Kuax6Q
Explore more terms: https://t.co/kobNxmaQrY