A high CK is not the diagnosis.
It is only the entry ticket.
Inflammatory myopathy should be approached by pattern first, not by calling everything polymyositis.
First, look at the weakness.
Slow, asymmetric weakness with finger flexor and quadriceps involvement
Think inclusion body myositis.
Rapid proximal weakness with a CK volcano
Think immune mediated necrotizing myopathy, especially anti HMGCR or anti SRP.
Subacute proximal weakness with mechanic’s hands, Raynaud’s, arthritis or ILD
Think antisynthetase syndrome, especially anti Jo 1, PL 7 or PL 12.
Rash with or without weakness, sometimes even with normal CK
Think dermatomyositis, especially MDA5, TIF1 gamma, NXP2, Mi 2 or SAE.
Antibodies are powerful, but only when the phenotype agrees.
MRI tells you activity versus damage.
Biopsy still matters in seronegative cases, suspected IBM, poor steroid response or dystrophy mimics.
The real mistake is stopping at muscle.
Always ask about:
lung, skin, swallow, heart and cancer risk.
Myositis is not one disease.
It is a pattern recognition exam where the wrong lane can cost muscle, lung and time.
Pattern first.
Antibody next.
Biopsy when needed.
Screen beyond muscle.
Treat the subtype, not the CK.
#Neurotwitter #Medtwitter
Source: Allenbach Y, Benveniste O. Inflammatory Myopathies. NEJM, 2026.
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
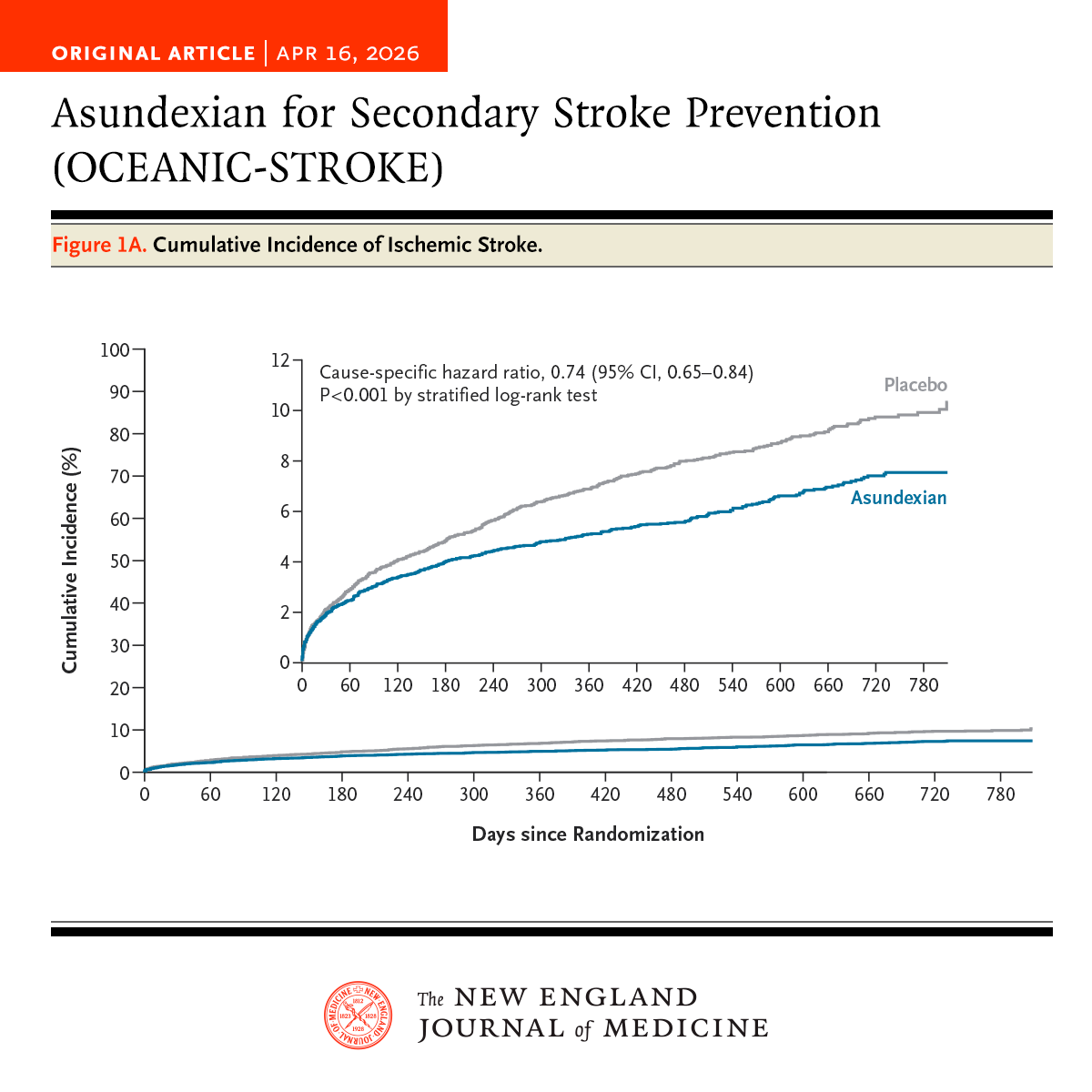
In the phase 3 OCEANIC-STROKE trial involving patients with noncardioembolic ischemic stroke or high-risk TIA, asundexian added to antiplatelet therapy led to a lower risk of ischemic stroke without increasing major bleeding. Full trial results: https://t.co/UPJGedYXFe
Editorial: Asundexian for Noncardioembolic Ischemic Stroke https://t.co/V1dVNbx4T8