🔬 PEACE 2 phase III: Adding pelvic RT to prostate RT + 3y ADT in very high-risk localized prostate cancer did NOT improve bPFS, MFS, CSS or OS. Borderline cPFS signal (HR 0.81, p=0.09). No added AEs. @PBlanchard_MD #ESTRO2026. @VedangMurthy what now?
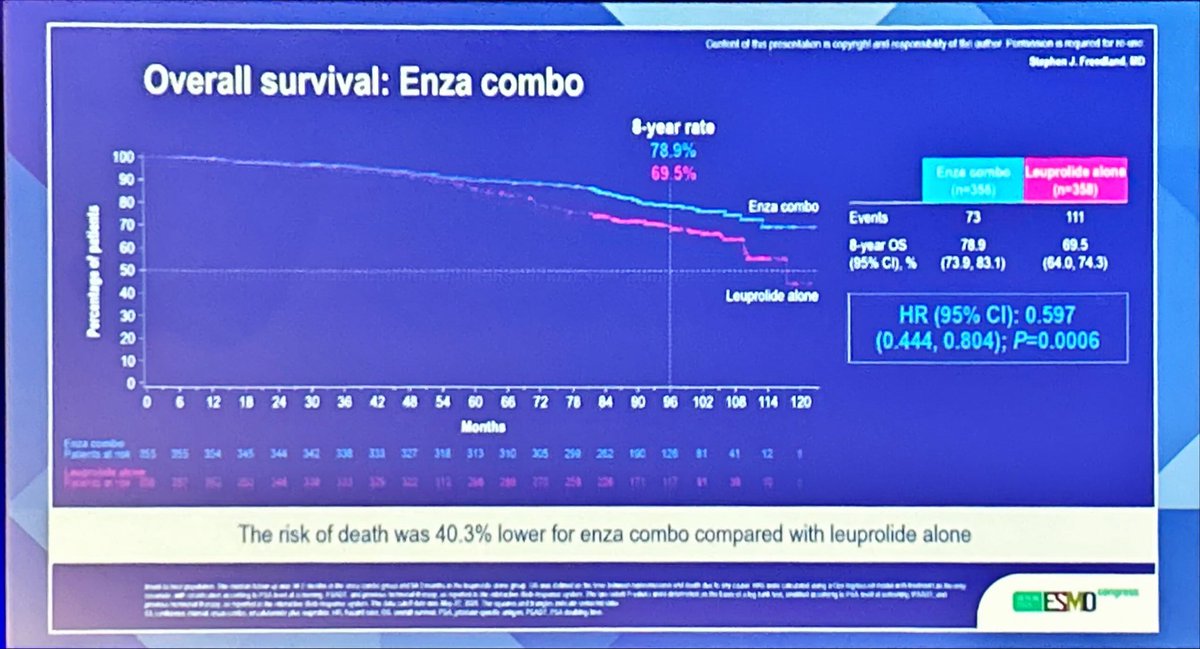
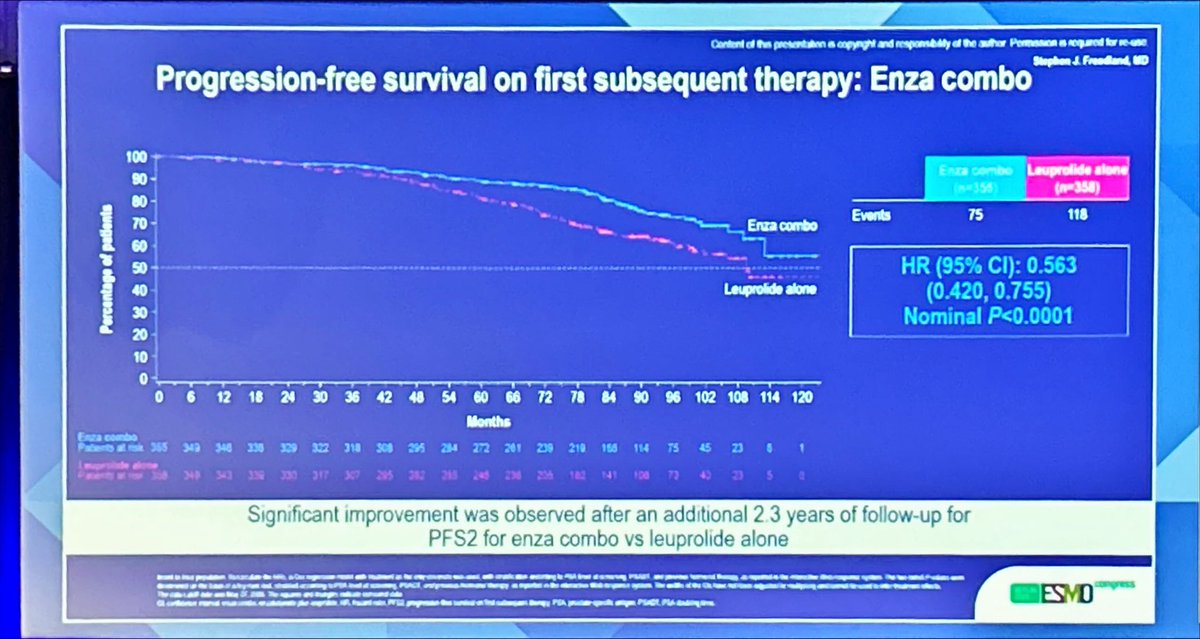
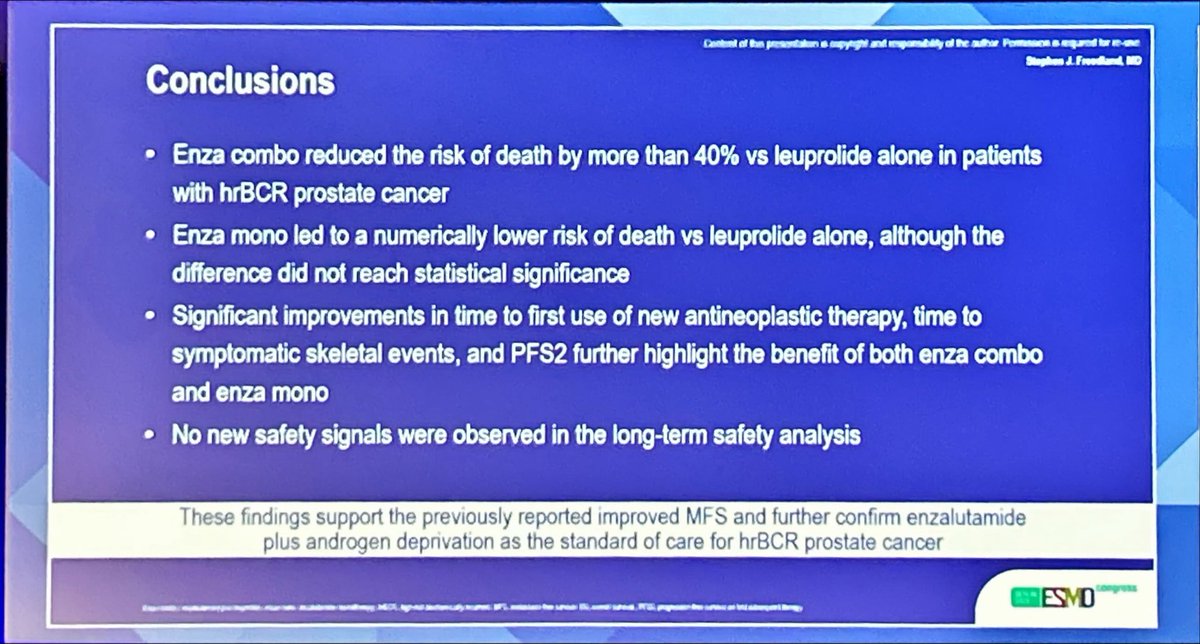
🚨improved OS with ADT+enza in high risk BCR (biochemical recurrent) #prostatecancer
New standard of care but important to reconcile the data with the results of PRESTO AFT19 (apalutamide) & integration in current landscape (PSMA, MDT).
#ESMO25
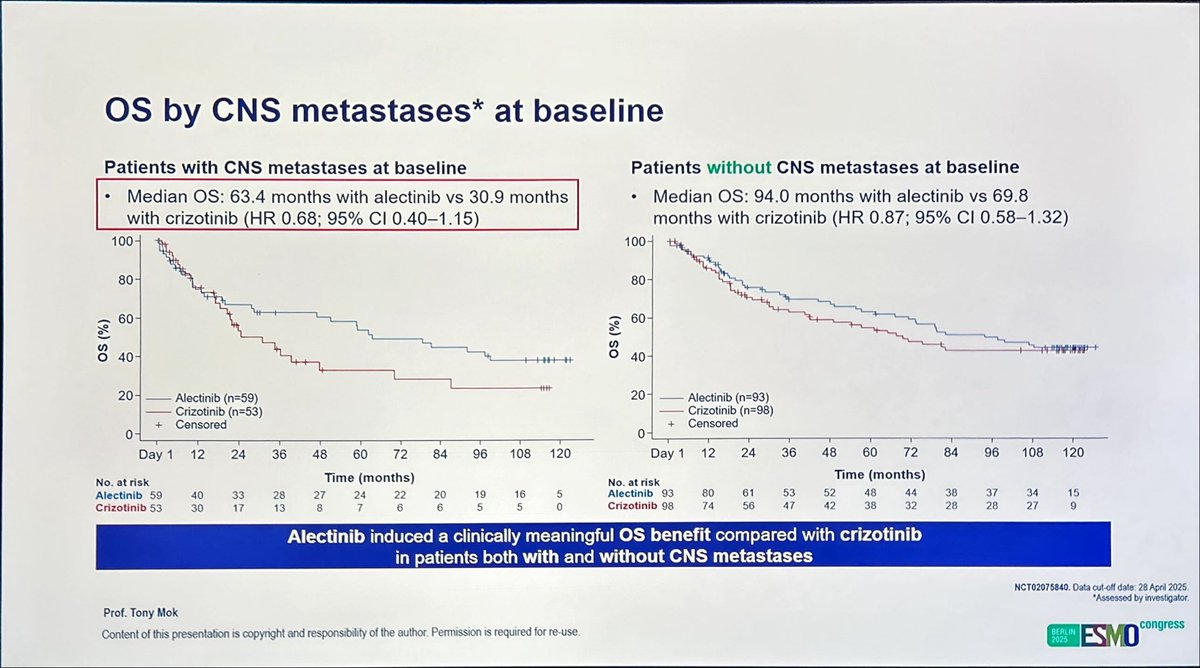
🫁 ALEX: final OS. @TonyMok9
Survival benefit with first-line alectinib vs crizotinib in advanced ALK+ NSCLC (mOS 81.1 vs 54.2 mo).
Benefit observed regardless of CNS metastases status; safety consistent with prior data.
#ESMO25#CánCare#NSCLC#ALK#lcsm
🆙#ESMO25🇩🇪
🔥#LCSM Proffered paper, non-mets, SCLC
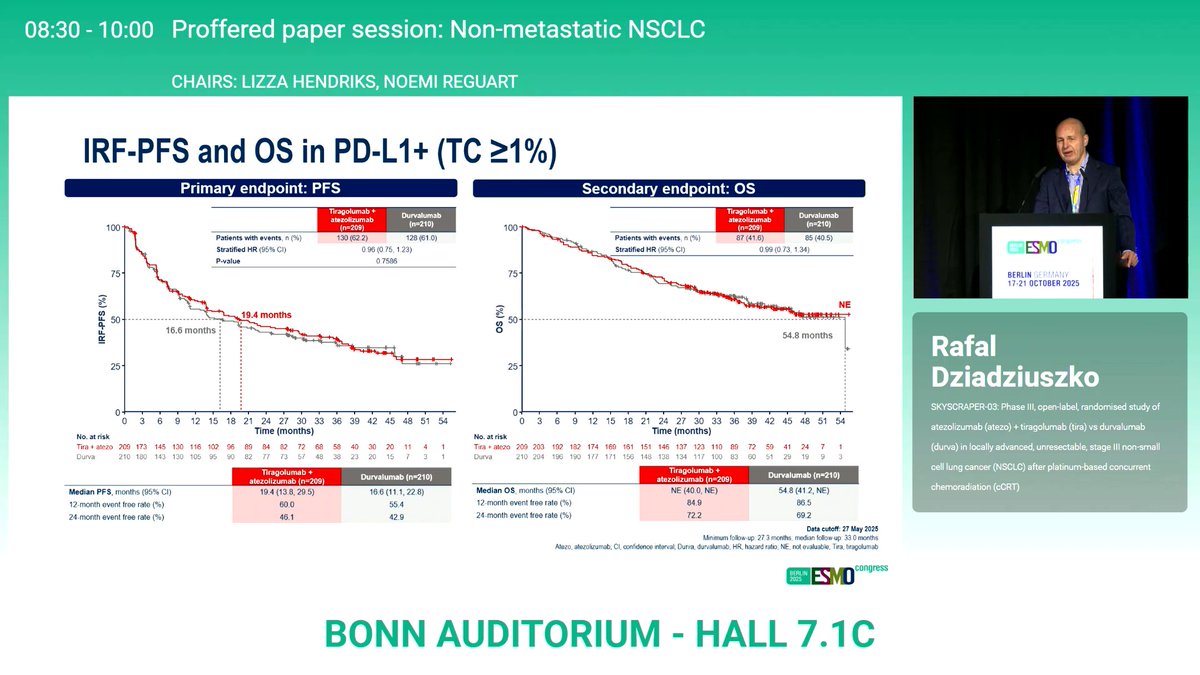
☑️SKYSCRAPER-03: Phase III, open-label, randomised study of atezolizumab + tiragolumab vs durvalumab in stage III NSCLC after platinum-based cCRT
☑️OS 19.4m vs. 16.6m, HR 0.96 (95%CI 0.75-1.23)
🎙️Dr. Rafal Dziadziuszko
@OncoAlert@myESMO@Larvol
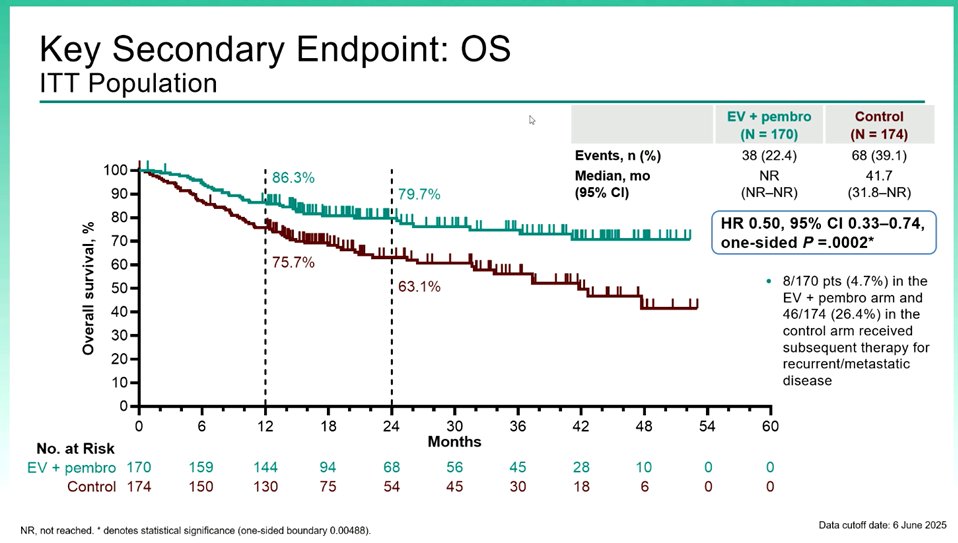
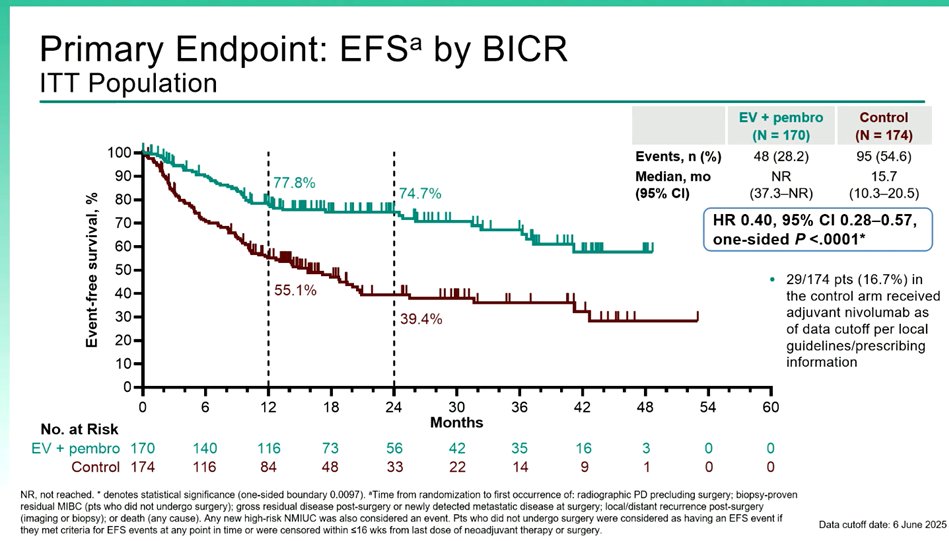
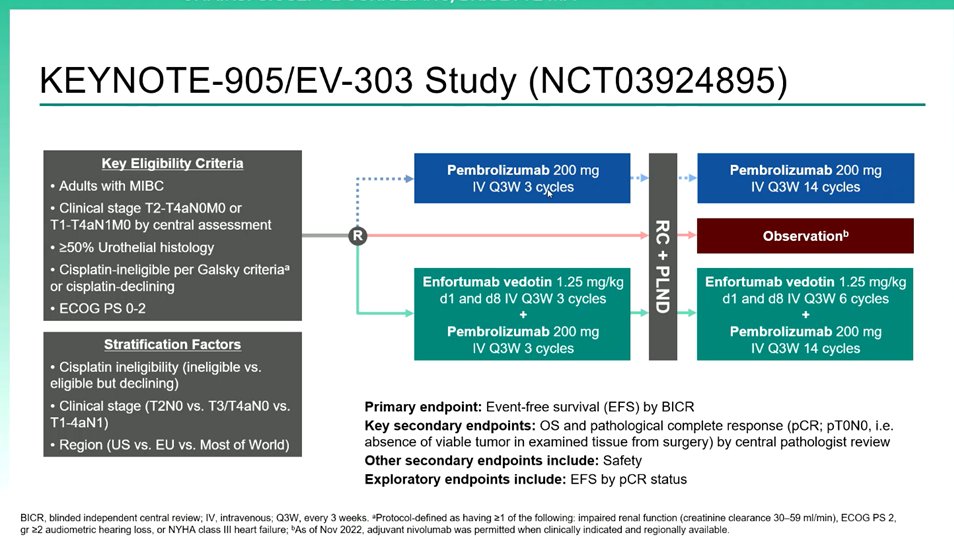
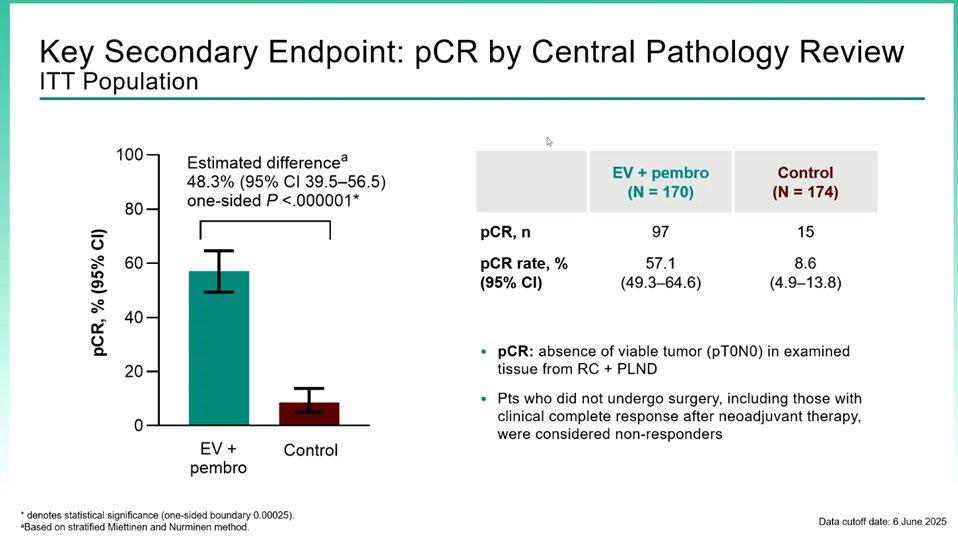
#ESMO25 KEYNOTE-905/EV-303
Perioperative pembro + Enfortumab vedotin vs surgery alone in cisplatin ineligible MIBC
The combo achieved major gains ↑EFS HR 0.40, ↑OS HR 0.50, ↑pCR 57% vs 9% (P<.001)
Practice changing & the new SoC in this setting 🌟
@OncoAlert@myESMO
#ESMO25
FLAURA2: Final OS analysis confirmed Osi + CTx ↑ OS vs Osi mono (HR 0.77; p=0.02) in 1L EGFRm NSCLC.
Benefit was consistent across poor-prognosis subgroups (CNS mets, L858R, plasma EGFRm+, TP53 altered), reinforcing combo as the 1L SoC
@OncoAlert@myESMO
ALEX trial 1st L alectinib (vs crizo) not ⬆️OS but trial not powered for OS. The best drug first? living w/o disease PD and good control of risk of brain PD count most!!Today lorlatinib is one SoC, futute SoC in 1st line Neladalkib (NVL655), ALKZAR trial vs alectinib?. #ESMO25
A real BRIDGE very clever study to fill the gap between resectable and borderline resectable #nsclc with early MDT reassessment and high resection rate and pCR. Excellent presentation as usual by Martin Reck
@OncoAlert @ONCOassist
🆙#ESMO25🇩🇪
🔥#LCSM Proffered paper, mets
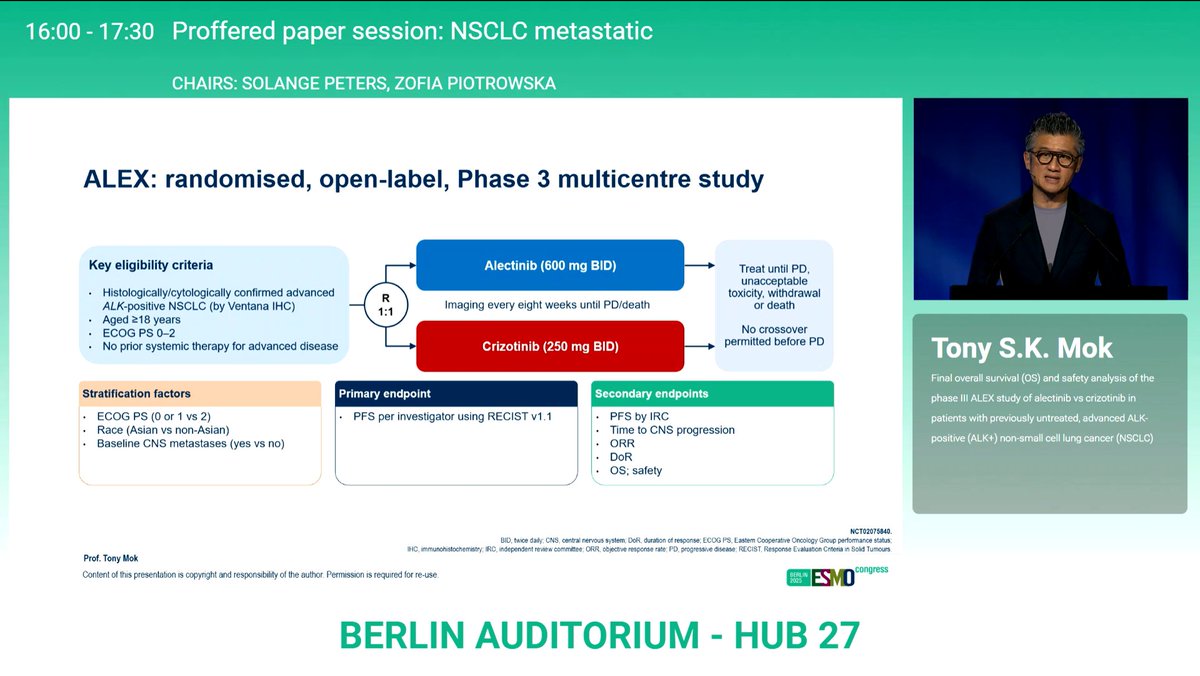
☑️ALEX: Final OS of ALEX study of alectinib vs crizotinib in ALK-positive NSCLC
☑️Alectinib/Crizotinib mOS 81.1m/54.2m
🎙️ @TonyMok9@OncoAlert@myESMO@Larvol
🔥BREAKING‼️ @NEJM 🆙
✅Survival with Osimertinib plus Chemo in EGFR-Mutated Advanced NSCLC
🎯mOS 47.5m vs. 37.6m, HR 0.77 (95%CI, 0.61 to 0.96)
🎙️ Dr. Pasi A. Jänne
#WCLC25#ESMO25#LCMS@IASLC@myESMO@OncoAlert@Larvol
https://t.co/Lp3AiRvwiS
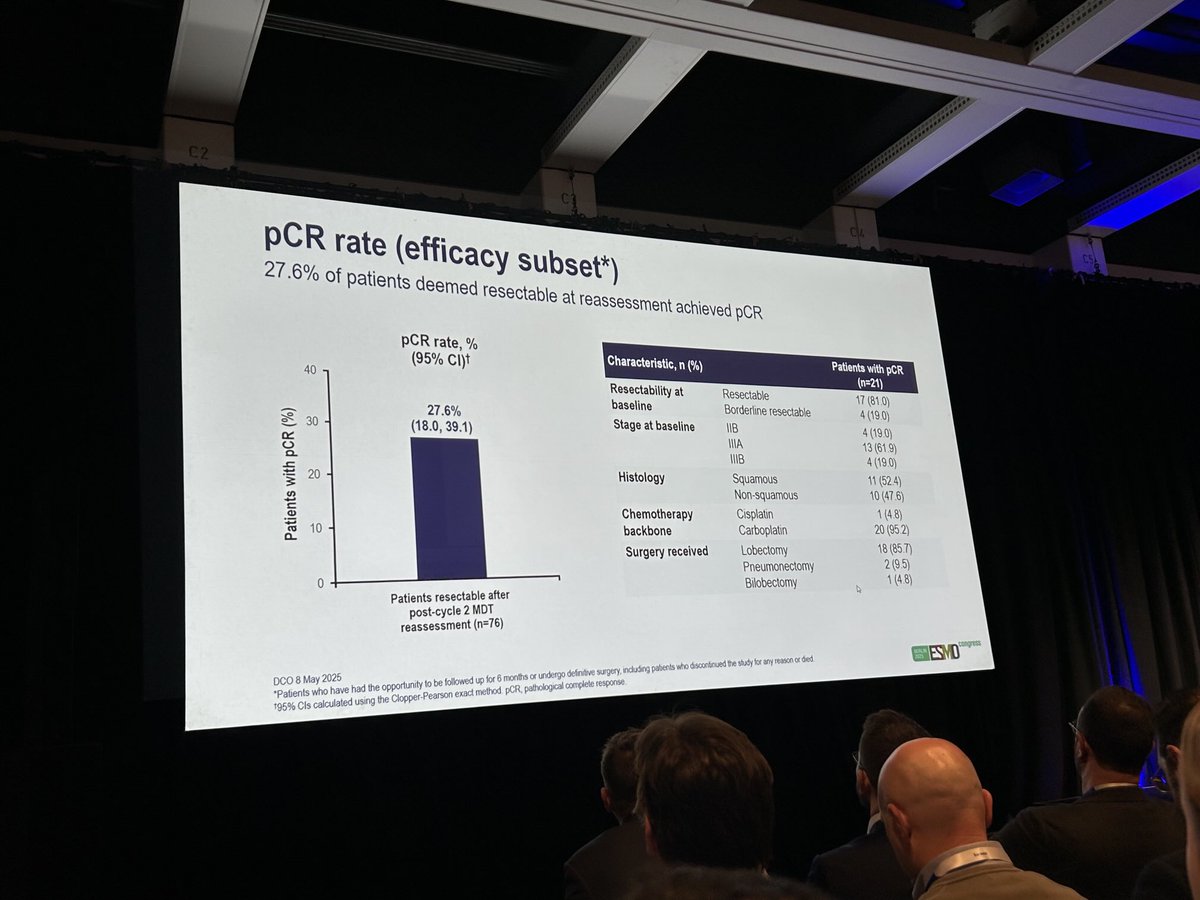
🫁 MDT-BRIDGE @MartinReck2@myESMO
In stage IIB–select IIIB NSCLC, close MDT reassessment during neoadjuvant durvalumab + chemo enabled local treatment in 95% of pts.
Resection rate 85.7% (94% R0), pCR 27.6%.
Outcomes consistent with AEGEAN, even including borderline resectable cases.
#CánCare #NSCLC #lcsm #ESMO25
Practice changing results from PROTECT trial. Patients with cribriform positive disease do better with radiotherapy & hormones rather than surgery or active surveillance #radonc#pcsm https://t.co/PvDPHU5tuL
KN905
Very impressive results with neoadjuvant EV-P in cisplatin-ineligible muscle invasive #bladdercancer presented by C Vulsteke at #ESMO25
✅Improved PFS & OS
✅High path CR rates (57%)
✅No delay in surgery
✅Expected toxicity in this frail population
New SOC
Key question is whether this would allow bladder preservation protocols and not cystectomy.
What is the point of removing 57% of intact bladders? Could we do less to improve patients QoL?
#radonc
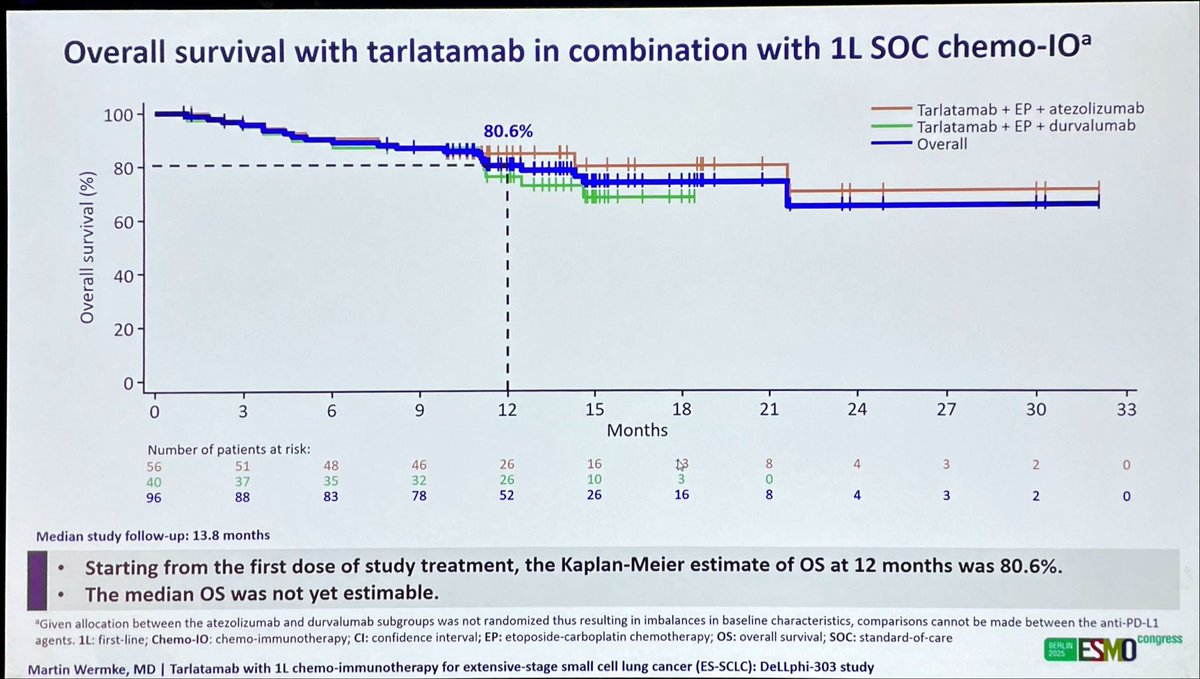
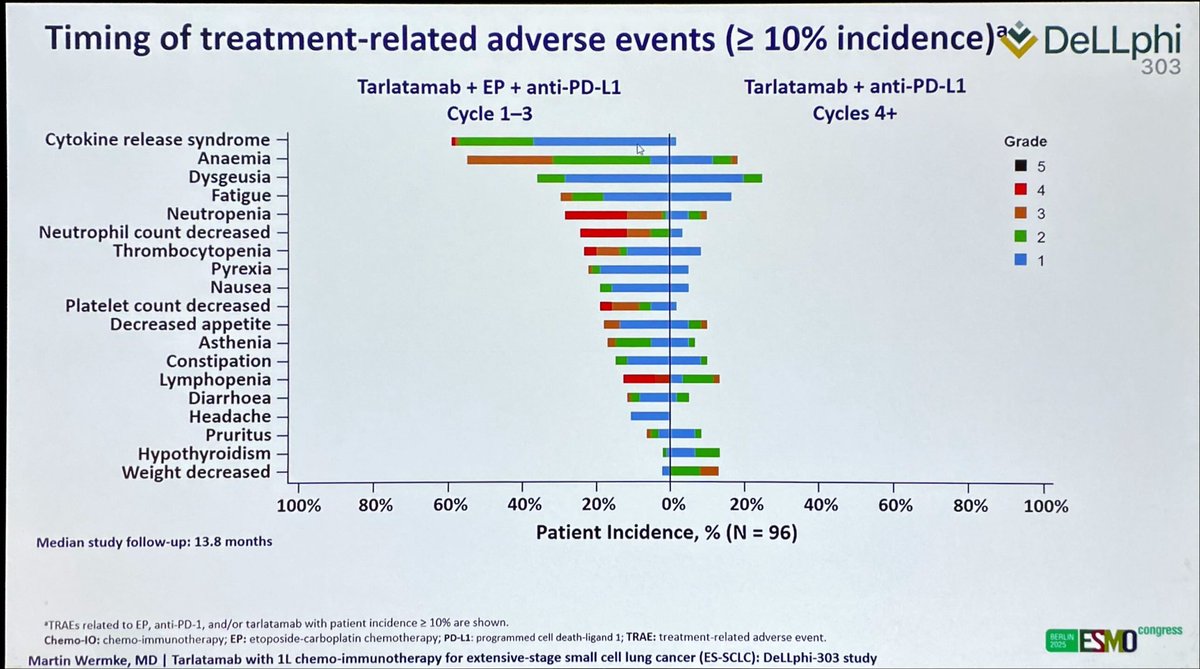
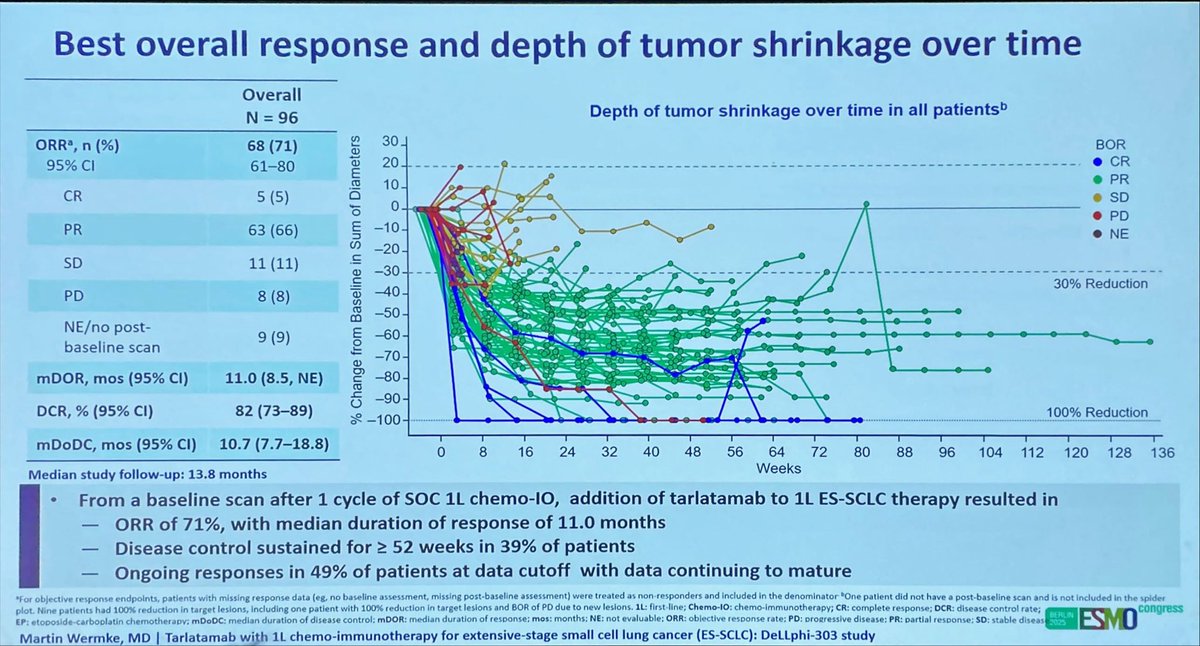
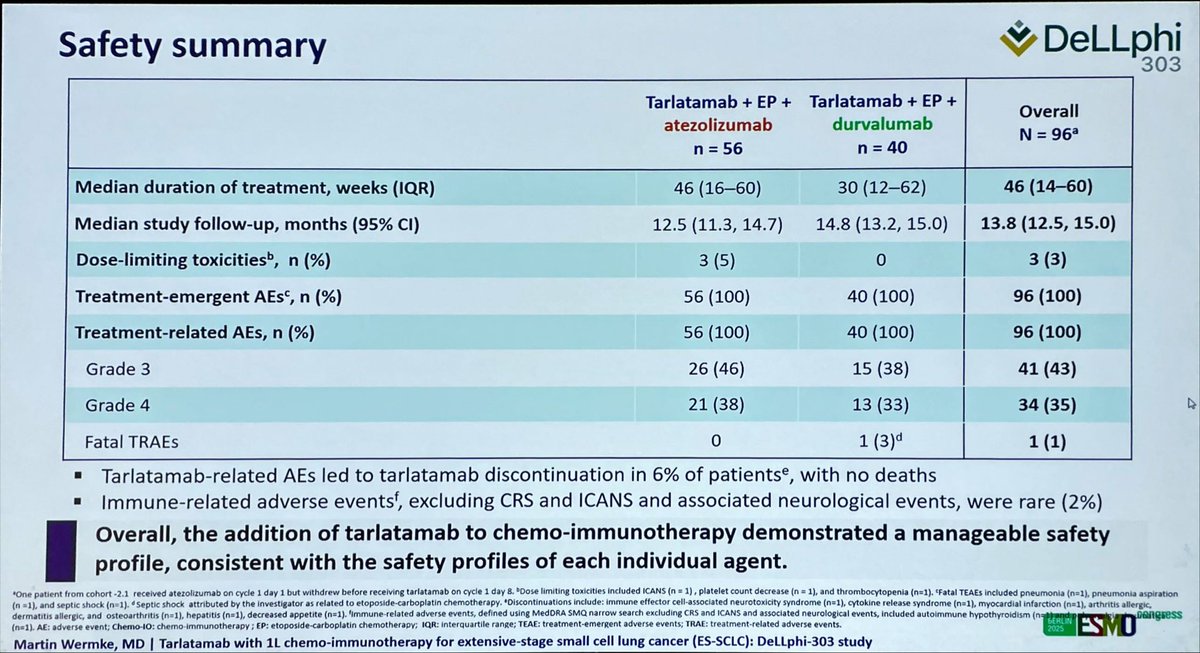
Tarlatamab incorporated upfront with chemo-immunotherapy breaks all the known stats in first-line SCLC. No new data safety concerns. Awaiting data from randomized ph3 trial, but likely to be the next SoC. #ESMO25#SCLC@SclcSMASHERS
Median overall survival for newly diagnosed metastasic ALK+ lung cancer patient treated with alectinib is …. 🥁
81 months
#ESMO25#LCSM@TonyMok9 ALEX trial
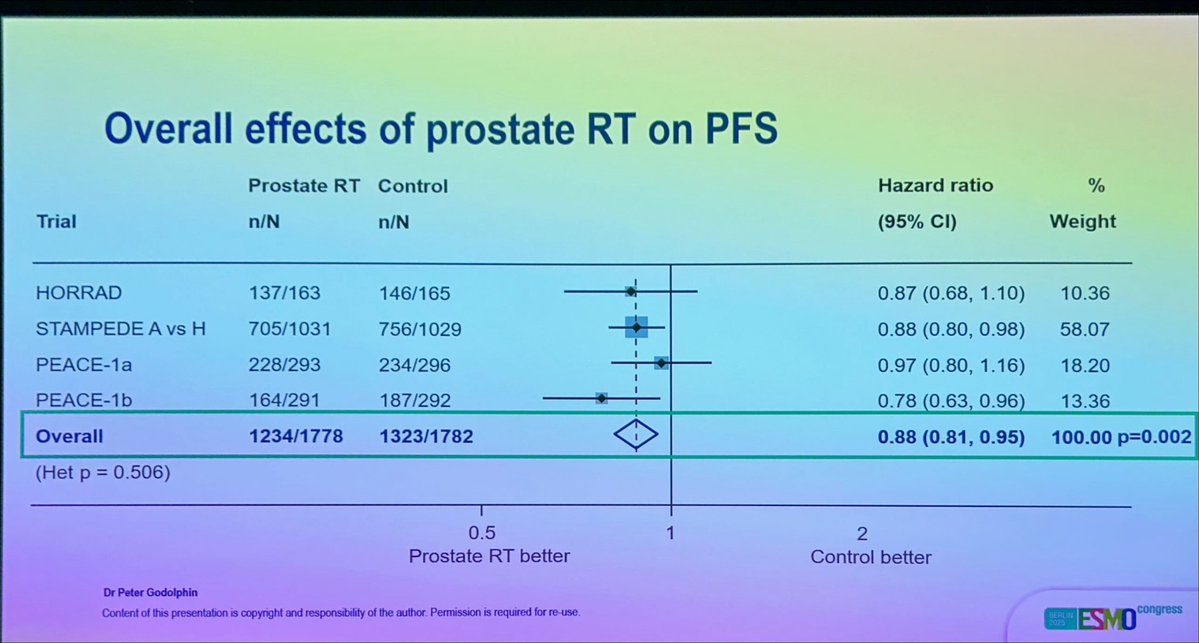
STOPCAP at #ESMO26
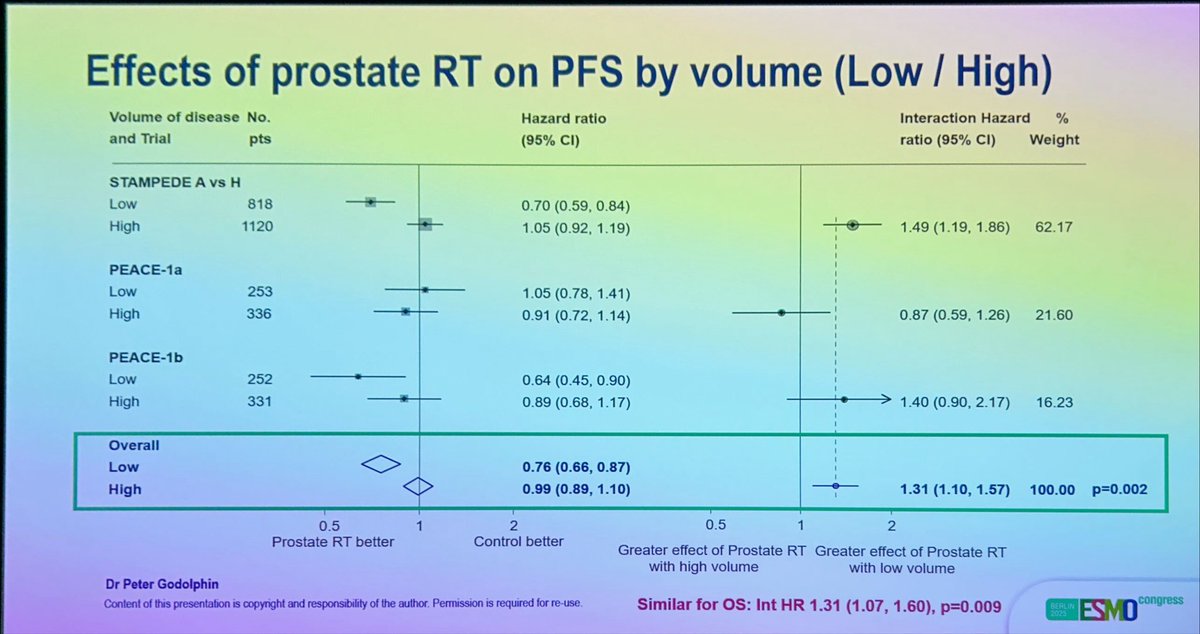
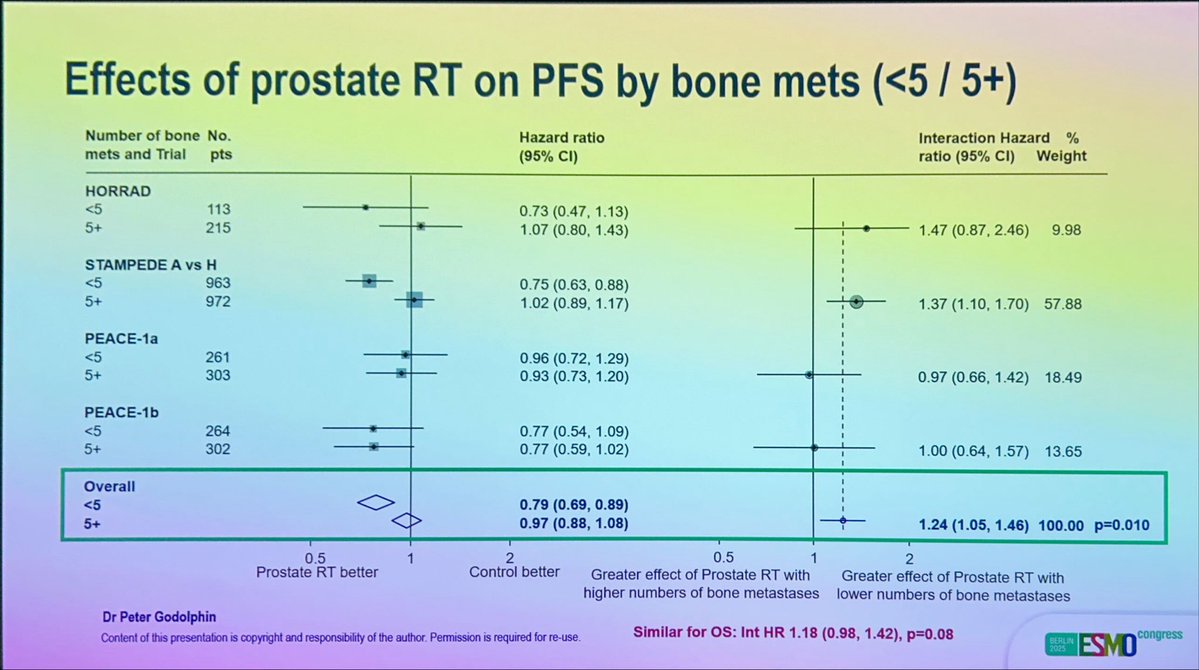
Benefit of #radiotherapy in de novo M1 #prostatecancer on OS & PFS.
Restricted to <5 bone or low volume mets on conventional imaging.
No interaction with other patient/tumor characteristics.