Something significant is about to happen for clinicians 🧬
We're partnering with @ALISHealth_AI, the clinical co-pilot for longevity, to build the full technology infrastructure behind their platform. And we're doing it with an AI architecture that has never been deployed in clinical medicine before.
ALIS is founded by two people whose names need no introduction in this field: Martin O'Dea (Longevity Summit Dublin) and Prof. Brian Kennedy (NUS Medicine). Their science, including the LinAge clock (with Jan Gruber), the Intervention Atlas, and the PC-based methodology, is at the forefront of biological age research.
Rejuve Biotech provides a reasoning engine architecturally different from LLMs. Data ingestion, intelligence engine, clinician dashboard, reporting, and the infrastructure to scale it to 10,000+ clinics and 1 million+ patients.
The core of what we're bringing is Hyperon, a neural-symbolic framework built towards AGI. Every clinical AI platform in this space today uses black-box models. They give clinicians a score. Hyperon gives them a reasoning chain. Every recommendation in ALIS is traceable to specific biomarkers, weighted by evidence quality, and auditable by the clinician who acts on it.
And it’s happening right now.
If you're running a longevity clinic and want to be among the first, the waitlist is now open: https://t.co/wR8k73uEET
2/2 Europe does have an event that is focused on aging science and brings the community together. We will try our very best to help this happen at LSD 2026.a
1/2 Very sad news about ARDD 2026. For many of us the end of August is one of the highlights of our year. There really is an awful lot of work behind these events and we hope Morten and team come back in 2027 and enjoy success in Boston in '26
For 2026 it is essential though that
@MaxUnfried No rejuvenation therapies now or in the foreseeable are given to people over 70. So if this is the metric of success we use we are in trouble for at least another half century.
SAVE THE DATE! LSD2025 will be at Trinity College Dublin *2-4 July 2025*
Join us for an exciting event and register to the waitlist for early bird details and discounts:
https://t.co/gQ9wCQGxMO
We can’t wait to see you there!
#longevitysummitdublin2025#dublinevents
William Greene at #LSD2024@hevolution_f aims to revolutionize healthspan science
• Funding cutting-edge research
• Supporting biogerontology investigators
• Translating discoveries into therapeutics
• Launching VC for longevity biotech
Full talk here: https://t.co/B7hrk1CDiQ
Fragmented data, privacy breaches, inefficiencies—healthcare faces numerous challenges. Blockchain is revolutionizing healthcare and longevity research by transforming data management, enhancing clinical trial platforms, and empowering patients with data ownership, transparency, and incentives.
@fedichev I see logic @davidpblackmore response but think we need to walk and chew gum concurrently here. error is not trusting public with multiple goals. Prevent disease but also prevent decline. research on both. Prevent decline may help slow disease, but is a different biological goal
I spoke at the excellent #ARDD2024 last week and broke the habit of a lifetime by presenting data :-) (On RMR1, natch.) Those who missed the livestream will have to wait for the video, but here's a photo (by Eugen Chirita), one of 100s at the site:
https://t.co/Rh1UODxp2w
Another great update and comments from @aubreydegrey
Definitely worth reading and supporting. RMR is an important milestone and threshold for future interventions and public awareness.
When RMR is achieved, everyone will start talking about rejuvenation and demand action.
✅ I signed, have you❓
Initiative led by @aubreydegrey and @BKennedy_aging
Now widely embraced with broad signatory endorsement across stakeholders in the longevity community.
Share & re-tweet! ♻️ 👨🏻⚕️
Dublin Longevity Declaration calls on governments, funding agencies, and the public to support innovative interventions for combating age-related diseases and extending healthy lifespans.
Spearheaded by @BKennedy_aging@aubreydegrey@MartinODea10
https://t.co/xDOMaMEA6p
Many apologies for having skipped a monthly update - I was just too swamped with preparations for @LongevityDublin (which was a roaring success as always - if you didn't attend, you missed a real feast of education and entertainment). Back on track now though!
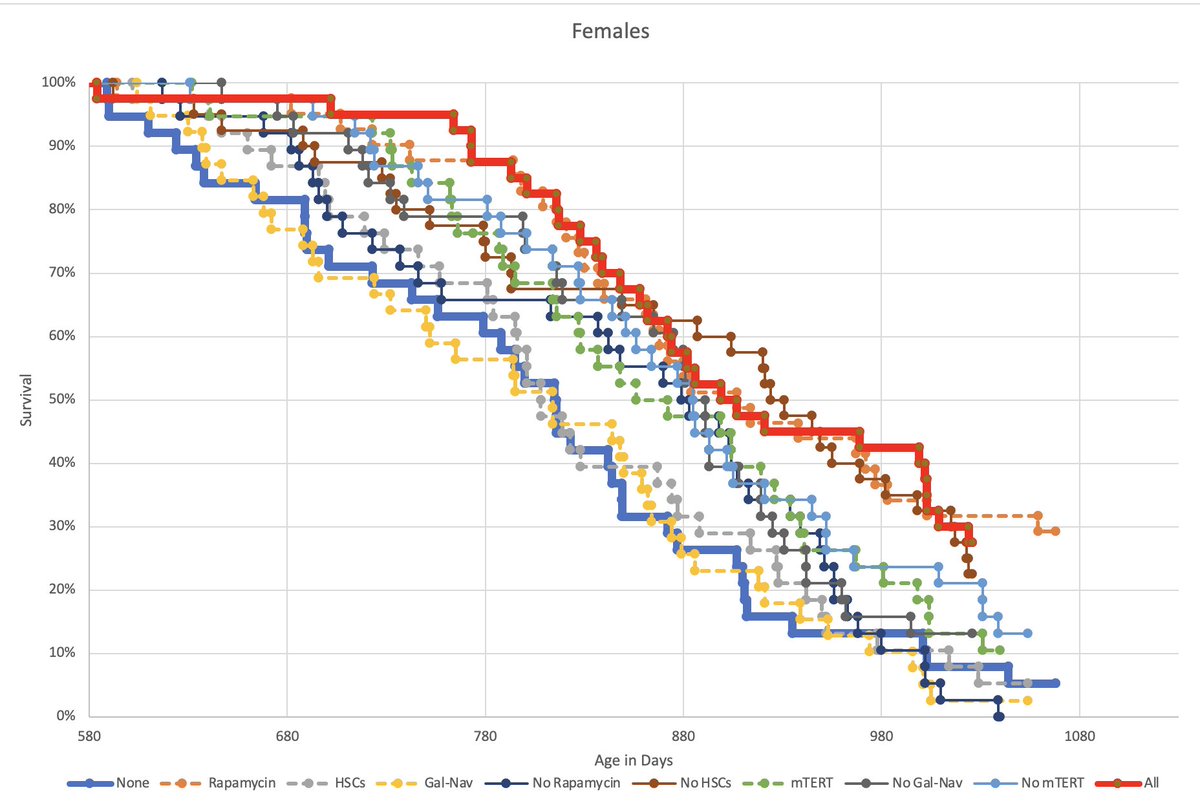
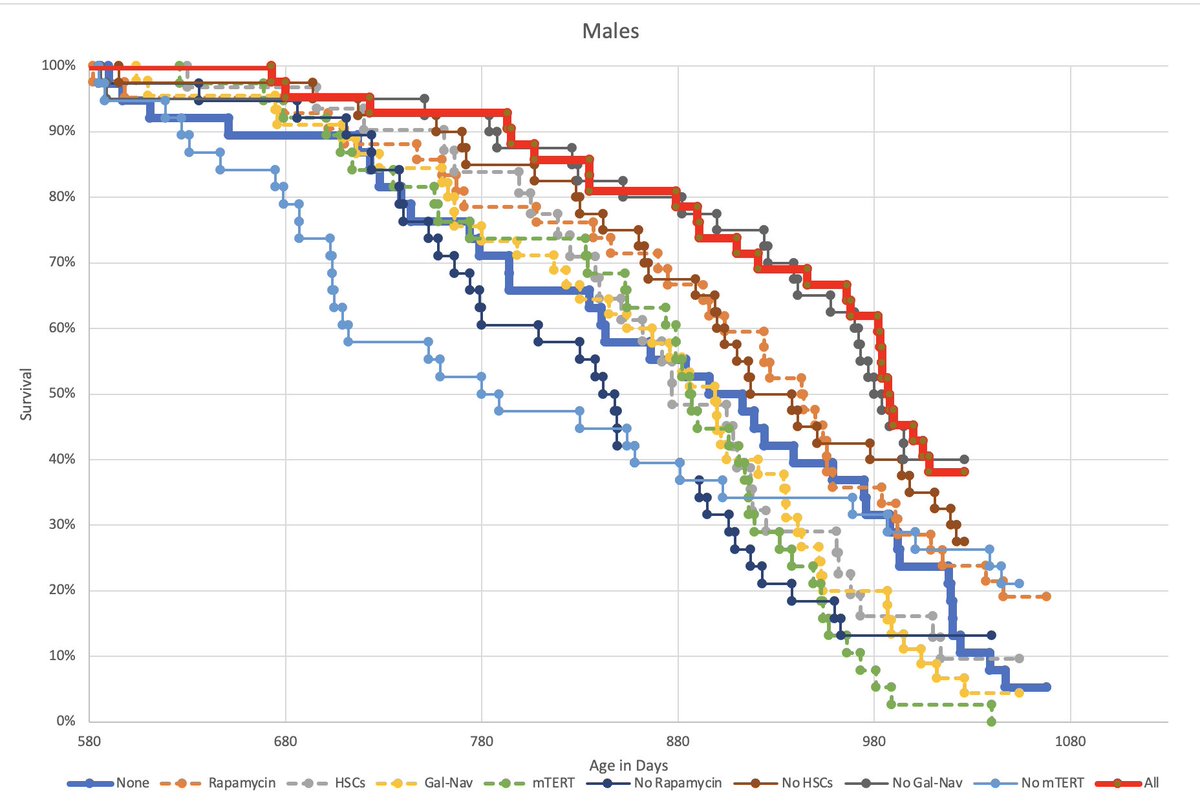
This update marks a milestone, namely that one treatment group of each sex has now entirely expired. For males it's the group getting only telomerase, and for females it's the group getting everything except rapamycin. In females, moreover, the group getting only rapamycin is doing as well as the group getting everything - both of them are still above 25% survival. I think it's now fair to conclude that the impact of rapamycin in the female groups has overshadowed everything else - which is disappointingly boring, but which we will of course be analysing in much greater depth as we collate more of the firehose of data on mouse health that we've been collecting.
In males, however, the situation is altogether more interesting, and since males of this strain are well known to live longer in the first place (and considerably more lifespan studies have been done on males than on females anyway), that's for sure the sex I would choose to give interesting results. Here, the rapa-only groups is also doing better than any of the other single-treatment groups, but it's being beaten not only by the all-four group but also by three of the three-treatment groups. Indeed, the all-but-rapa group, which was doing the worst of all a few months ago, has now overtaken all the other groups that aren't getting rapa. So at this point it can reasonably, albeit still tentatively, be said that the three bona fide damage-repair interventions are indeed conferring meaningful benefit over and above rapa in males, even if not in females. Nonetheless, the results for both sexes strongly argue for the decision we've provisionally made regarding RMR2, which is to give everyone rapa so as to provide the best possible baseline.
We've also, finally, reached the point where all groups have passed the 50% mortality point and we can thus do final analysis on median lifespans. But honestly I'm not sure there's much point, because everyone is (rightly) much more interested in maximum lifespans, which we're getting close to being able to analyse too. It's certainly weird that the no-telomerase group and the no rapa group fell below 50% in males at so early an age, but since they both completely caught up I have difficulty getting intrigued. And all other groups are maintaining pretty much the same rank order that they had at 50% survival (and indeed at 75% survival), so we may as well wait until the curves are complete (or almost so,anyway) before analysing them further.
@BarackObama Big ol place America with a colourful political adolescence still breathing, and so difficult to pinpoint single moments. Could spend hours on why but your orchestrating Biden over Bernie (from an Irish no dog (but humanity) in fight perspective)) could be last and sturdiest nail