Cognitive Biases in Multimodal Diagnostic Interpretation:
I find this fascinating, and I'll confess that I had an LLM help me with this. I hadn't thought of biases in pathology before, but I think this should be required reading for all pathologists. I'll confess that I've been sucked into each one of these biases over time. I particularly wanted to highlight incorporation bias, where you try to use somebody else's results, such as those from radiology or molecular testing, to interpret our own cytology or histopathology results.
👉Anchoring Bias
Definition: Overreliance on the first piece of information encountered.
Example: A pathologist may be influenced by a radiology report labeling a lesion as "suspicious," leading to an overly aggressive interpretation of borderline cellular atypia.
👉Confirmation Bias
Definition: The tendency to interpret findings in a way that confirms preexisting assumptions.
Example: A pathologist may favor a malignant interpretation in the presence of a clinical diagnosis suggesting carcinoma, even when features are equivocal.
👉Diagnostic Overshadowing
Definition: A dominant clinical context obscures alternative explanations.
Example: A known malignancy may bias interpretation of new findings, with benign lesions misclassified as metastases.
👉Incorporation Bias
Definition: Integrating the results of one diagnostic modality into the interpretation of another, compromising independent assessment.
Example: Pathologic interpretation is skewed by prior knowledge of a positive KRAS mutation, resulting in upstaging of an indeterminate smear.
👉Framing Effect
Definition: Diagnostic interpretation shifts based on how the case is presented.
Example: Labeling a specimen as “rule out malignancy” may prime the interpreter toward a malignant diagnosis.
👉Premature Closure
Definition: Halting diagnostic deliberation after an early conclusion is reached.
Example: A diagnosis of low-grade IPMN may lead to under-recognition of subsequent evidence suggesting high-grade atypia.
👉Availability Bias
Definition: Overestimation of a diagnosis based on recent or memorable cases.
Example: Recently, encountering a rare pancreatic neuroendocrine tumor may lead to overdiagnosis in future ambiguous cases. @smlungpathguy
Pitfalls of p63: Case 3
This is a spiculated mass detected on imaging. Again, p63 was performed, likely because of the fibrous background and the cribriform features, and it showed positivity.
What is your diagnosis?
@washu_pathology@washupathedu#breastpath#PathTwitter #PathX
Excited to share the news about the upcoming book ! “Authoritarian practices and humanitarian negotiations”. Grateful for the opportunity to contribute a chapter and design the cover.Dive into this insightful read—I invite you all to explore the diverse perspectives #humanitarian
Hot off the press!
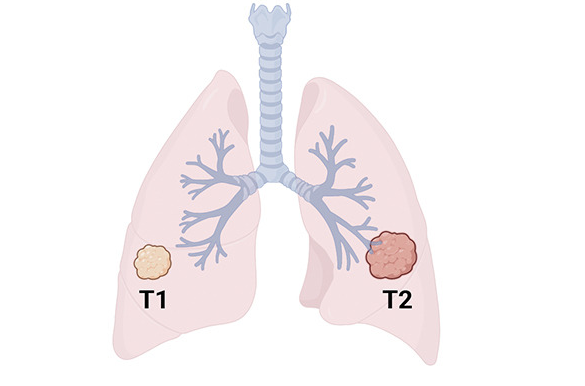
Delighted to share the review article by Jason Chang and I @ModernPathology on the ever-vexing problem of multiple lung carcinomas.
This affects ~1 in 5 patients with lung cancer, so is exceedingly common.
Recent molecular methods are providing major insights into pathology and clinical aspects here.
Please check it out!
https://t.co/ooysVyHWKQ
@PulmPathSoc@MSKPathology #PulmPath #MolPath @DrNetto@smlungpathguy
PGY-1 pitfall #1. Thyroid does NOT have a capsule. I had this realization after submitting multiple thyroids entirely, and my attending pointed out the capsule needed to be submitted only for certain cancers. The thyroid is not encapsulated
#humbled#rookiemistake#pathTwitter
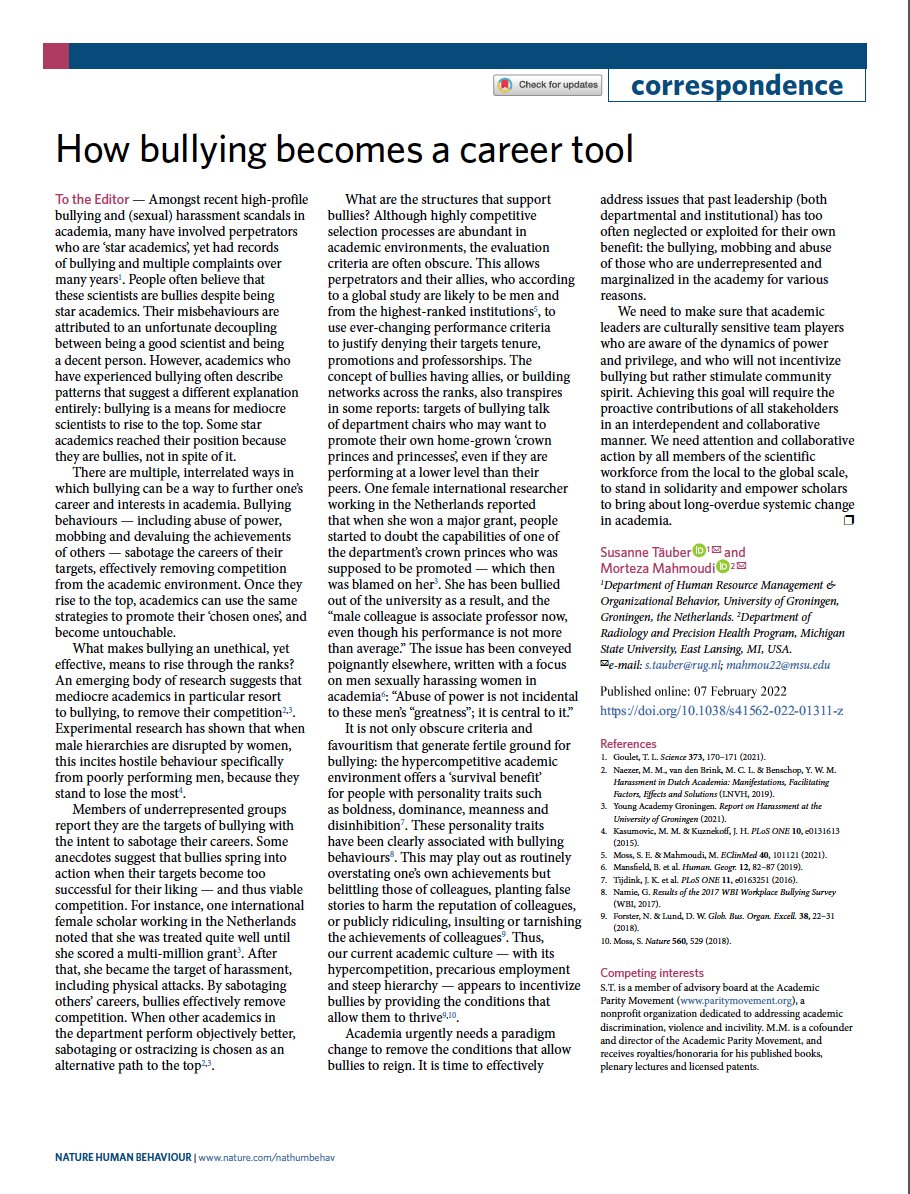
"Bullying is a means for mediocre scientists to rise to the top. Some star academics reached their position because they are bullies, not in spite of it." - Excellent piece about bullying in academia (and really any other professional environment). https://t.co/JTqGBaAuuf
Case of the month : A 72Y/O woman underwent an endobronchial #USG#FNA of a 1.0 cm well-circumscribed mass. What is the best diagnosis? submitted by: @MaelleSaliba@MichelleGarlin@NiyatiDesai13 and Dr.Saqi! #papcyto click 👉 for ans: https://t.co/RwigfGTkGu