I recently wrote about the effort to end the torture of pigs. On Thursday, @Dwarkesh_sp, @AvitalBalwit, and @NanRansohoff are hosting an in-person party for folks in the Bay Area to support the effort!
If you'd like to attend, sign up here! https://t.co/ccjHAbHoD6
This has quietly been a miracle month in medicine.
In the last 5 weeks we’ve got news on:
- retatrutide, the triple agonist GLP-1 from Lilly, basically melting fat and body-wide inflammation at record levels
- RevMed’s new pancreatic cancer drug showing unprecedented abilities to extend life
- small trial of a one-and-done PCSK9 gene editing therapy for slashing LDL cholesterol
- Mayo’s AI-assisted radiology showing vastly improved cancer detection
- this new therapy for metastatic solid tumors
This stuff is at varying levels of evidence. Retatrutide is ~100% on its way, other stuff needs more clinical trial data. But put it together and we’re maybe on the verge of majorly reducing the mortality of heart disease and cancer, the two leading causes of death in America.
A trolley is about to hit 5 people laying on the track
You can redirect the car, but the other track has not yet reached regulatory approval or completed its 1 year environmental testing period, so operating a train car on it is a violation of transit regulations
What do you do?
Today, the state of Washington randomly revoked the medical license of a clinician because they lost her fingerprints:
"Because your fingerprint submission was rejected, all eligibility requirements have not been met... and you are prohibited from practicing"
Now dozens of patients will have to miss appointments because of the state's incompetence will this is rectified. The company I work with will have to explain the revenue blip and its patients will be upset.
State medical licensure requires repeated, wasteful data aggregation and opens the door to hiccups like this one. Nobody is winning in the system we have created.
It's time to think about a new law to reform and put standards around state licensure and / or a national licensure clearinghouse. Enough is enough.
An incredible visualization of an alternative future for SF
A lot of ink is spilled on the topic of housing in SF ... this is one of the best treatments I've seen.
Every so often I think about how, in 2022, for $24B we could had "prototype vaccines ready for each of the 26 known viral families that cause human disease" so they can be deployed in 100 days if there was ever a need.
This effort was not funded. https://t.co/TJBuqp69Nn
Missing from the “will AI replace doctors?” debate is that doctors (and lawyers and psychologists and bankers) all vote & form the donor base to political parties & have deep community ties. The government will largely determine what AI is allowed to do, no matter what it can do
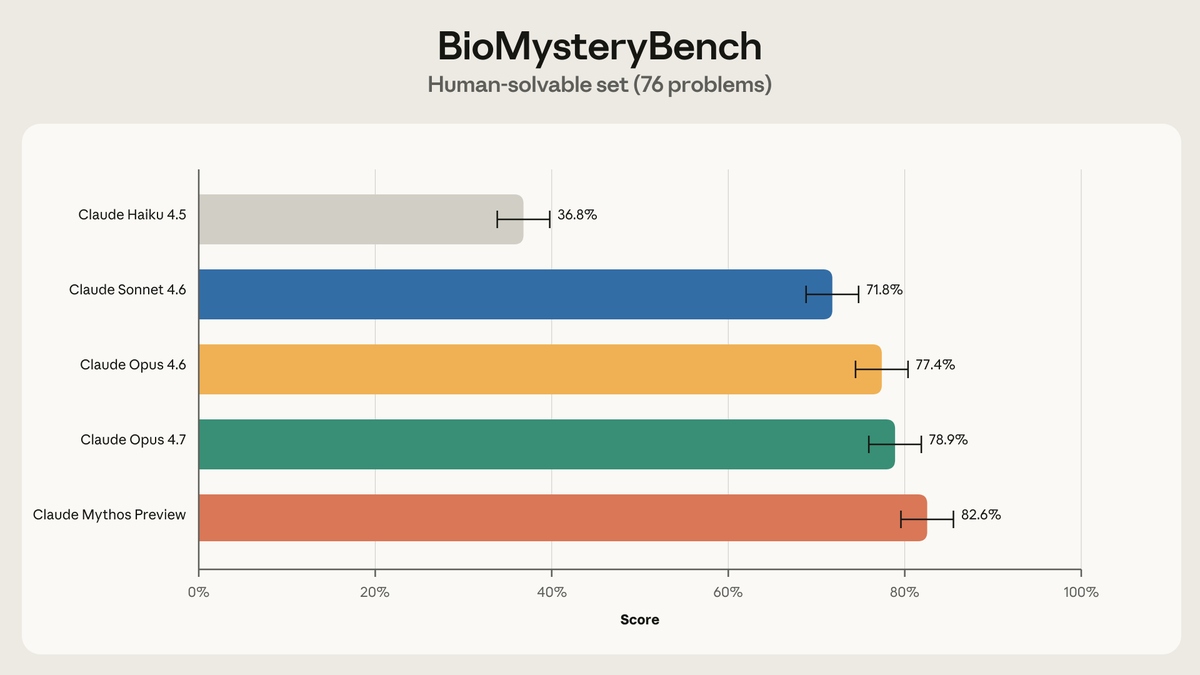
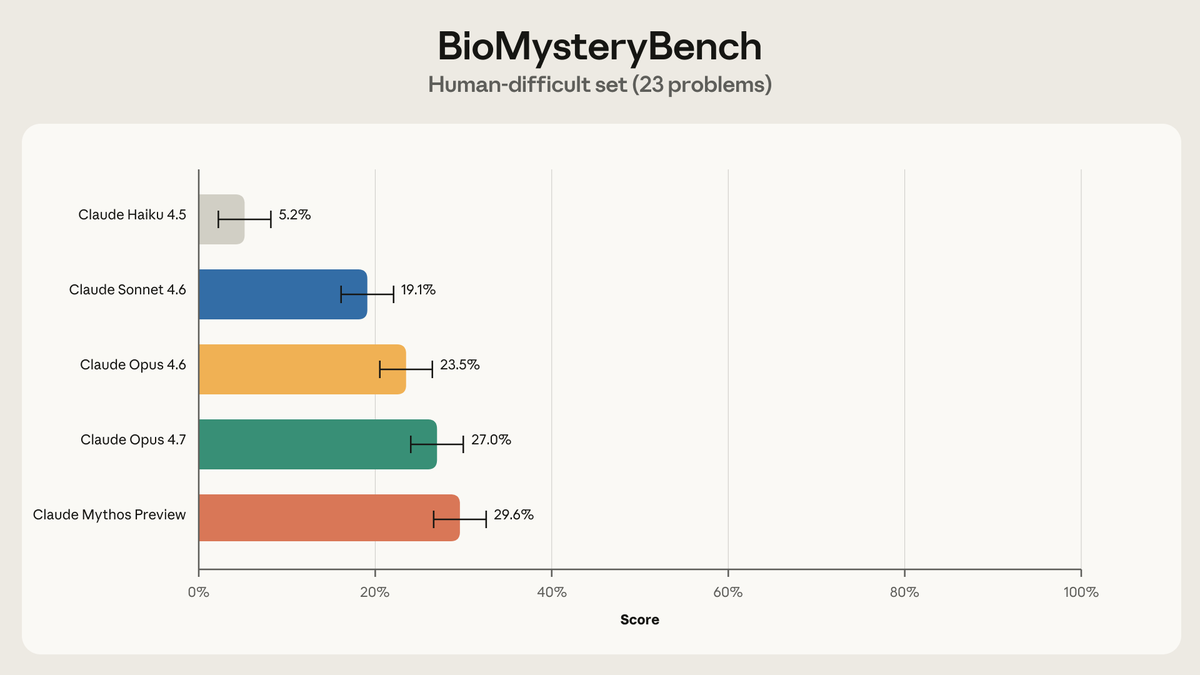
New on the Science Blog: We gave Claude 99 problems analyzing real biological data and compared its performance against an expert panel.
On 23 problems, the experts were stumped. Our most recent models solved roughly 30% of those—and most of the rest.
Last year I called for federal pre-emption of heterogeneous state laws regulating healthcare AI, and for the creation of a new entity within HHS to evaluate AI systems.
I am glad to see @Bob_Wachter and @ZekeEmanuel endorse and build on these ideas in JAMA.
According to Wachter and Emanuel, "at least 47 states are considering more than 250 clinical AI bills and some have enacted laws addressing data privacy, transparency, bias, and payment policies."
Fragmentation and poorly designed state laws like Mia Bonta's AB 1979 in California, which would ban clinical AI, do not serve patients and physicians. Federal pre-emption - aligned with President Trump's July 2025 AI Action Plan - should be a a bipartisan priority.
This site can be very negative so let me say today that @KelseyTuoc is awesome. Rational , reasonable, and wise while also being benevolent and gracious. An excellent writer. Bravo.
The consumer health stack is commoditizing
Getting labs, pulling in your medical records, booking a telehealth visit, even AI primary care. All of these are relatively swappable and VC cash incinerators by themselves. When every layer of the stack is interchangeable, you start asking which piece actually has staying power.
I think it's wearables, and one core reason is body real estate.
You're not wearing two smartwatches. You're not rocking an Oura Ring AND a Samsung Galaxy Ring AND a RingConn like some kind of biohacking Xiaolin Showdown. You pick one. And once you've got 18 months of resting heart rate data and sleep baselines built up on that device, switching to a competitor means starting over from scratch.
Plus every other piece of the consumer health stack is reactive and requires you to initiate. You have to book the visit, order the labs, log into 15 different MyChart instances to pull up the records. Wearables can alert you proactively and say “something’s off”, as my Oura ring does every time the GERD dragon rises at night.
And ironically, I think the business model for wearables is about to become more valuable. Software companies are currently going through an existential crisis realizing that they might be getting commoditized as AI gets better at engineering and many of the moats they’ve been used to are evaporating.
Hardware has always been dunked on because they have worse margins, they’re hard to scale, and there haven't been network effects. But now this might be changing - wearable companies get margins from the hardware AND recurring software (Whoop's subscription model, Oura's membership, Apple's ecosystem lock-in).
It’s so dumb that physicians need to get a medical license in every state. They all have different processes and takes forever.
Why doesn’t a startup create a national medical license? Physicians just pay an annual fee and can practice anywhere.
Is anyone building this?
IMO most of US healthcare would be fixed* if we did a few simple things
1) divorce employers from providing health insurance
2) Use a price setting mechanism that was transparent (government setting prices or price transparency)
3) Everyone in one risk pool (e.g. on the exchanges, single payer, etc)
*fixed in the sense that you would be making tradeoffs between cost, quality, and access to care - but at least those tradeoffs would clearer
One of the things I found really frustrating about public health guidance during the pandemic was that the public wasn't trusted with nuance, so the communication was often over-torqued.
I think health communicators should trust their audiences with nuance.
"Friends, stop drinking alcohol. Not cut back. Eliminate." isnt' really nuance. It's absolutism. You're offering a pragmatic defense of absolutism, and it's smart to be pragmatic, but I'd prefer we just be honest: Alcohol is a delicious bit of extremely mild cellular poison and having too much of it is really bad in the long run but having a little of it won't kill you.
Everything in the realm of diet circles the issue of moderation. Chronic caloric surplus leads to obesity. Severe caloric deficit can lead to death. I'd prefer we attempt to articulate the principle of moderation in alcohol, too