Retweets are not endorsements. Once a RCEM President, now just an EP trying my best. Likes data, vaccines and people. Dislikes 🧌 Won't engage with anons, soz
@sib313@999Daedalus007@2manypeople4me It's the four S's of planning: staffing, space, systems and stuff. Fixing one without fixing the other doesn't work well.
@LittlePersonDoc@PreetKGillMP It’s an odd argument to choose, when there are so many other more meaningful potential benefits, e.g. reduced duplication of investigations, safer medication etc
@TJCoats@jo3hill A neat way to illustrate this is by plotting mean daily attendances against mean ED length of stay in minutes. (Thanks to @kurtstat ) It tells the story that no one ever listens to 🙄
The @CRAFFTStudy recruited 750 children.
329 (44%) had completely off-ended fractures - the kind many clinicians might feel must be reduced.
This wasn’t a cohort of children with minor injuries. 👇
@drkeithsiau My residents did a systematic review of case reports of harm. Spoiler. Tooth picks and fishbones are particularly bad (sharp and don’t show on CT) We found no harm from drawing pins and safety pins. Harm can definitely occur below the diaphragm
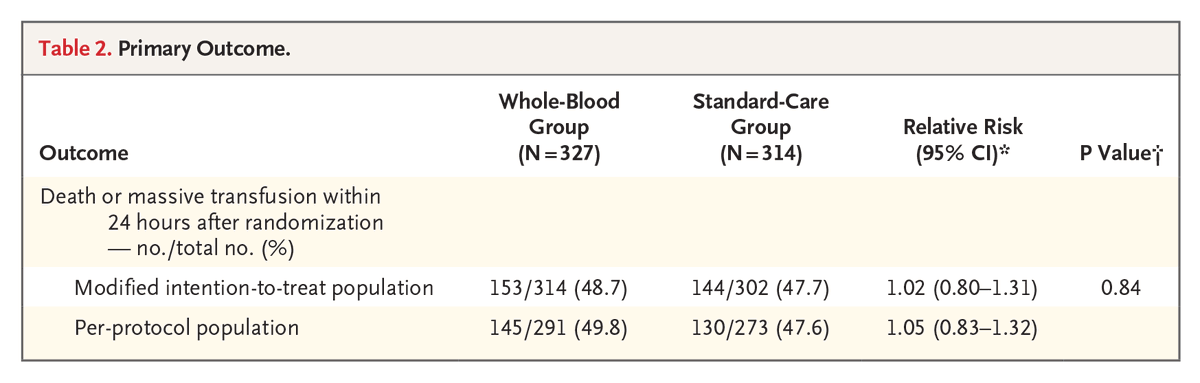
Presented at #ISICEM:
Among patients with traumatic hemorrhage, prehospital whole-blood transfusion was not superior to standard transfusion with red-cell and plasma components in reducing the risk of death or massive transfusion. Full phase 3 SWiFT trial results: https://t.co/67l1bSI81L
@ISICEM
The association between long emergency department stays and inpatient length of stay: a retrospective cohort study | BMC Emergency Medicine | Springer Nature Link. Published today by my residents. Another harm of long ED stays… 1/n https://t.co/2QFTpWQFpQ
7/n So what? We already know that long ED stays are associated with all sorts of harm for patients. This shows that there is a vicious cycle of a long ED stay and long IP stays. Long inpatient stays will worsen ED crowding