New data from 10,421 patients with metabolic syndrome: the C-reactive protein-triglyceride-glucose index (CTI) outperformed 23 cardiometabolic markers — including TyG, CRP, NLR, and non-HDL-C — as a predictor of CV mortality.
Patients in the highest CTI quartile had a 60% higher risk of CV death.
Integrating inflammation + metabolic stress into a single index may be the key to better risk stratification in MetS.
📄 Journal of Clinical Lipidology (2026)
#Cardiology #MetabolicSyndrome #CVDRisk #Inflammation #PreventiveCardiology
https://t.co/CAWw1R35q7
🚨 South Asians develop heart disease a full decade earlier than Europeans, with double the heart attack and stroke risk.
Standard risk calculators miss this entirely.
The tools your doctor uses to protect you are failing you.
I am a cardiologist who has spent years treating South Asian patients who had "normal" risk scores right before their first heart attack.
That number on the calculator meant nothing.
And the data explains exactly why.
💓 Here is what the science actually says.
A landmark UK Biobank study published in Circulation in 2021 analyzed South Asian cardiovascular outcomes against European populations.
The result was not subtle.
✅ UK Biobank Circulation Study: South Asians carried a hazard ratio of 2.03 for heart attack and stroke compared to Europeans.
That is double the risk.
Not slightly elevated. Double.
And the Pooled Cohort Equations, the standard calculator your doctor uses to decide whether you need treatment, completely failed to detect it.
The American Heart Association officially recognized South Asian ancestry as a cardiac risk-enhancing factor in 2018.
They placed it in the same weight class as high blood pressure and smoking.
That matters because most physicians are still not acting on it.
🔬 Why South Asians carry this outsized risk:
South Asians have higher rates of insulin resistance even at normal body weight
Visceral fat accumulates at lower BMI thresholds compared to Europeans
ApoB and small dense LDL particles run higher in this population
Lipoprotein(a) levels are elevated in a significant portion of South Asian individuals
Inflammation markers trend higher even in the absence of traditional risk factors
Standard BMI cutoffs were built on European data and miss metabolic danger in South Asian bodies
⚠️ The calculator problem is not minor.
The Pooled Cohort Equations assign a 10-year cardiovascular risk score.
That score determines whether you get treated.
It was built predominantly on European and African American cohort data.
South Asians who score below 7.5% on that calculator and get told they are fine are sometimes the exact patients who show up in my cath lab three years later.
This is not a failure of the patient.
This is a failure of the tool.
🩺 What actually needs to happen in a South Asian patient visit:
Calculate BMI using South Asian thresholds. Overweight starts at 23, not 25. Obese starts at 27.5, not 30.
Measure ApoB directly. LDL alone misses the particle burden.
Check Lipoprotein(a) at least once. It does not change with lifestyle and you need to know your baseline.
Order a coronary artery calcium score if the standard calculator shows borderline risk. It reclassifies South Asian patients correctly when the equations fail.
Treat South Asian ancestry itself as a risk enhancer in your clinical decision making.
"A South Asian patient who appears low-risk by standard calculators, receives a coronary artery calcium score showing early calcification, and starts a statin at 38 instead of waiting until 52 can prevent a heart attack that would have ended their career, their presence at their children's milestones, or their life. That is the difference between a calculator that missed the mark and a physician who looked further."
❌ Your ethnicity is not just a demographic checkbox.
❌ A normal risk score is not the same as low risk if you are South Asian.
❌ Waiting for symptoms before acting is how South Asians end up with severe disease in their 40s.
The question is no longer whether South Asians carry elevated risk.
The question is whether your cardiologist knows how to measure it.
❤️ Bottom line:
South Asian ancestry is not a background detail. It is a clinical finding that changes how risk should be assessed and treated.
The UK Biobank data covering hundreds of thousands of individuals confirmed a hazard ratio of 2.03. This is not a small signal in a small study.
Get your ApoB measured. Get your Lipoprotein(a) measured. Ask about a coronary artery calcium score. Know your South Asian-adjusted BMI.
South Asians who get correctly risk-stratified in their 30s and 40s and treated early do not become the patients I see in crisis at 50.
Are you South Asian and has your cardiologist ever mentioned any of this to you?
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #SouthAsianHealth #HeartAttackPrevention #ApoB #Lpa #PreventiveCardiology #MetabolicHealth
Bempedoic acid just got a new unexpected benefit — less blood clots?
Could bempedoic acid have a role beyond LDL lowering?
Possible mechanisms:
🔸 Anti-inflammatory effects (↓ hsCRP)
🔸 Lipid-inflammation-coagulation axis?
🔸 Off-target pleiotropic effects?
Excited to share our latest study published in Brachytherapy describing an approach to managing synchronous prostate and rectal cancers using pelvic chemoradiation and an HDR brachytherapy boost.
https://t.co/YoTj2LxYCk
#RadOnc#Brachytherapy#ProstateCancer#RectalCancer
Important and timely work exploring how inflammation + cardiometabolic dysfunction intersect in PAD. 🩸🦵
Excellent collaboration by @SahilGhay, @DrTcard ,@UjuetaFrancisco and team 👏
CTI may help uncover vascular risk that traditional markers alone can miss — especially in early/subclinical disease.
#CardioTwitter #PAD #Atherosclerosis #PreventiveCardiology
🚨 New publication in Atherosclerosis Plus 🫀
Can a simple inflammatory-metabolic index help identify PAD risk?
In our analysis of U.S. adults, the C-reactive protein–triglyceride-glucose index (CTI) was independently associated with lower-extremity peripheral artery disease.
Key findings 👇
🔹 Each 1-unit ↑ in CTI = 47% higher adjusted odds of PAD
🔹 Highest CTI quartile = >2-fold higher odds vs lowest quartile
🔹 CTI was linked to both clinical PAD and borderline ABI
🔹 CTI outperformed TyG and improved PAD discrimination beyond metabolic risk alone
These findings suggest CTI may offer complementary insight into vascular risk and early/subclinical PAD. 🚶♂️🩸
Grateful to our amazing team and collaborators!
https://t.co/H5lWAhu3cj
Amazing editorial highlighting how EPA-derived pro-resolving mediators may help explain EPA-EE’s cardioprotection beyond triglyceride lowering, with potential roles in inflammation resolution and plaque stabilization!
Sudden cardiac arrest (SCA) prevention is a paradox ➡️ we focus on a few people at highest risk (e.g., low EF), but most SCA occurs in people without known disease.
Here, in @JACC_journals #Advances we present an AI approach to population-based SCA prediction using ECG+EHR.
A fantastic cross-country collaboration @broadinstitute@broad_ml4h@UW@MGHHeartHealth@MGBResearchNews@MACE_Lab_AI
🫀⚠️ SCOT-HEART changed cardiology with one simple idea:
👉 First scan. Then treat.
This is going to generate some hitching to some colleagues within the community 😁. Sorry about that.
And 10 years later…
the message is even more disruptive.
For decades, we built cardiology around:
👉 ischemia
👉 stress tests
👉 flow limitation
Find ischemia.
Open arteries.
Simple.
Except… it didn’t reduce hard events consistently.
SCOT-HEART helped expose the problem:
👉 Atherosclerosis—not ischemia—is the real disease.
At 10 years:
👉 coronary CT guidance reduced:
- coronary death
- non-fatal MI
despite:
❌ NO increase in revascularization
Let that sink in.
Patients did better NOT because we opened more arteries.
They did better because:
👉 we identified plaque
👉 intensified prevention
👉 treated biology earlier
The most important number may not be stenosis anymore.
It may be:
👉 total plaque burden
👉 plaque phenotype
👉 lipid-rich disease
👉 adverse plaque features
The paper says it clearly:
Patients with:
⚠️ low-attenuation plaque
⚠️ positive remodeling
had dramatically higher event rates.
This is the paradigm shift
From: ❌ ischemia-centered cardiology
To: 👉 plaque-centered prevention
And the implications are enormous.
Because suddenly:
👉 non-obstructive CAD matters
👉 “normal” stress tests become insufficient
👉 anatomy alone becomes incomplete
Even more interesting
The next frontier is already here:
⚡ Photon Counting CT
⚡ AI-driven plaque analysis
⚡ Radiomics
⚡ Quantitative phenotyping
My take
SCOT-HEART did not simply validate coronary CT.
It challenged the entire logic of modern cardiology.
We used to ask: 👉 “Is this lesion ischemic?”
Now the real question is: 👉 “How biologically dangerous is this patient?”
Bottom line
The future is not:
👉 detect stenosis
👉 react late
It is:
👉 detect atherosclerosis early
👉 personalize prevention aggressively
⚡ Because myocardial infarction often starts long before ischemia appears.
#SCOTHEART #CCTA #Cardiology #Atherosclerosis #PlaqueImaging #Prevention #PhotonCounting #AI #PrecisionMedicine
Proud to contribute to this ESC Statement; thanks to all co-authors for the excellent collaboration.
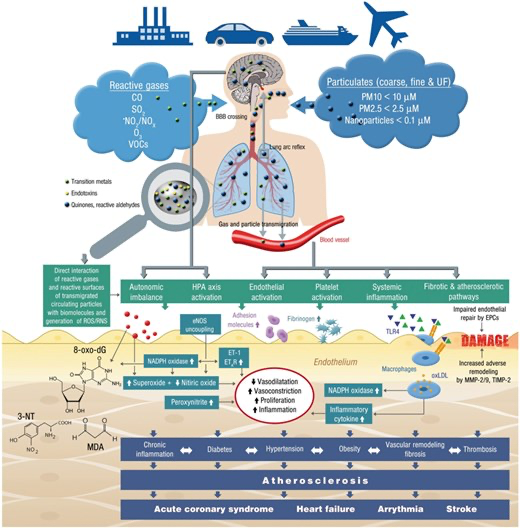
Air, heat, noise, and light pollution are clinically relevant CVD risk determinants.
@ESC_President@escardio@EAPCPresident@PTKardio@UMB_Bialystok
https://t.co/r7fp4N11BV
🚨 New paper out in Cardiovascular Revascularization Medicine 🚨
We analyzed 469,175 urban TAVR hospitalizations from 2016-2022.
The signal was clear:
🫀 Black and Hispanic patients had higher cardiometabolic burden
⚠️ Hispanic patients had higher mortality, MACE, AKI/dialysis, mechanical ventilation, transfusion, and cost
⚠️ Black patients had higher MACE, AKI, prolonged LOS, and CPR
✅ Stroke outcomes were similar across groups
The takeaway: TAVR has advanced dramatically, but equity in outcomes still needs to catch up.
Proud of our team and grateful to everyone involved.
https://t.co/1W52C1fLI3
#TAVR #Cardiology #HealthEquity #StructuralHeart #MedTwitter
🔍 Expert Analysis: The VESALIUS-CV, Ez-PAVE & GoFreshRx trials at #ACC26 collectively signal a maturation of #cvPrev guidelines.
Lipid mgmt➡️earlier, lower, & goal-oriented therapy
Hypertension care➡️structural lifestyle interventions
Read more🔗 https://t.co/c1vqcicHm5
With deep sorrow, I received the news of Dr. Eugene Braunwald’s passing, one of the greatest figures in world cardiology.
His scientific legacy, clinical vision, and immeasurable contribution to generations of cardiologists will continue to live on in our daily practice and in the history of medicine.
My heartfelt condolences to his family, friends, students, and to the entire cardiology community. May he rest in peace.
HF with mildly reduced EF (HFmrEF) sits between HFrEF & HFpEF; where does it truly belong?
A new HFSA Scientific Statement examines its epidemiology & pathophysiology & provides a comprehensive management framework for this understudied HF phenotype🫀
🔗 https://t.co/pP2WihJQxc
In an open-label, randomized trial in @NEJM, researchers compared an intensive LDL goal (<55 mg/dl) with a conventional one (<70 mg/dl) among patients with stable cardiovascular disease.