📊 Índice PROFUND
🔑 clave medicina geriátrica y paliativos para medir la mortalidad al año en pacientes pluripatológicos
🔎Evalua
✅edad ≥85
✅neoplasia
✅demencia
✅ingresos hospitalarios
✅dependencia Barthel <60
ayuda a adecuar el esfuerzo terapéutico. 🩺🏥 #Geriatría🏥
These guidelines provide principles of neuroprognostication for AIS pts admitted to the ICU & address reliability as well as prediction models in the context of counseling pts & families.🧠
https://t.co/frHRPC3Gr3
#SCCMNeuro#NeuroICU#NeuroX#NeuroTwitter
We’re heading to #ADS2026, and we're bringing our newest innovation in bedside brain monitoring. 🧠 Continuous, objective delirium monitoring is about to change critical care, and we can't wait to share an exclusive first look!
Visit the Ceribell exhibit and find out how we're transforming bedside delirium assessment.
Can't make it to the show? Request a virtual walkthrough here: https://t.co/Odb9jXjUEa
#deliriummonitor #criticalcare #neurodiagnostics
Lots of misunderstandings here.
First, this isn’t peer reviewed science. This is a press release. The level of evidence is essentially “trust me bro”
Second, sepsis early warning systems have been around for decades. This isn’t new. Most hospitals have systems like this.
Third, and most importantly, the way this intervention reduces the mortality *rate* probably isn’t actually saving any lives. What it’s doing is generating a ton of false positives. These people don’t need antibiotics but get them anyway, leading to side effects and resistance. But if you double the number of people with “suspected sepsis” in the denominator you make the mortality *rate* appear to drop. This is why in an actual published scientific paper we’d look at the number of deaths per year not just a rate. That’s also probably why this is press release and not an actual scientific publication…
🧠 Does adding a lumbar drain to an external ventricular drain improve outcomes in severe subarachnoid hemorrhage?
📊 A new secondary analysis of the EARLYDRAIN trial investigated the safety and efficacy of this simultaneous dual CSF drainage strategy in high-grade aSAH patients.
The study evaluated EVD-dependent patients to minimize clinical heterogeneity and revealed several crucial findings for neurocritical care.
✅ Safety: The addition of a lumbar drain is safe, with suspected infection rates (47.8%) and hemorrhage risks remaining statistically similar to using an isolated EVD (44.5%).
❌ Efficacy: Dual drainage does not independently reduce the risk of clinical vasospasm or improve 6-month functional outcomes when properly adjusted for the patient's initial injury severity.
⚠️ The Volume Paradox: The authors highlight a volume paradox where high-volume CSF drainage strongly predicts permanent shunt dependency, rather than preventing it or acting as a marker for functional recovery.
🧬 Ultimately, long-term functional recovery and mortality are heavily driven by nonmodifiable factors, specifically patient age and admission Hunt-Hess grade.
@mayoclinicnccfl@RabihTawkMD@berejah
What are your thoughts on the volume paradox and aggressive CSF drainage protocols? Let us discuss below! 👇
Reference:
Trevisi G, Palermo M, D’Arrigo S, Doglietto F, Albanese A, Sturiale CL. Safety and additive efficacy of dual CSF drainage (ventricular + lumbar) in severe aneurysmal subarachnoid hemorrhage: a secondary analysis of the EARLYDRAIN trial. Neurocrit Care. Published online June 8, 2026. https://t.co/6SCLxXgAde
Listen up!
Trying to get into a rhythm on how to approach pulsatile tinnitus?
Does pulsatile tinnitus get your heart racing?
This week’s @theAJNR SCANtastic has all you need to know!
https://t.co/BTI94N5Wsk
Pulsatile tinnitus is caused by turbulent blood around the petrous bone!
It’s like traffic: if you alter the flow of traffic, you will start to hear some noise & horns!
So what causes turbulent traffic?
1. Complex traffic patterns
If the roads are crazy, people get confused and drive crazy. Same w/flow from:
--AVMs
--dAVFs
--Tumors
--Diverticula
2. Diverted traffic
Nothing causes more chaos than making people go a different way than normal. Variant flow anatomy can cause pulsatile tinnitus:
--Large mastoid emissary veins
--Large occipital sinus.
3. Blockage of traffic!
If there is an accident, there is turbulence as people try to get around. For flow, blockages are stenoses:
--Carotid stenosis
--Transverse/sigmoid sinus stenosis
--Jugular stenosis
In this month’s @theAJNR, Zhang et al. found jugular stenoses were equally prevalent in both controls & pts w/pulsatile tinnitus
It raises the question if should we treat jugular stenosis!
Now hopefully your heart won’t skip a beat when you see a case of pulsatile tinnitus!
Follow @theAJNR and check it out for yourself:
https://t.co/BTI94N5Wsk
Did you know that continuous EEG detects status epilepticus significantly faster than short, isolated seizures in the ICU? 🧠⚡
A retrospective analysis of the CERTA trial evaluated 182 critically ill adults on continuous EEG to compare seizure detection times.
Here are the key findings:
⏱️ The median detection latency for Status Epilepticus (events lasting 5 minutes or longer) was 0 minutes, meaning it was often detected immediately upon starting the recording.
⏳ The median detection latency for short seizures (under 5 minutes) was 375 minutes.
💡 Why it matters: High seizure burden is associated with worse clinical outcomes in critical care patients. [4] Because status epilepticus is detected so much earlier than short seizures, understanding these latencies can help hospitals optimize their continuous EEG recording times and better allocate limited medical resources.
Reference:
Rossetti AO, Hahn CD, Novy J, et al. Status epilepticus is detected earlier than seizures on cEEG in critically ill adults. Neurocrit Care. 2026. https://t.co/cKsVTH583D
@wotivBill #BrinFreund @MayoFL_NeuroRes@mayoclinicnccfl
Letters to the editor
Veldeman: Commentary on: “Impact of Nimodipine-Induced Blood Pressure Reductions on Cerebral Autoregulation and Functional Outcome after Aneurysmal Subarachnoid Hemorrhage”
https://t.co/ELVT9DtrSV
Link: https://t.co/aAa7hJkSvr
@neuroritical #neurocritcare
Should Cardiac CT be SOC for Acute Ischemic #Stroke? Diagnostic Yield of Cardiac CT to Detect Cardiac Thrombi in Patients With Acute Ischemic Stroke (AIS of HEARTS) | @StrokeAHA_ASA@ChaturvediNeuro@msphippsmd https://t.co/EpxVP0UIlp
Early vs Delayed Extubation After Thrombectomy for Acute Ischemic Stroke. Pehaps we should ask patients what they prefer? @JAMANeuro https://t.co/ebaYfWK7O2
Did you know nearly half of acute ischemic stroke (AIS) patients may have hidden cerebral microbleeds (CMBs)? 🧠🩸
A recent 2026 study of Chinese AIS patients revealed a 49.1% prevalence of CMBs.
Key takeaways from the research:
🔬 Highest CMB rates were found in patients with Large Artery Atherosclerosis (59.4%) and Small Vessel Disease (47.5%).
📈 The top independent risk factors for CMBs are Hypertension and severe White Matter Hyperintensity.
💡 Interestingly, lower LDL cholesterol levels were linked to a higher burden of 3 or more CMBs [4].
🧠 Deep and infratentorial microbleeds were heavily associated with Small Vessel Disease and severe white matter injury.
These findings are crucial for neurologists and care teams weighing the risks and benefits of antithrombotic therapies for secondary stroke prevention.
How does CMB burden influence your clinical decision-making for stroke patients? Let us know below! 👇
Zhu R, Yang Y, Chen X, Hou L, Cheng X, He M. Prevalence and Risk Factors for Cerebral Microbleeds in Chinese Patients With Acute Ischemic Stroke. Brain and Behavior. 2026;16(6):e71495. https://t.co/V6FlRYndAU
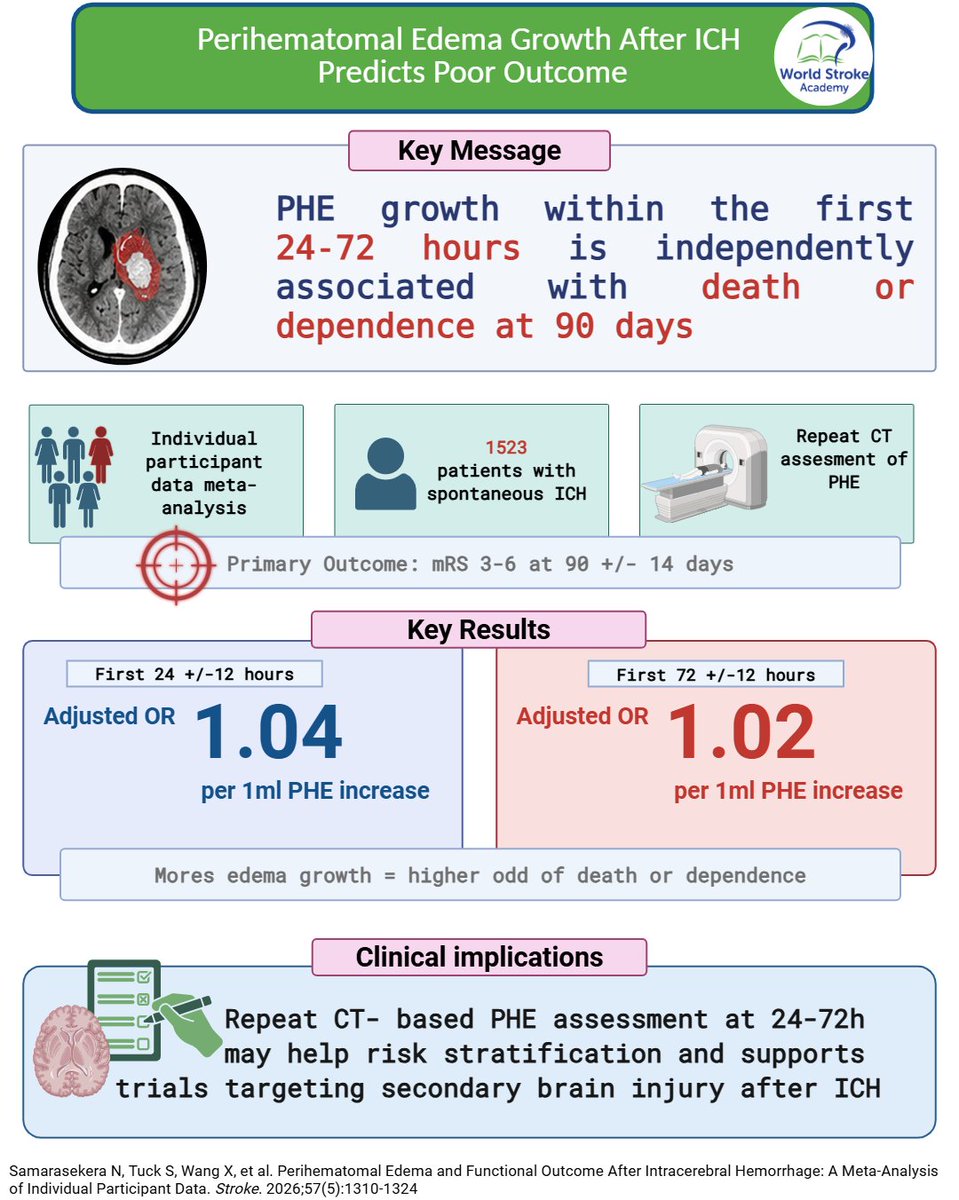
#MondayTIP#PerihematomalEdema
🩸After ICH, #PHE edema growth matters
📈In an IPD meta-analysis, PHE growth on CT at 24–72h was independently linked to death/dependence at 90 days
🎯Repeat CT may aid risk stratification and trial design
https://t.co/Ch6P4LDGyL
There hasn't previously been a treatment vs pancreatic cancer this successful. Striking improved (a > doubling) survival results @NEJM and @ASCO today with daraxonrasib, which also became available via an FDA approved early access program and began shipping to physicians this week @RevMedicines
https://t.co/e04jqJMPw0
Focused Update: Chronic Subdural Hematoma in #Stroke 🩸 Incidence is rapidly increasing, and recurrence remains high. Inflammation-driven neoangiogenesis and rebleeding sustain disease progression but are not targeted by current surgical treatments. https://t.co/XyZ9iQYw85
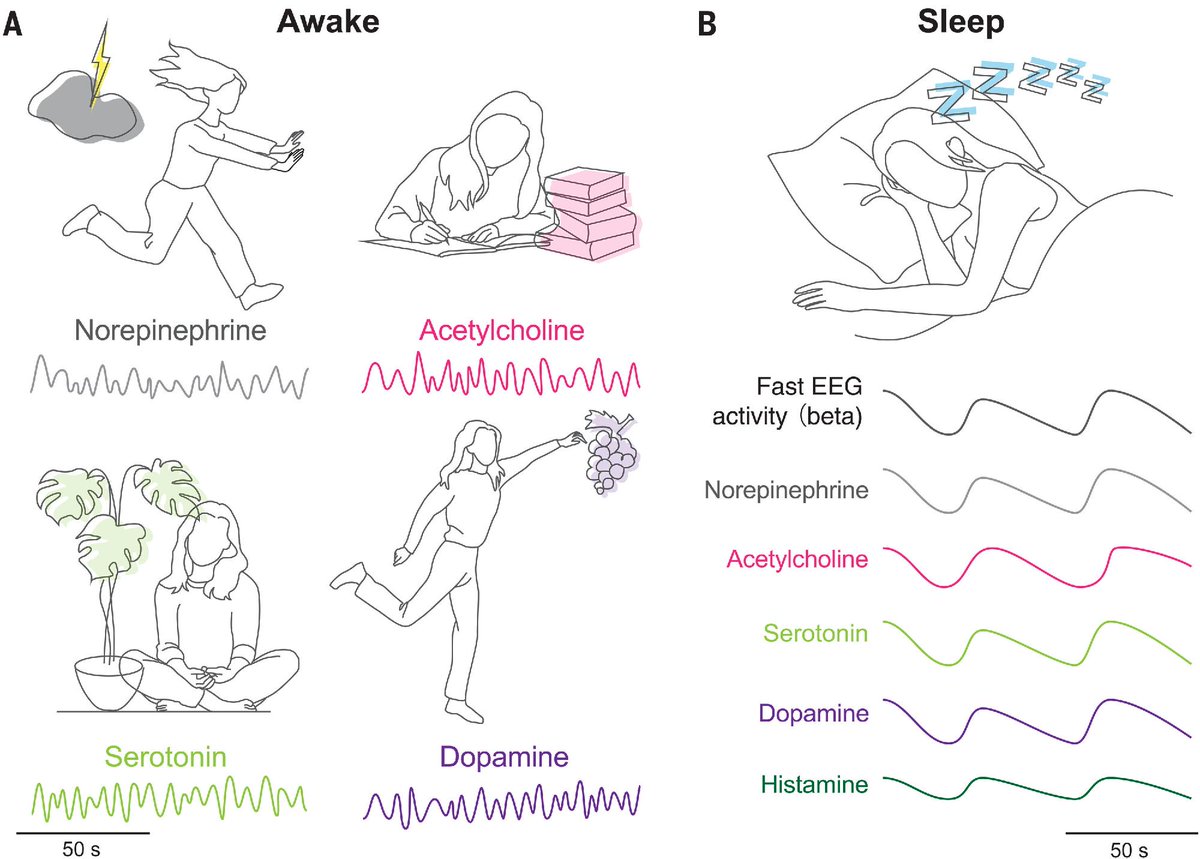
Recent studies have revealed the synchronization of neuromodulators including norepinephrine, serotonin, acetylcholine, dopamine, and histamine during sleep.
A new #ScienceReview explores what potential role the synchronization of these oscillations may play in health. https://t.co/fcDdHm1SDP
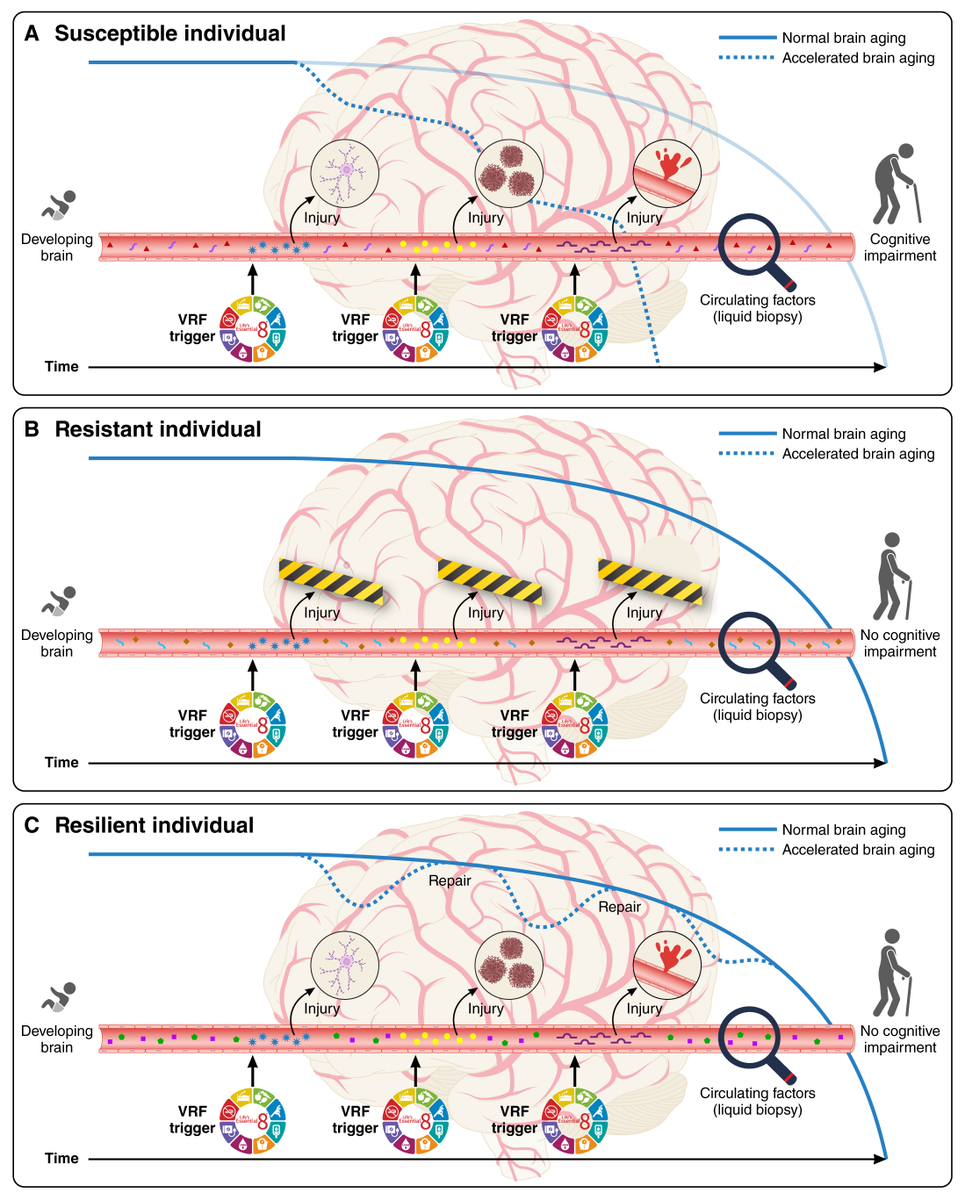
Published today, Vascular Contributions to Cognitive Impairment (VCID) and Brain Health: Clinical Update and Mechanistic Considerations.
This paper proposes that multi-mechanistic origins of VCID and time-appropriate interventions that complement VRFs modification are important to maintaining brain health and preserving cognitive function across the lifespan.
📷 Conceptual diagram of vascular contributions to age-related cognitive decline and worsening brain health.
We've written about AI-induced physician deskilling that has already surfaced
https://t.co/iMy6zyWnhZ @tberzin
AI-induced never-skilling among newly trained doctors, while not yet proven, is a serious concern that needs to be addressed @NatureMedicine@nliulab
https://t.co/yov3YvsGti



























![freemanwd's tweet photo. Did you know that continuous EEG detects status epilepticus significantly faster than short, isolated seizures in the ICU? 🧠⚡
A retrospective analysis of the CERTA trial evaluated 182 critically ill adults on continuous EEG to compare seizure detection times.
Here are the key findings:
⏱️ The median detection latency for Status Epilepticus (events lasting 5 minutes or longer) was 0 minutes, meaning it was often detected immediately upon starting the recording.
⏳ The median detection latency for short seizures (under 5 minutes) was 375 minutes.
💡 Why it matters: High seizure burden is associated with worse clinical outcomes in critical care patients. [4] Because status epilepticus is detected so much earlier than short seizures, understanding these latencies can help hospitals optimize their continuous EEG recording times and better allocate limited medical resources.
Reference:
Rossetti AO, Hahn CD, Novy J, et al. Status epilepticus is detected earlier than seizures on cEEG in critically ill adults. Neurocrit Care. 2026. https://t.co/cKsVTH583D
@wotivBill #BrinFreund @MayoFL_NeuroRes @mayoclinicnccfl](https://pbs.twimg.com/media/HKFYD5eWAAEY7vN.jpg)

![freemanwd's tweet photo. Did you know nearly half of acute ischemic stroke (AIS) patients may have hidden cerebral microbleeds (CMBs)? 🧠🩸
A recent 2026 study of Chinese AIS patients revealed a 49.1% prevalence of CMBs.
Key takeaways from the research:
🔬 Highest CMB rates were found in patients with Large Artery Atherosclerosis (59.4%) and Small Vessel Disease (47.5%).
📈 The top independent risk factors for CMBs are Hypertension and severe White Matter Hyperintensity.
💡 Interestingly, lower LDL cholesterol levels were linked to a higher burden of 3 or more CMBs [4].
🧠 Deep and infratentorial microbleeds were heavily associated with Small Vessel Disease and severe white matter injury.
These findings are crucial for neurologists and care teams weighing the risks and benefits of antithrombotic therapies for secondary stroke prevention.
How does CMB burden influence your clinical decision-making for stroke patients? Let us know below! 👇
Zhu R, Yang Y, Chen X, Hou L, Cheng X, He M. Prevalence and Risk Factors for Cerebral Microbleeds in Chinese Patients With Acute Ischemic Stroke. Brain and Behavior. 2026;16(6):e71495. https://t.co/V6FlRYndAU](https://pbs.twimg.com/media/HJzOJtMXoAAR10n.jpg)