85 to 90 percent of women physicians are eldest daughters.
That is not a coincidence. That is a pipeline.
Eldest daughters are trained, before age five, to over-function. They take on a parent's worry. They organize the family. They clean up without being asked. They do not ask for help, because they were rewarded their whole childhood for not needing any.
Then they walk into medicine.
A career that demands hyper-responsibility, hypervigilance, perfectionism, and silent sacrifice does not have to ask these women to give those things. They were giving them before they could read.
The system is not stumbling into a burnout problem. The system is recruiting from a pool of people whose entire childhood was a training program for it.
This is what pediatrician and certified coach Jessie Mahoney has been finding when she asks the room. In every group, in every retreat. Maybe one or two women are not eldest daughters. The rest have been carrying something since before they could spell their own name.
Most of those women blame themselves. "Why don't I have boundaries?" "Why do I over-function?" "Why can't I delegate?"
Because at five years old, your family rewarded you for over-functioning. Because every teacher praised you for it. Because the medical training system selected for it. Because every job since has reinforced it. The pattern is older than your medical degree by twenty years.
The other piece nobody names: by the time these women are in their fifties, they are carrying eldest-daughter responsibility for aging parents AND running a department as chief AND running a household. The role does not retire when the children do. It just compounds.
Jessie's reframe is the part worth bookmarking.
The "hero" framing is the trap. Eldest daughters were made the savior of the family before they could read. Then medicine made them the savior of the patient. Then the department made them the savior of the team. At every stage, they learned that if they did not do it, terrible things would happen and it would be their fault.
Awareness is the first move. Non-judgment is the second. Excellence is not doing everything yourself. Excellence is letting other people do their jobs.
You are allowed to gift some of it back. You can ask your siblings to carry the aging parent. You can let your medical assistant do the medical assistant's job. You can stop covering the gap that nobody actually asked you to cover.
Most eldest daughters in medicine have never asked for help. When they finally do, they discover people are willing to help. The asking was the whole obstacle.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
What is the one task you have been carrying for your family or your team that no one ever actually asked you to carry?
#ThePodcastbyKevinMD
A low-cost and expert-driven medical technology is being used in rural areas in Australia!
The machine is operated by a sonographer remotely (using a gaming controller) and helps perform an ultrasound examination.
Doctor shortages shouldn't mean that patients have to travel more (sometimes for no medical reason), but to use technologies that can extend the reach of medical care.
This is a perfect example of that!
Interesting case
CXR: Consolidation in the right upper lobe with inferior bulging of the horizontal fissure. A central lucency suggests cavitation. Small right pleural effusion
@IhabFathiSulima@hemo_shk
Show more ...👇👇👇
#Mondaytip
🧠 New @American_Stroke#Stroke Guidelines
✔️ TNK = first-line option for IVT
✔️ EVT expanded (large cores & basilar ≤24h)
❌ No aggressive BP or glucose lowering
👶 First pediatric AIS guidance
⏱️ Systems of care matter more than ever
https://t.co/XbT7cJasYG
One of our residents, Dr Kartavya, has been missing since yesterday. If anyone has any information on his whereabouts, please contact.
Also, please circulate this.
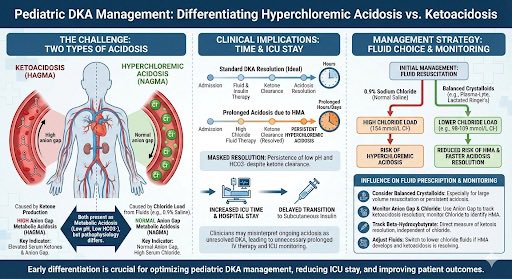
In DKA don’t chase the pH /bicarb
You need to know when ketones have cleared (via direct measurement or anion gap)
Otherwise may end up treating an iatrogenic hyperchloremic acidosis with iv insulin delaying transition to subcut
This is why we go on about balanced crystalloid
📢We're wrapping up the year with 2 final webinars & kicking off 2026 with the first confirmed!
💪Stroke Spasticity: https://t.co/7NzGm9IsRc
🧬Factor XI/XIa Inhibitors: https://t.co/6AwjtalSsO
🚀New Antithrombotic Strategies: https://t.co/Bv7ICl0Z6H
All FREE #StrokeEducation!
updating the IBCC chapter on ECMO
any recent advances or important articles I should include?
please share any recent practice-changing insights you’ve had about ECMO 🙏
(it’s one of the harder chapters to update due to high volume of new research)
“Happy Birthday, Dr. Andreas!🥳🥳 Wishing you the best for your future and everything ahead my friend!
We all learn from you keep up the Great Work!🤩
You are a rare Gem! @ecgandrhythmRoe
🔷 SOFA 2.0 – A Quick Guide for clinicians & researchers
long-awaited SOFA 2.0 was presented at Hot Topics @ESICM LIVEs & simultaneously published in JAMA on October 29! 7 🇧🇷 authors!
🔷 How should it be implemented in clinical practice & research?
👇🏻
https://t.co/MAPdqy3O0H