Presented at #ASCO26:
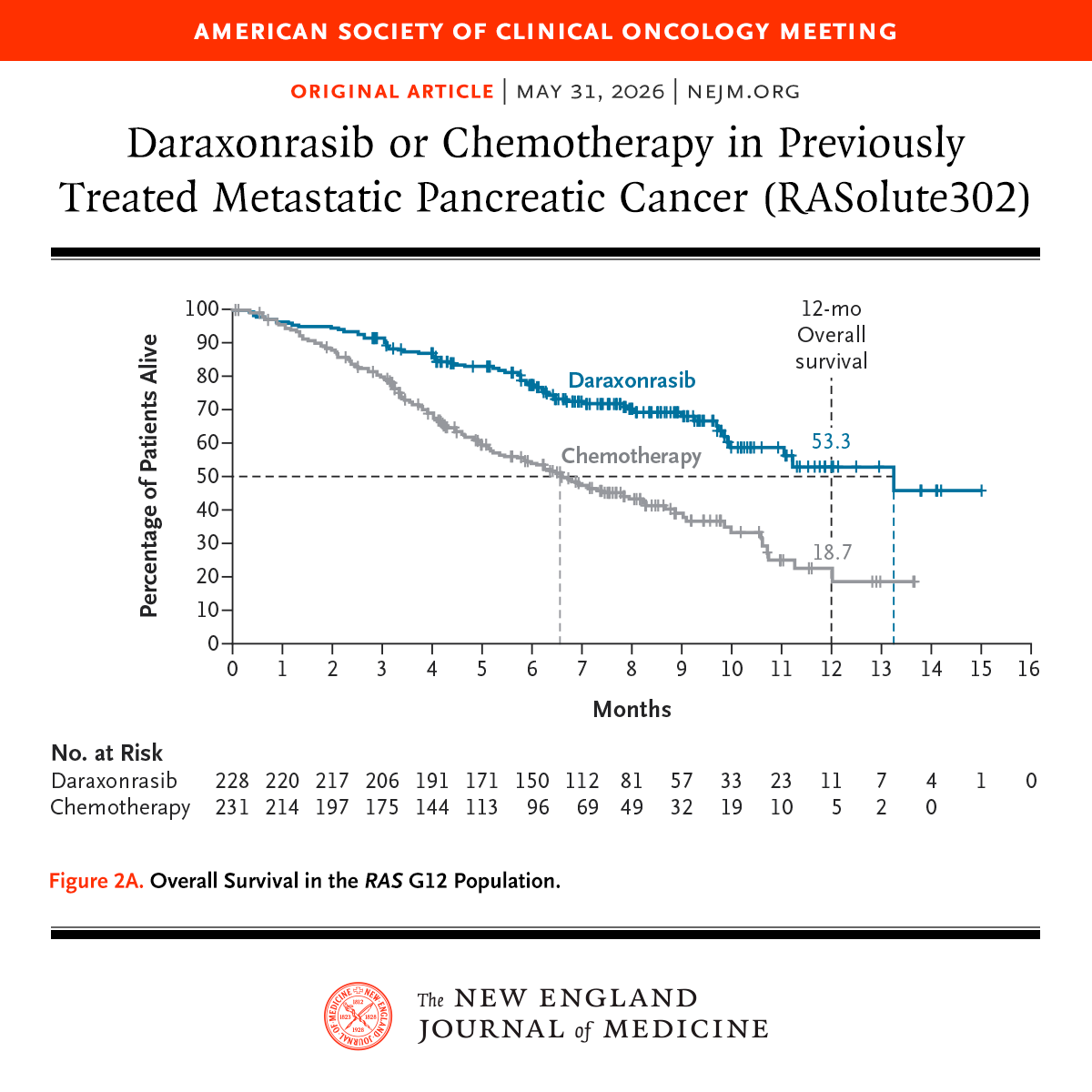
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
Absolutely practice changing!! One of the most stunning developments in the treatment of patients with metastatic pancreatic cancer !! It is one of the rare moments in oncology which you will always remember ! Like the imatinib, trastuzumab presentations @ASCO#ASCO26@OncoAlert
I hope you didn’t miss out on @paul_wongg talk at #AHPBA26 on an externalized pancreatic stent during robotic Whipple!! Looking forward to the manuscript! 💫
@TClancyMD told me in November, two weeks post Whipple that I would enjoy a walk on the beach in March and not feel the effects of the surgery.
I doubted him.
Today I took that walk and he was right. I didn’t feel the effects of the surgery.
I even stopped to capture an image of the moment.
Praise God and thank you Dr. Clancy.
Looking forward to a new position as Director of Interventional Cardiology at Mass General Brigham. With incredible colleagues throughout the system, we will build the most comprehensive IC program internationally.
Congrats to the GGI team for an fun BWH #Boston10K that raised money for pancreatic cancer research! Sweats, grazes and muscle cramps to show for our efforts!
@BrighamWomens@BrighamSurgery@BAA
“No children are dying on my watch,” said Rubio. It's blatantly false. Credible estimates count 190K deaths so far.
In Kenya, I am documenting for a film devastating impact, including this child's starvation & many deaths directly caused by Rubio’s actions. See my @msnbc clip
Congratulations to Kenneth Tanabe, MD, Co-Chief of MGH Division of Gastrointestinal and Oncologic Surgery, who was appointed President-elect of the Society of Surgical Oncology! The SSO is the world’s leading professional org dedicated to advancing the field of surgical oncology
Shimul Shah, MD, MHCM, new Chief of MGB Transplantation, has been appointed President-elect of the Americas HepatoPancreaticoBiliary Association! The AHPBA is one of the world’s leading professional orgs, dedicated to advancing the field of liver, pancreas, and biliary surgery.
It seems few people know what an “indirect cost” is or why it has to be 40-60%.
The reason the government forced universities to raise their indirect costs up to (typically) 40-60% was to force a huge amount of regulations on the universities while also minimizing the bookkeeping to comply with those regulations. This includes the work by contract managers, compliance lawyers, accountants, safety management, etc., who are required by the government per the terms of the contract. If universities had to allocate all those categories of labor to each contract hour-by-hour it would require too much bookkeeping, which would waste money. (I’m setting aside for now the question of whether or how much the regulations are wasting money and only discussing how you bookkeep the effort to comply with the regulations.)
So to save money, while also requiring universities to do these types of work, the government requires universities to roll those categories of labor into “cost pools” that must be allocated as a percent of the technical work in each of the contracts. While the actual “overhead” might be only 15%, these pooled labor charges that are required by the government are typically much more.
Second, the government doesn’t allow the universities to figure out their own indirect rates. These rates are determined by the federal government through audits every couple of years. The government then sends a document telling the university what rate to use for its cost pools. For example, the University of Colorado was told by the DHHS to use 54% (https://t.co/zLuEjM75st) and U. Nebraska was told by DHHS to use 55.5% (https://t.co/z2ZQ2cIkLK). 40-60% is not only reasonable to fulfill the terms of the contract, it is the rate that the government tells the university it can charge for all the work the government requires the university to do.
So if the government wants to reduce the indirect rate to 15%, then it needs to do one of these two things:
Either
(A) eliminate all the federal regulations that force the universities to do those categories of work (compliance, accounting, management, safety management, tracking harmful chemicals, etc.)
Or,
(B) stop requiring universities to pool those real costs into the “indirect cost” category and allow universities to include them in the “direct costs” of the contract.
If the government chooses (A), then the safety rails have been entirely removed. (Even if the government lowers the regulations without entirely eliminating them, the costs they impose will still be real costs that probably come out to more than 15%.)
Or, if it chooses (B), then the direct costs will go way up and research will actually be less efficient because all the bookkeeping, not more efficient.
But if the government caps the indirect rate at 15% without doing either (A) or (B), then it will be impossible to do research for the federal government without going bankrupt. That’s the worst possible choice. It will kill research in the US. Is that what we want?
I can explain it for you but I can’t understand it for you. It’s up to the reader not to be ignorant.
NIH announces new funding policy that rattles medical researchers
"We’re all reeling," Dr. George Daley, the dean of the Harvard Medical School, wrote NPR in an email. "This would decimate medical research."
https://t.co/AVTvkTuZ5T