Raised in rural eastern WA. Left to learn a trade - ultimately interventional cardiology @BWH. Returned to rural eastern WA 2 practice interventional cardiology
@CMichaelGibson Performing ❤️ caths in cath lab is like reading 📖 in library: every day looks the same to uninitiated; every day is different to the expert
The Open Evidence clinic encounter tool creates a note that’s written as if my scribe was me, but me with unlimited time. It also shows what clinical trial data and guidelines think about my plan. It’s amazing. https://t.co/xfT9cH2FjW via @NYTimes
Our new paper is out in the European Journal of Preventive Cardiology #EJPC looking at body composition changes in patients taking GLP-1 receptor agonists while going through our Pritikin intensive cardiac rehabilitation program at @UCSDCardiology
https://t.co/kNSedHYvAo
Congratulations to my mentees who led this study: UC San Diego medical students Ian Jennings and Kristine Ly, UCSD undergraduate Mariam Marooki, and research coordinators Gavin McLLaren and @marissadzotsi . Not all weight loss is equal and quality of weight loss matters. When patients lose weight on GLP-1 RAs, the muscle they keep matters just as much as the fat they lose.
Across 468 patients, those on GLP-1 RAs improved their fitness and lost fat while holding their skeletal muscle mass steady. In a structured cardiac rehab setting built around supervised resistance training, aerobic exercise, we did not see the muscle loss that has been a concern with this class of medications.
Just as important, everyone in cardiac rehab improved their fitness by roughly 3 METs, whether or not they were on a GLP-1. That is a meaningful number. Each 1-MET improvement is associated with a 10 to 25% reduction in mortality, so a gain of this size translates into a substantial improvement in cardiovascular outcomes. It is a powerful reminder of what structured cardiac rehab delivers.
The takeaway for preventive cardiology: GLP-1 therapy works best as part of a comprehensive program. Combined with structured exercise and nutrition, patients gain multiple cardiometabolic benefits and preserve the muscle that keeps them strong and functional. We need to utilize cardiac rehab more! @MWilkinsonMD@hsbhatia@dranulala@purviparwani@DrMarthaGulati@VietHeartPA@EJPCEiC@SamiaMoraMD@EugeniaGianos@JamalRanaMD@Bweber04@MonSangh@ditchhaporia@khurramn1@MichaelJBlaha@Jcontreras75@emilyswlau@EmilyManoogian@SatchinPanda
Trump said something outside a press gaggle that I don’t think enough people caught.
A reporter called him out on the corruption. He gave three responses.
1. I have the right to do it.
2. He’s not stealing that much. A billion or two billion dollars. Not that much money. Classic Trump.
3. People don’t care.
That’s the permission structure. Our collective apathy is what they’re using to justify everything happening in Washington right now.
Please stand up and prove him wrong.
Role of Physical Activity in Obesity Treatment and Cardiometabolic Health: A Scientific Statement From the American Heart Association: @CircAHA
🥸So -> single treatment modality, physical activity and exercise programs are unlikely to result in clinically meaningful weight loss (ie, at least 5% loss of initial body weight) unless aerobic physical activity levels are exceptionally high!
😱 Congratulations to @AHAScience
👇👇👇
Donald had a temper tantrum on national television and walked out of an interview simply because Kristen Welker presented him with a basic fact.
Note to other journalists: now is the time to pile on. He won't be able to handle it.
🚨 BREAKING
The first drug where AI designed both the target and the molecule has just published Phase II results in Nature Medicine.
Patients with a fatal lung disease gained lung function in 12 weeks.
Current treatments only slow the decline. This is different.
🧵 Here's what just happened (and why it matters for medicine).
#AIDrugDiscovery #ArtificialIntelligence
Extraordinary study in JAMA IM confirms what many of us have warned against: "pay-for-performance" incentives in medicine reward "teaching to the test" with potentially harmful results
In this quasi-experimental study, incentivizing doctors to control blood pressure (BP)...
1/X
30 yrs ago yday, as per the Budapest memo guaranteeing their territorial integrity, Ukraine handed their final nuclear warhead to Russia.
Also gave entire command firing chain, delivery vehicles Tu-22s & 1068 Kh-55 cruise missiles. Which have been fired at Ukraine in this war
“The White House said that medication lists in executive summaries, like the one they provided on Friday, are often abbreviated for readability and relevance.”
No. This is not true. The medication list provided by the president’s doctor is assumed to be a complete list, not just the medications the White House wants the public to know about. What medications were omitted?
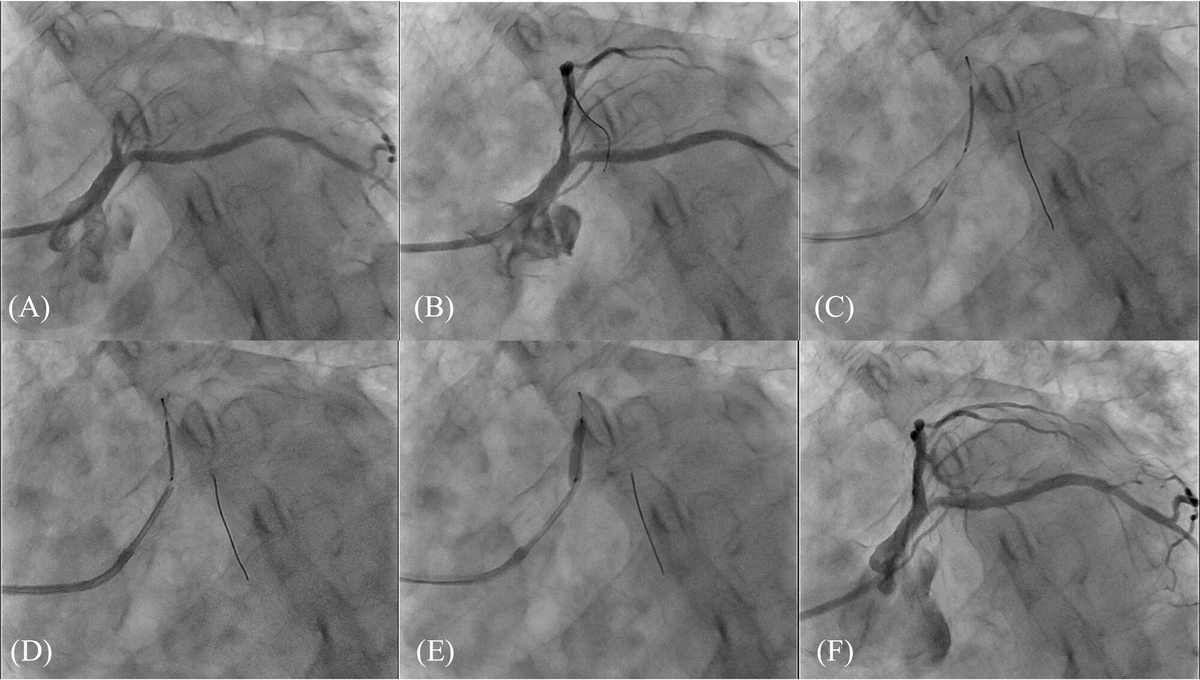
Welcome to the Ostial Stenting With Guide Extension Catheter Tip Technique: a novel approach enabling precise ostial and bifurcation stenting using a guide extension catheter https://t.co/Alfop7WzBQ @ccijournal
I’m glad Dr. Barbabella’s overall assessment is that the president is well. A few questions.
1. Why did the president have another coronary artery CT? He was last scanned in Oct. We don’t typically scan patients 6 months later unless we are concerned about a finding on the initial scan. What prompted the repeat CT?
2. The report notes that the president’s ankle edema is improved compared with last year, but at the president’s last annual exam he had no edema.
3. Dr. Barbabella attributes the president’s bruising to his aspirin and handshaking. But what about his left hand? Also, why is the president, taking a dose of aspirin 4x higher than recommended for cardiovascular protection?
4. Why was the president again given a MOCA dementia screening test? He’s had 3 in the recent past.
5. Did the WH medical team address the patient’s apparent daytime fatigue and sleepiness?
6. AI assessment the president’s “heart age” is that of a much younger 66-year old man is not a clinically utilized tool.
7. The president himself called this visit a semi-annual physical. Going forward, is the new schedule every 6 months? Why more frequent than the traditional yearly exam?
Coronary microvascular obstruction: the "no-reflow" problem that haunts STEMI care. New ESC clinical consensus on pathophysiology, prevention & management: a must-read. Read more in #EHJ.
https://t.co/WWlcFSfVyj
#cardiotwitter@ESC_Journals@escardio
With everything we are hearing right now about ticks this seems like good information to share.
“Here’s what I’ve learned after more ticks than I care to count.
First, whatever your uncle told you, forget it. No matches. No nail polish. No Vaseline. No soap on a cotton ball. All of those do the same terrible thing, they stress the tick out, and a stressed tick empties its gut back into the bite before letting go. Which, if you think about what that actually means for a second, is literally how Lyme and the rest get transmitted so you’re not speeding up its exit. You’re making it throw up into you.
Fine-tipped tweezers. Grip right where the mouthparts enter the skin, not the body, the head. Pull straight up, steady, no twisting, no jerking. It’ll feel like it’s resisting because it is, the mouthparts are barbed. Just keep the pressure on and it lets go in a few seconds. If a piece breaks off in the skin, leave it alone. Your body pushes splinters out. Digging around with a needle does more damage then the fragment ever would.
Clean it with alcohol or soap. Wash your hands.
Now here’s the part most people skip: don’t flush the tick.
Tape it to an index card. Clear packing tape right over the body, write the date and where on your body it was, and stick the card in a drawer. If you come down with anything weird in the next 30 days, rash, fever, joint pain, that flu-that-isn’t-flu feeling, that tick goes with you to the doctor. Some labs will test the tick itself, which is faster and often more reliable than waiting for antibodies to show up in your own blood. A dated tick taped to a card is one of the most useful things you can hand a doctor who’s trying to figure out what’s wrong with you.
The other thing worth saying out loud: if the tick was engorged when you pulled it, and you can’t swear it was off your body within 24 hours, call your doctor that same day. Don’t wait for a rash. Fewer than three out of four Lyme cases even produce the classic bullseye. A single preventive dose of doxycycline within 72 hours of a deer tick bite cuts the Lyme odds way down, and most docs in tick country will write that prescription without giving you a hard time, especially if you walk in with the tick taped to a card and a clear timeline.”
In a large Texas cohort called ARIC, Jonathan Cohen found the lottery winners. A few hundred people whose PCSK9 gene carried loss-of-function mutations. Their LDL cholesterol was 28% lower than average, and their coronary heart disease risk was 88% lower. Published in NEJM in 2006.
These people hadn't done anything to earn it. A single gene was broken, and their livers ran a cholesterol-clearance program that the rest of us need daily medication to approximate. Most of them didn't even know.
We've spent 20 years approximating. Statins work, and roughly half of patients quit within 12 months. PCSK9 injectable antibodies work better, at $5,850 a year, with uptake rates so poor that cardiologists write papers about it.
Today @NEJM published a trial that stops approximating. VERVE-102 is a base editor. One IV infusion rewrites a single DNA letter in liver cells, shutting down PCSK9 the way it's already shut down in Cohen's lottery winners.
Heart-2 trial: 35 patients, six doses. The highest dose cut LDL 62% and suppressed PCSK9 protein 88%. Effects sustained 18 months and counting. No serious adverse events.
The gap between the people who won the genetic lottery and everyone else just got an engineering solution.
A mathematician at Bell Labs noticed that the scientists who won Nobel Prizes and the ones who never amounted to anything were equally smart, equally hardworking, and equally credentialed, and the only thing that separated them was a single question almost nobody is brave enough to ask themselves before they die.
His name was Richard Hamming.
He spent 30 years at Bell Labs, in the same building as John Tukey, Walter Brattain, and a long list of physicists who took home Nobel prizes for work they did down the hall from his office, including the legendary Claude Shannon.
His invention of error-correcting codes made modern computing possible. He has won the Turing Award. And all the while he was creating his own legacy he was secretly doing a study on the people around him.
The study was straightforward. 2 Teams. The legends and the lost. Same I.Q.s. Degrees same. Same desk hours. Same access to the world’s best resources.
And yet, at the end of 40 years in their careers, one group had changed entire fields, and the other group could not be remembered by their own colleagues five years after retirement. He wanted to discover what the actual difference was.
In March 1986, he stood before 200 researchers in a Bellcore auditorium and told them what he had seen.
He said it all came down to one question. And hardly anyone he ever met was willing to ask it directly.
He called it the Friday-afternoon ritual. He spent years blocking out his Friday afternoons and not doing anything productive with them every week. No experiments. No meetings. No deliverables.
He called it Great Thoughts Time. He sat down with a notebook and asked himself a couple of questions in order. What are the most relevant problems in my discipline? And why I am not working on either of them.”
Most weeks, the answer was the same, he said. For a week now he had marched confidently in a direction he did not think was the most important direction. He was a goer. He worked a bit. He was getting clean results that would publish in respected journals. (
And for five days straight he'd been lying to himself about whether any of it mattered.
The reason almost nobody does this ritual is because the honest answer is unbearable. The thing is that if you sit down on a Friday afternoon and say out loud that you are not working on the most important problem in your field, now you have to do something about it.
You have an immediate change in direction, or you have to keep lying to yourself every week from that point on. Most people choose the lie.
In the short term it’s cheaper, but over a career it’s more expensive.
Hamming took the ritual a step further in the Bell Labs cafeteria. He began approaching scientists he barely knew, asking them what they thought the most important problems in their field were.
A week later he would ask them why they had not worked on these problems. Eventually people wouldn't have lunch with him. “I had to keep finding new tables,” he said.
Nobody had a good answer for that, and being around someone who kept asking it made every meal feel like a performance review.
The line that broke me is the line that most people skim over in the transcript. His words: If you do not work on an important problem you are unlikely to do important work.
That’s not motivational line. It is a rational one. You cannot make a great result from a problem that does not matter. Input restricts the output. The choice of the problem is the ceiling of the career.
The transcript has been freely available on the internet for almost 40 years. Stripe Press published the complete lectures as a book. Naval Ravikant quotes it all the time. It’s still given out to new hires at every serious engineering lab in Silicon Valley.
Most people will not run the ritual this Friday. They will be busy. They always are.