Medical Oncologist in Recife, Brasil. Particularly interested in breast and gynecological oncology, new developments in molecular oncology and survivorship.
1st line ET plus palbociclib vs standard mono-CT in high-risk HR+ /HER2- metastatic BC and indication for CT: primary results from the randomized phase IV PADMA study in @ESMO_Open.ET+Palbociclib improved TTF and PFS, with higher hematological toxicity. https://t.co/EhNMUKJuoY
ADCs enable an improved delivery of chemo, expanding its activity, but not necessarily decreasing its side effects. Why is that? How can we reduce the toxicities of ADCs?
Glad to share our @NatRevClinOncol article on how to optimize the safety of ADC! 🧵
https://t.co/QcpeKTosCq
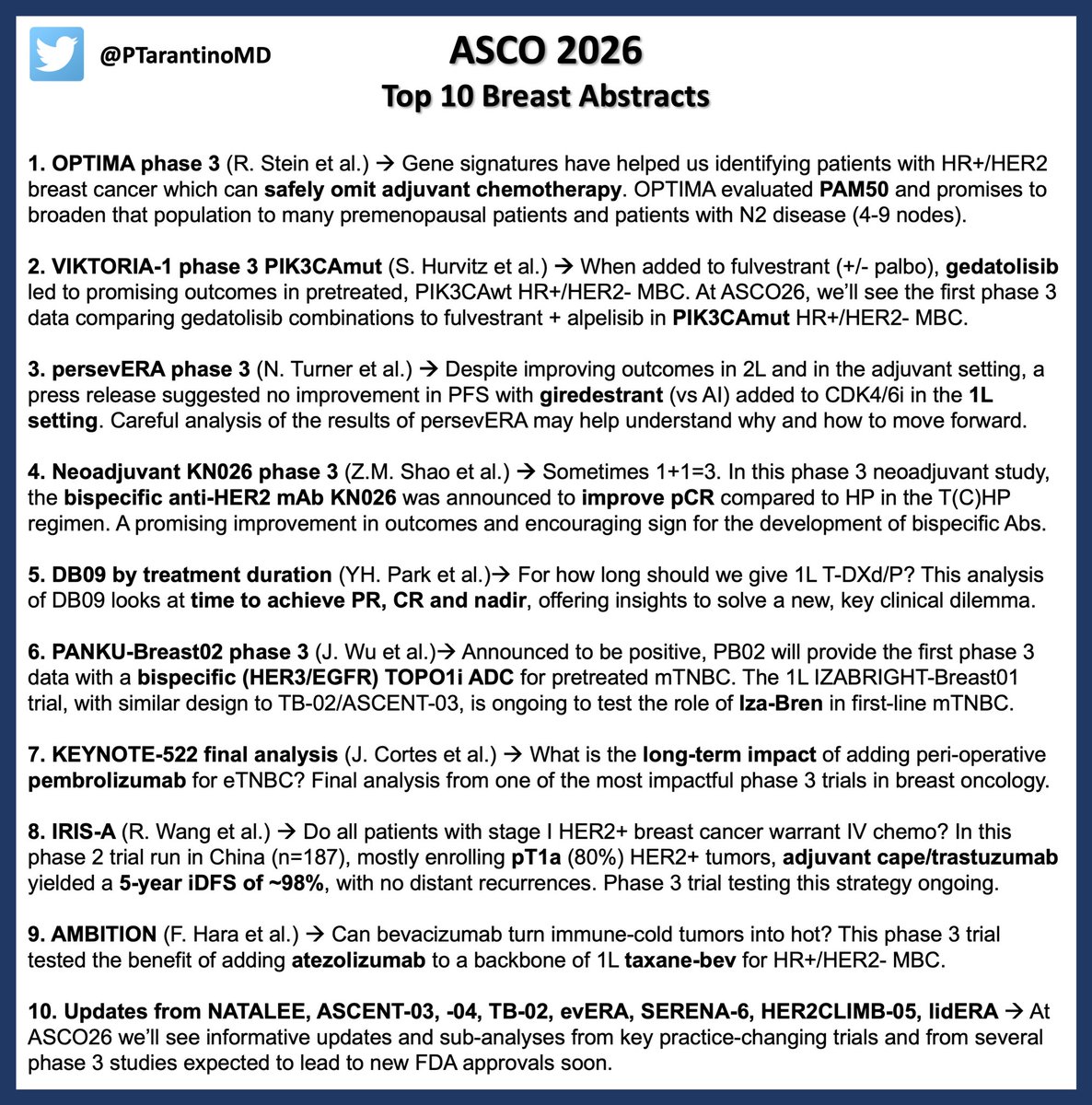
Only few days to #ASCO26. For breast oncologists, this edition will deliver a new promising biomarker to spare unnecessary chemo, informative updates from practice-changing trials across subtypes, and major innovations coming from China. See you in Chicago next week! #bcsm
🎯🎯.- How to apply the current evidence in the treatment of mCSPC!! Excellent review.🙌
https://t.co/OFccsZ439w
👉.- The new molecular precision "triplet intensification" is here.
👉.- A HRR (BRCA2+) alt and pTEN loss population have a poor prognosis.
👉.- We need to better biomarkers profile in this setting
@OncoAlert@APCCC_Lugano@ANZUPtrials@myESMO@GuardConsortium@fedelosco
🧬 NGS is NOT just “detected” or “not detected.”
👉 The real question: Did we look properly?
🔹 Coverage = Did we look at that region?
🕳️ If an exon isn’t covered → it’s a blind spot.
🔹 Depth = How many times did we read it?
📉 Low depth = ↑ risk of missing low-frequency variants.
💡 Think of NGS like CCTV:
🎥 Coverage = How many cameras are installed?
🔁 Depth = How many times each frame was reviewed?
🚫 No camera? You missed the theft.
🤷♂️ Blurry frame? You can’t ID the culprit.
🔍 What to ask your lab (ALWAYS):
✔ % of target covered at ≥100x
✔ Mean & minimum depth per gene
✔ Any dropouts or low-confidence zones?
📊 Take-home:
➡️ Coverage = Where you looked
➡️ Depth = How well you looked
You need both to treat with confidence.
📖 Save this before your next MDT or tumor board.
🧬 More genomics insights coming 🔜
#OncoTwitter #MedTwitter #PrecisionOncology #NGS #Genomics #MolecularOncology
@OncoAlert@myesmo@esmo_open@ASCO@tmprowell @vinrajs @marklewismd@oncology_bg@DrChoueiri@Liz_ORiordan@rsm2800@mtmdphd@JackWestMD@JankovicK
```
Pleased to share the first series of pts who experienced recurrence on adjuvant abemaciclib+ET:
➤ 9.2% (15/163) recurred
➤ 50% ER loss post-tx
➤ 90% TP53-pathway alterations post-tx
➤ Median 1L m+ tx duration: 3.0 mo (IQR 1.6–5.0)
https://t.co/5Jpzq8uyc2
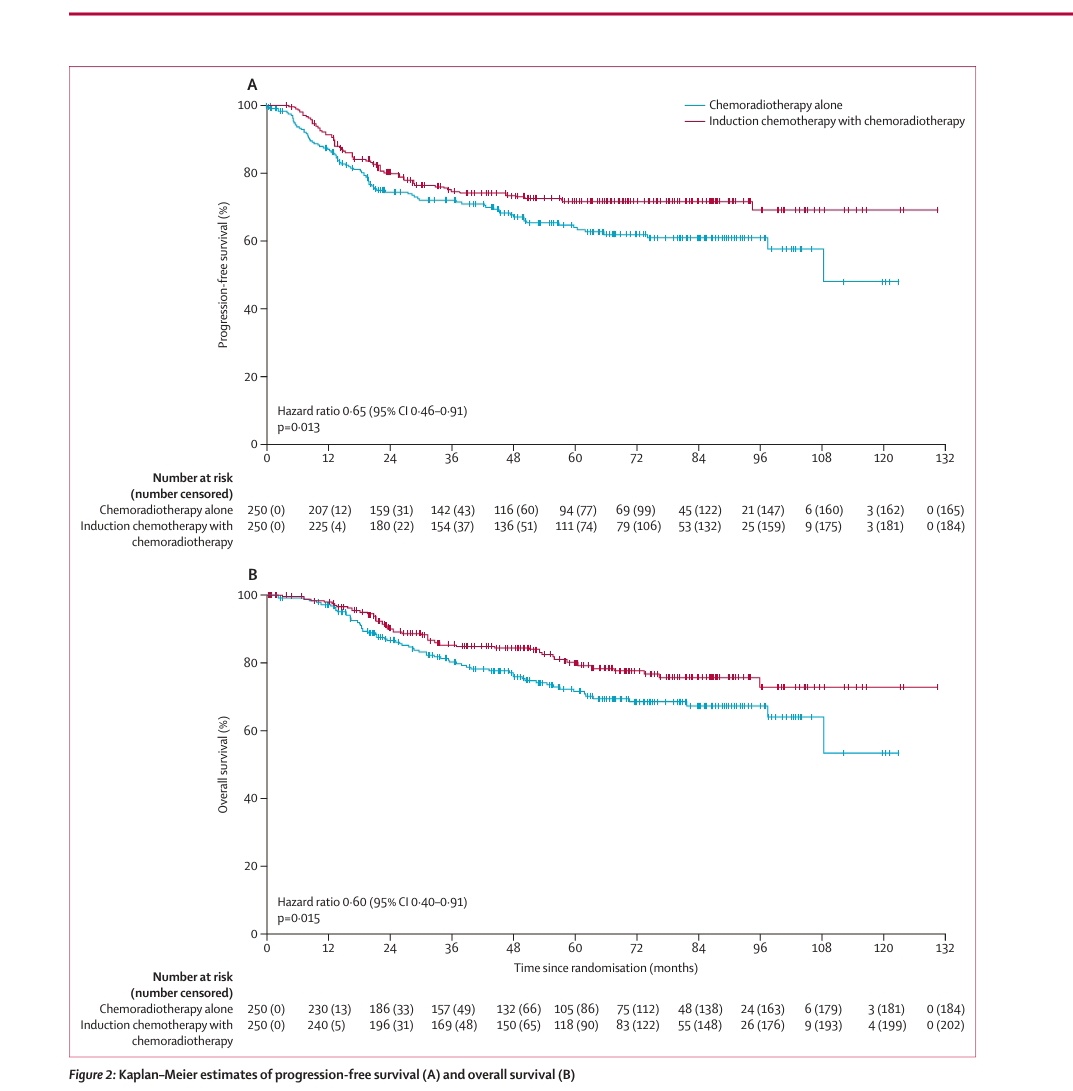
So finally it is published. Much awaited Interlace trial for locally advanced ca cervix shows 8% OS benifit at the end of 5 years for neo adjuvant chemo followed by CTRT vs CTRT alone. HR 0.60
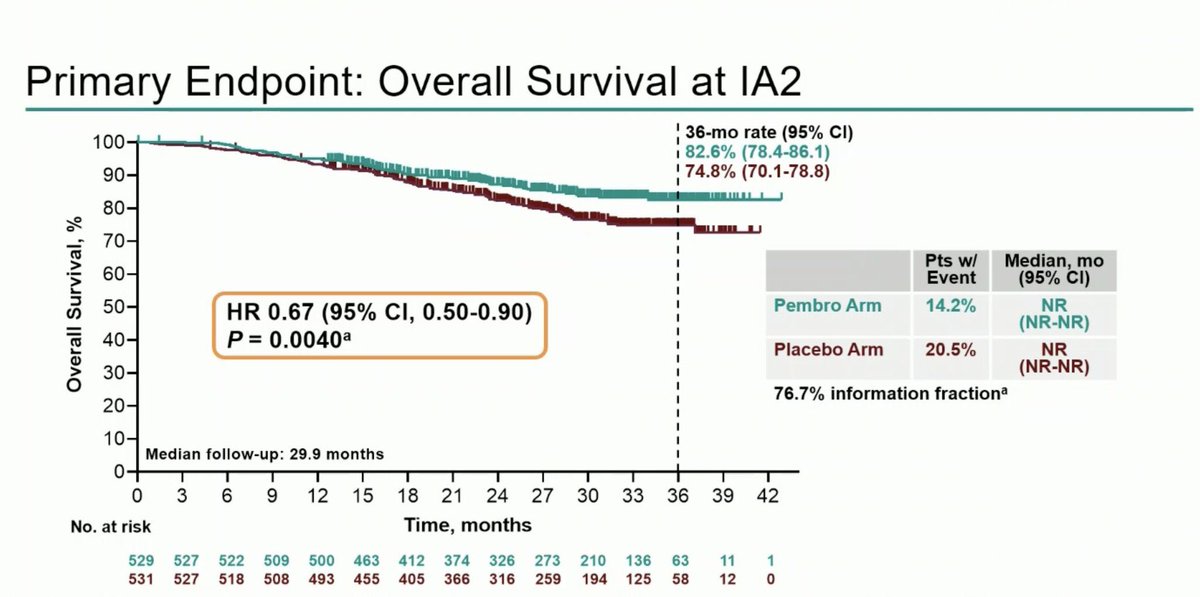
Now how will you fit keynote A18 into this- pembrolizumab with CTRT did show OS benifit with HR of 0.67 . @myESMO@Larvol@ASCO@BanerjeeSusana@5_utr@Larvol@brunolarvol@OncBrothers@OncoAlert
Nice slide to show outcomes of perioperative chemo vs CTRT for all trials in GE junction and Stomach adenocarcinoma. Good for discussion with patient in clinic . @myESMO