A common sub-analysis in clinical trials is the association of the type of response with survival outcomes, often showing that responders tend to do better. One issue with these analyses is that the causation is often misinterpreted.
Patients are implied to have experienced better PFS/OS because of achieving a better response. In truth, the opposite may be true: patients with less aggressive tumors are more likely to stay on treatment for long enough to achieve a deep response.
The statistical analysis is also tricky. The Kaplan-Meier PFS/OS curves for responders are usually flat for several months, suggesting “guarantee time bias”: patients who eventually become responders must survive and be progression-free long enough to be classified as responders.
In a nutshell, patients may not survive longer because they achieve a deeper response; rather, patients with more favorable timor biology and longer disease control are more likely to remain on treatment long enough to achieve partial or complete response.
The same issue applies to analyses of drug toxicities, dose reductions, and irAEs: patients must remain alive and on treatment long enough to experience these events, which can make these groups appear to have better outcomes unless appropriate time-dependent or landmark methods are used.
A thorough discussion of this bias is found in this article, published in the inaugural year of @JCO_ASCO (vol 1, 1983).
Thanks to @ValenzaCarmine for sharing this article with me.
https://t.co/XzZ09Mdn28
Your clinical trial baseline is a mix of liver mets, lung mets, bone mets, and primary tumors.
You compare it to post-treatment samples from different sites.
The "treatment effects" you find will mostly be tissue site differences.
This is a fantastic #OpenAccess review in @CellGenomics!
scTrends: A living review of commercial single-cell and spatial 'omic technologies
Perfect for that overview for your trainees. Find link below.
Are metastatic #cancers more like their normal origin or target tissues? Our work in @ScienceAdvances systematically compares the #transcriptomics of primary and metastatic #tumors to healthy tissues in a #PanCancer, genome-wide manner! #metastasis 🧵1/10 https://t.co/DWdkyMOXsv
3) Yet in my past 25 years as a computational biologist I have repeatedly seen some of the best, most technically gifted and intellectually deep, bench biologists treat computationally differently. Any computational result that supports a claim they wish to make is sufficient ->
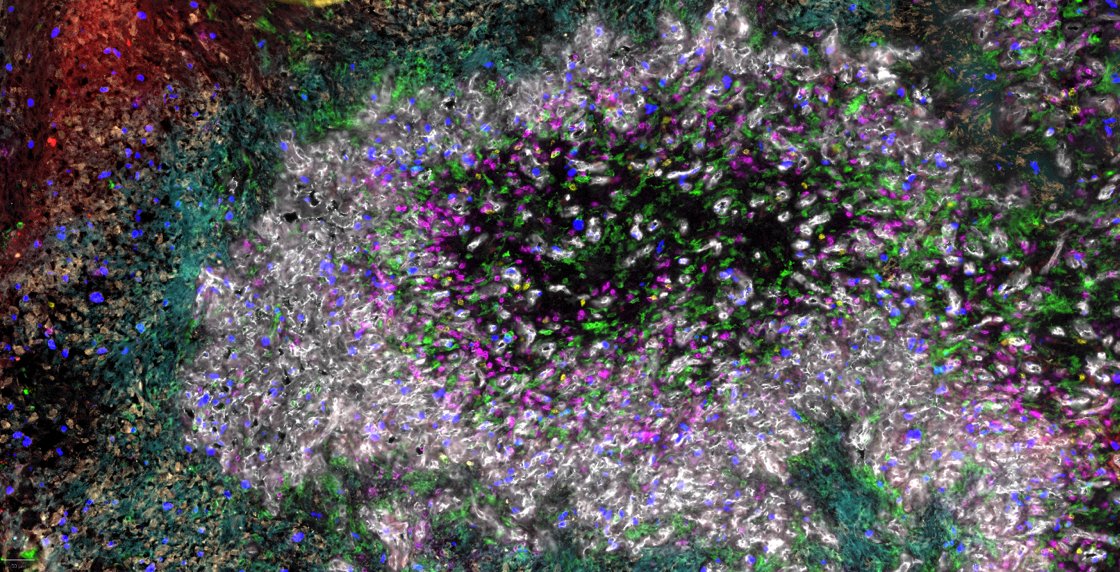
We’re excited to share our preprint on spatial organization in glioblastoma: https://t.co/OTaanCDDXG. We combine spatial transcriptomics (Visium) and proteomics (CODEX) to reveal a five-layer organization of cellular states and highlight a role of hypoxia as tissue organizer. 1/
9 months after presenting #ASHG19 the paper is finally out! Congrats @True_Gene for your amazing work on grouping human tumors by cancer cell intrinsic expression! Check out how MSLN and AKT are related in #PDAC#PancreaticCancer#openaccess
https://t.co/B4sN4nxo7G
The last portion of my graduate work, highlighting mesothelin-associated biology buried within patient tumor tissue datasets, is out today:
https://t.co/JHj9Qiguzp
#histoepigenetics@histoepigenetic
Happy to share our latest study on site-specific turnover of DNA methylation: https://t.co/HR5PF4NIW4 Genomic maps of DNA methylation, while informative about genome activity and cell state, provide only a freeze frame and do not reveal the dynamics of DNA methylation.