British Army EM/PHEM Consultant (PGY-13), Travel enthusiast and Foodie. Interests include POCUS, Human Factors, strong coffee and good steak. All views my own.
UK HEMS - a very different profile compared to the "average" US HEMS program.
Also, not mentioned, there are zero single engine helicopters used for HEMS in the UK.
(<4% of US HEMS programs staff with physicians)
https://t.co/8ru77wFKZR
New in EMJ - free open access:
Endovascular resuscitation: an expert practice review
A practical overview of REBOA, SAAP and ECPR for emergency physicians managing the sickest patients in shock or cardiac arrest.
Please read / comment / share
DOI: 10.1136/emermed-2025-215376
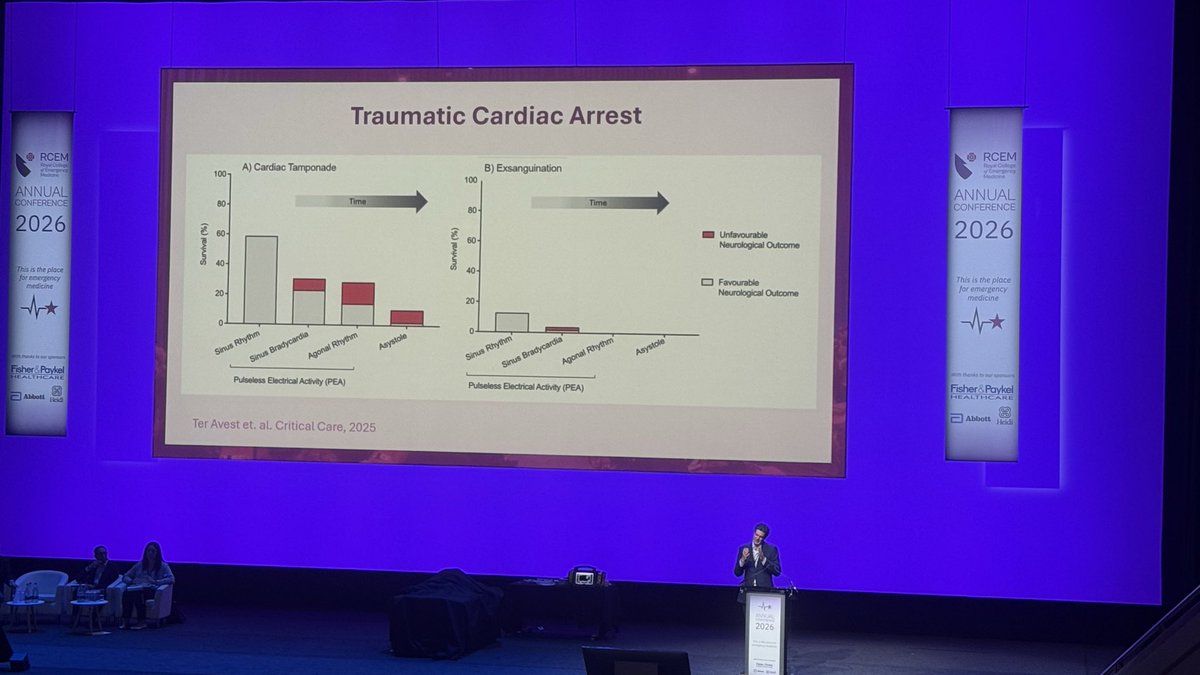
Definition of trauma cardiac arrest. Zane Perkins @RCEMevents Conference 2026.
Define by lack of coronary perfusion. So you can tell time since arrest by changes in cardiac rhythm.
At 1 minute heart slows.
At 5 minutes bradycardia established.
At 10 minutes PEA.
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
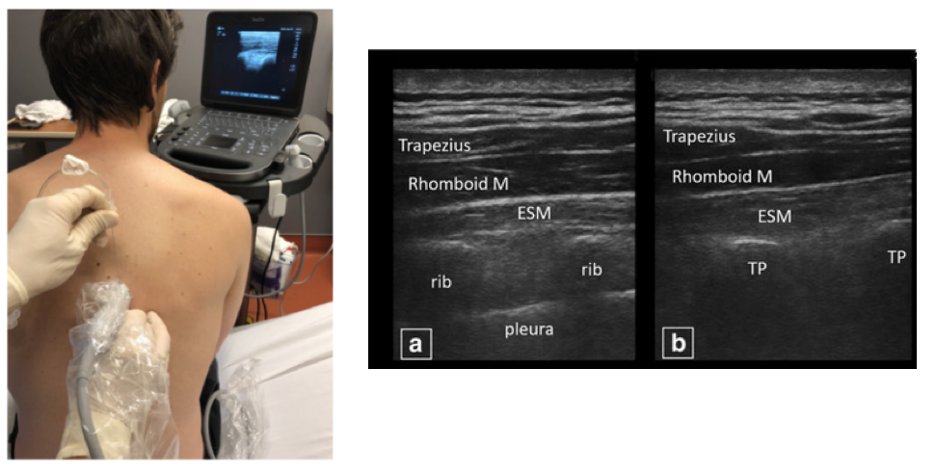
🫁 Rib fracture pain isn’t “just uncomfortable”, it can be quite painful and potentially harmful when undertreated.
Learn how to use PoCUS-guided:
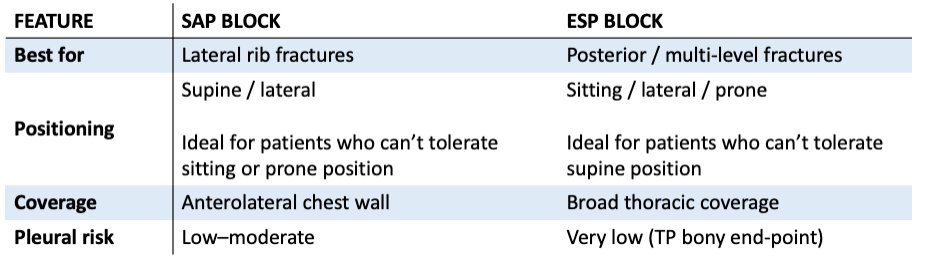
✅ Serratus Anterior Plane blocks
✅ Erector Spinae Plane blocks
https://t.co/ZQAIvOpv0q
Spoon fed guide on the blocks in order to help improve ventilation, improve pain, reduce opioids, and change patient trajectories.
Two excellent days of CPD @trauma2030 - inspiring, innovative and thought provoking stuff as always from the @LDNairamb and @London_Trauma teams. Great to catch up with some old friends and make some new ones too!
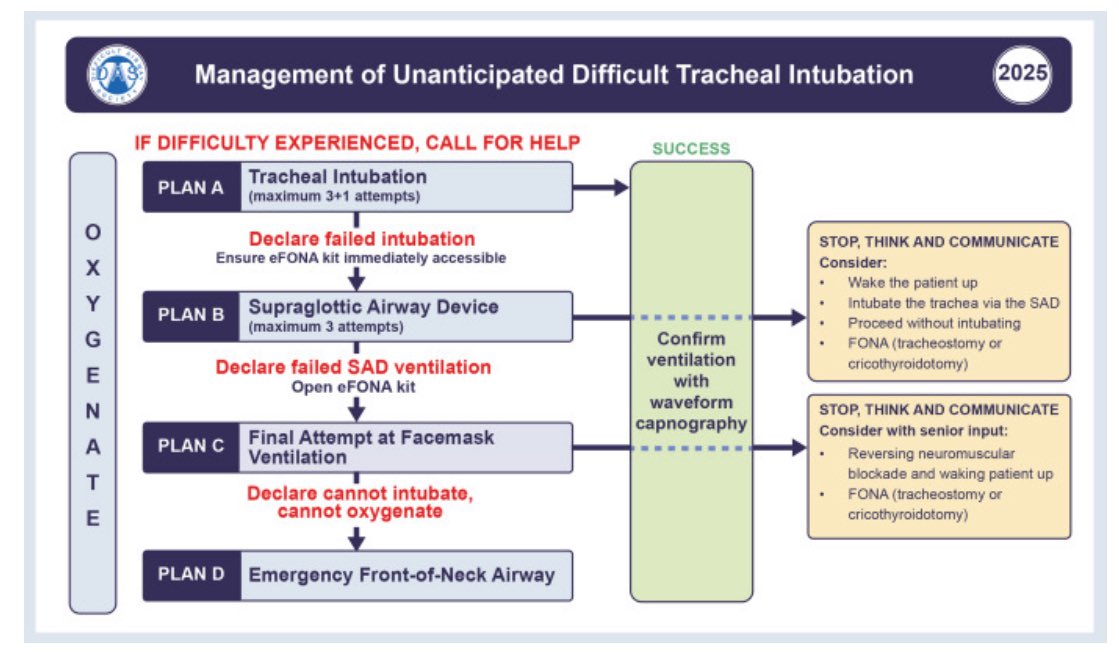
New DAS guidelines out today.
Had a quick spin through I can’t see any huge changes that will alter prehospital practice.
Nice to see integration of vortex style approach to FONA kit though: onto chest > open > use
https://t.co/EohtompLoJ
It's 4:00 AM and a patient comes in with a stab wound to the heart.
Repair it by 4:02 and the patient will walk out in a few days.
Wait until 4:05, and he'll be wheeled out in a bag.
🧵regarding a few surgical pointers on repair of traumatic cardiac injuries.
(1/ )
Taking battlefield medicine to the next level🩺🪖
The British Army has introduced a new role in a bid to save lives
Combat Life Savers — bridge the gap between the basic first aid skills held by all soldiers and medically trained personnel
🔗https://t.co/uPFcd97A6s
A recent systematic review with meta-analysis of 6 RCTs found that in neonates undergoing emergency intubation, VL was superior to DL for first-pass success with a NNT of 6.
This is particularly helpful for those of us that do not routinely intubate neonates but may, on rare occasions, have to do it under less than ideal conditions. It's a reminder that our ED's need to be pediatric-ready -- which includes the proper airway equipment for small children.
https://t.co/ryiSCKt99p
#emergency #emergencymedicine #criticalcare #icu #science #data #research #army #armymedicine #airway
Cardiac arrest isn’t a diagnosis in the same way as headache isn’t a diagnosis, jaundice isn’t a diagnosis, chest pain isn’t a diagnosis, abdo pain isn’t a diagnosis. If we keep trying to find magic bullets that treat the presenting complaint, we’re relying on luck to innovate.
The key to resuscitation of patients in cardiac arrest is not dissimilar to other clinical presentations:
What is the underlying pathophysiology? How can we best optimise the patient’s physiology under CPR conditions? What specific treatment(s) are options for this particular patient?
“Physiology-Guided CPR” 🚨🚨🚨
The inclusion of “physiology-guided CPR” in the ERC resuscitation guidelines marks a significant milestone in progress.
So here are my reflections on the journey we have undertaken and thoughts on the future directions
#SPEAR
🧵
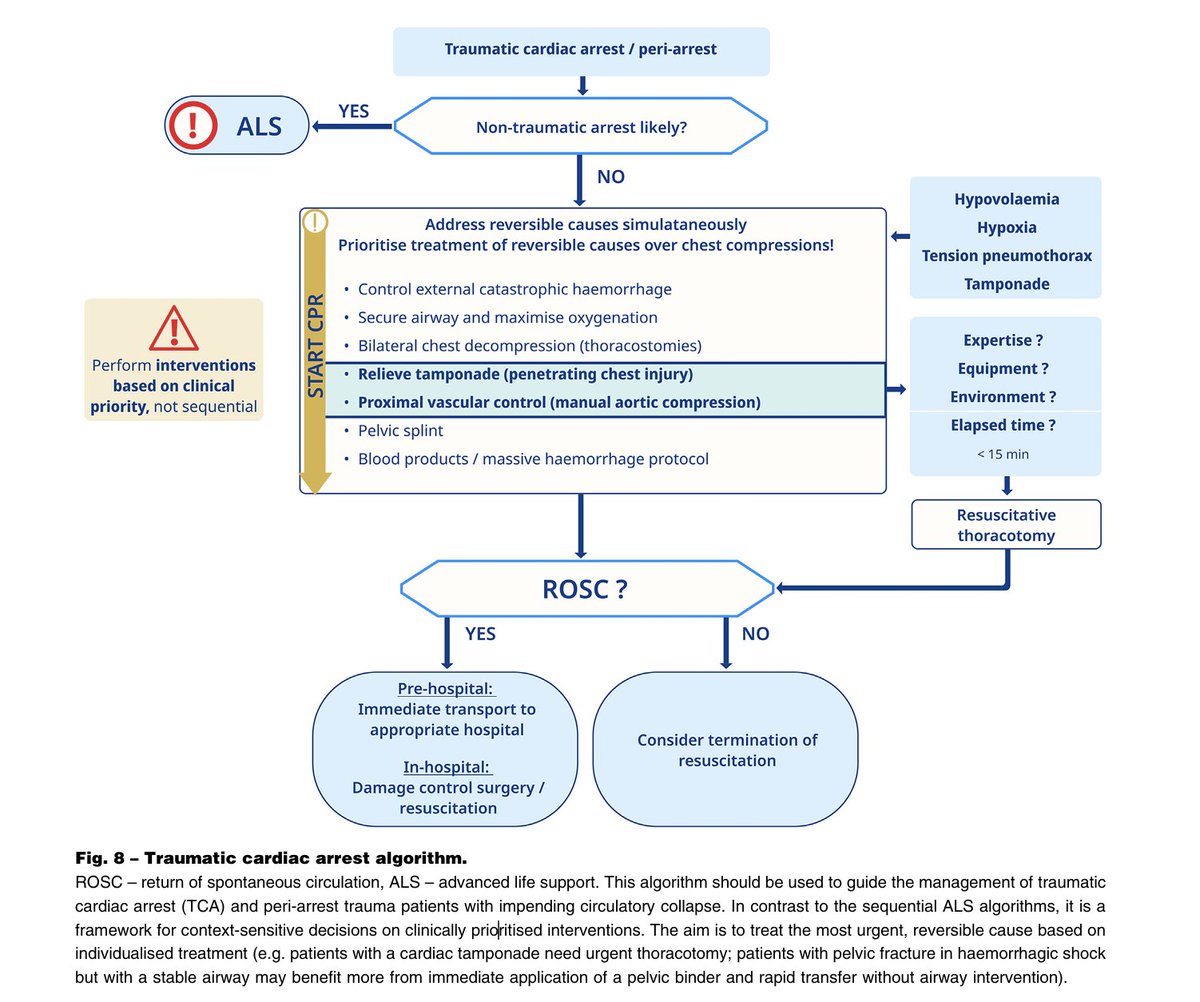
Perhaps ‘bye bye REBOA’ is an oversimplification. The guidelines do not allow for nuance; I am sure my collaborators at @LDNairamb will have some opposing views on this
TCA is a broad church of pathology (as is indeed, medical cardiac arrest) - A Zone 1 REBOA in a peri-arrest traumatic subdiaphragmatic haemorrhage may be a useful bridge to prevent TCA), or if the balloon is deployed very close to the “time zero” it may be a useful tool to augment coronary perfusion and myocardial rescue when used with rapid volume resuscitation and ICM
Never say never……
Super interesting concept on the new @ERC_resus 2025 guidelines!
TCA is a framework for context-sensitive decisions on clinically prioritised interventions
The incredible support of this amazing people is invaluable.
Your expertise and dedication is instrumental to its success #TALS (trauma advanced life support)
Level 2 trauma course
@UHSFT