Medical devices ≠ phones or laptops.
Repairs require specialized procedures, FDA regulations, calibrated tools & safety checks.
One-size-fits-all right to repair policies ignore this complexity - and will put patients at risk. Medical devices should be excluded.
More bad news for the health plans concerted attempts in litigation to do an end around on the #NoSurprisesAct. In tennis terms, the plans have been beaten 6-0, 6-0 in no less than 4 previous cases, w/ federal courts dismissing their lawsuits against both firms that engage in IDR and physician groups.
Now, @BCBSTX case against HaloMD has been dismissed w/ prejudice by a TX federal court, for the 5th consecutive dismissal.
Make no mistake: the health plans are "marketing" their lawsuits in DC and using it in their advocacy calling for fundamental changes in the NSA. How is that strategy working out for y'all now?
The link below describes the case but does not yet have the dismissal update included.
Let's see: The @texmed had 4 successful cases against the federal gov't (no less) on the prior administration's rules implementing the NSA. So the physicians & IDR firms are undefeated and health plans are 0-5--#justsayin
https://t.co/LbjtlNYUcp
Exhibit A for passage of the No Surprises Act Enforcement Act (H.R. 4710) is demonstrated by the experience of Radiology Associates of North Texas (RANT), one of the largest independent radiology groups in the US.
According to Radiology Business (5/20/2026), "Radiology Associates estimates it has prevailed in about 95% of finalized IDR disputes with Blue Cross Blue Shield of Texas, the state’s largest insurer. However, more than $3.5 million in awarded balances remain unpaid. RANT estimated that $1.64 million of this total has been outstanding for over 120 days. As of Tuesday, BCBS Texas has paid approximately 2% of awarded balances."
RANT is not alone in this experience.
The Emergency Dept. Practice Management Association (EDPMA), representing well over 60% of the ED groups providing care to ED patients (or organizations supporting the provision of care), released a study in April 2026 of over 659,000 successful NSA IDR claims won by its members in 2025. Yet, 48% of those IDR determinations were not paid within the 30-day period required by law. The total outstanding of award determinations not paid by the health plans exceeded $245,000,000.
Congress must pass HR 4710 to give CMS the same enforcement authority it has over hospitals and physicians that it does not currently have over health plans, mainly the ability to assess Civil Monetary Penalties (CMPs) for non-compliance with the NSA.
Radiology Associates of North Texas says it will waste over $51M on costs related to No Surprises Act https://t.co/VipNBtfaaG
Thanks to @RepAaronBean and @GregMurphyMD for leading an important discussion about the No Surprises Act.
Thanks to IndeMed's chair, @DrBruggeman, for representing physicians and patients.
You can tune in live right now:
https://t.co/FBMpqJncqY
For the 3rd year running, New York's legislators have rightfully rejected stripping away an important protection that ensures Medicaid patients can get the emergency and specialty care they need.
🚨 Now as final budget negotiations close, it's time for them to stand firm!
New York hospitals ask state to block Anthem policy that fines them for out-of-network care https://t.co/IhssBFBWVZ
#AnthemWatch#NY#medtwitter#healthcare
America's physicians are frustrated. The healthcare community is calling on Congress to crack down on insurers dodging No Surprises Act payments. No more payment delays, no more loopholes. Read the letter: https://t.co/jciit09vuB
This is the ultimate midwit healthcare take.
No, 32 countries have not “figured out” universal healthcare.
The UK has “free” healthcare, and roughly 1 in 3 cancer patients in England still fail to start treatment within 62 days of urgent referral.
Canada has “free” healthcare, and the median wait for neurosurgical treatment is around a year.
Australia has “free” healthcare, and over half the country still buys private insurance despite paying for a public universal system with their taxes.
Switzerland has universal coverage, because residents are required to buy private insurance. There is no government system where benevolent bureaucrats tuck you in at night with a warm blanket and an MRI appointment.
The actual lesson from other wealthy countries is not “they figured it out.”
America’s system has huge problems. Our prices are insane, insurance markets are distorted, and hospital systems are cartelized. Our regulations make care more expensive than it needs to be.
Yet we still guarantee access to even the 8% who don’t have coverage. We give easy routes to qualify for medicaid for those with disabilities.
Pretending the rest of the world solved healthcare because they slapped the word “universal” on a rationing scheme is not analysis.
It is bumper sticker policy for people who think access means having a card in your wallet while you wait a year to see the doctor you need.
New from me for @Paragon_Inst:
Physician-owned hospitals can increase competition and improve affordability.
But the ACA effectively barred new ones from opening and existing ones from expanding.
It’s time to lift these restrictions.
Read more ⬇️
Terrific development here, and bravo @CalHospitals!
@alan_condon reports:
"Anthem’s new policy is trying to force hospitals to solve a problem Anthem created,” CHA President and CEO Carmela Coyle said in a May 4 news release. "It’s illegal, ignores the agreements Anthem has with its enrollees, and will lead to further financial stress for California hospitals and the communities they care for during an extremely unstable period in healthcare."
https://t.co/xDwtPiIN9h
Excellent insights from @PresAmerMed on why more vigorous enforcement of the #NoSurprisesAct is urgently needed.
"[I]t’s clear that some health plans are undermining both the letter and the spirit of the #NSA. Unless federal agencies step in with robust enforcement and transparency, the careful balance #Congress created will unravel, putting #patient access at risk and threatening the viability of independent physician practices.
Health insurers are pointing their fingers.
But the facts point right back.
Insurers like Elevance Health are now claiming that the very system designed to protect patients, the No Surprises Act and its Independent Dispute Resolution process, is driving costs, being misused by providers, and operating outside its intended purpose.
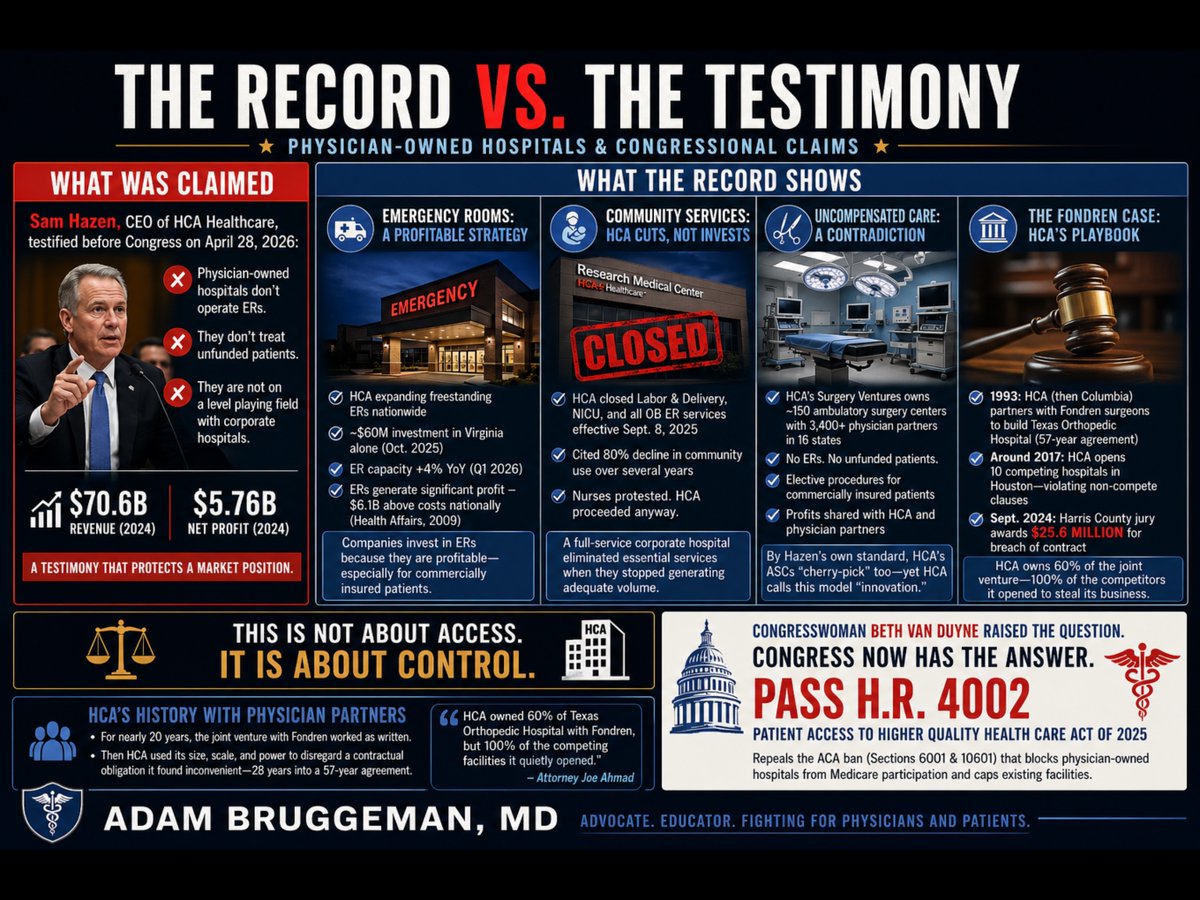
Yesterday, Sam Hazen, CEO of HCA Healthcare, sat before the House Ways and Means Committee and argued that physician-owned hospitals are not on a level playing field with corporate hospitals because they lack functioning emergency rooms and do not treat unfunded patients. Hazen delivered this argument while representing a company that posted $70.6 billion in revenue and $5.76 billion in net profit in 2024. He was not offering a neutral observation about healthcare access. He was protecting a market position.
Congresswoman Van Duyne did not let the testimony pass unchallenged. She pointed directly to HCA's own Research Medical Center in Kansas City, Missouri, which closed its labor and delivery unit, its neonatal intensive care unit, and all associated obstetrics emergency services effective September 8, 2025. HCA cited an 80 percent decline in community use of those services over several years as its justification. Nurses at the facility publicly protested the planned shutdowns and called on HCA to reverse course. HCA proceeded anyway. That is a full-service corporate hospital making a purely financial decision to eliminate essential community services when they stopped generating adequate volume. The same CEO who told Congress that physician-owned hospitals fail community obligations made that decision.
The emergency room argument deserves particular scrutiny. Mr. Hazen's implication is that operating an ER is a financial burden that justifies the premium reimbursement HCA collects across its outpatient system. The capital record contradicts that framing entirely. In January 2024, Hazen personally told HCA investors that the company's freestanding emergency room capacity would "grow consistently" in 2024 and 2025 to meet rising patient demand. In October 2025, HCA committed nearly $60 million to construct three new freestanding emergency rooms in Virginia alone, expanding its footprint there from eight to eleven standalone ER facilities. HCA has simultaneously been opening freestanding ERs in South Carolina, Florida, and throughout its other markets. In the first quarter of 2026, HCA reported that its emergency room capacity grew 4 percent year-over-year. A peer-reviewed analysis published in Health Affairs found that hospital emergency department revenue exceeded costs by $6.1 billion nationally as far back as 2009, a margin of 7.8 percent overall, with privately insured ED patients generating $17 billion in profit. Companies do not invest tens of millions of dollars in freestanding emergency infrastructure because that infrastructure is a burden. They expand aggressively into emergency care because it is profitable, particularly for commercially insured patients. When physician-owned hospitals choose not to operate ERs, they are not avoiding a community obligation. They are declining to compete in HCA's most profitable and most aggressively expanded service line.
The uncompensated care argument carries an equally significant contradiction. Through its Surgery Ventures division, HCA jointly owns and operates approximately 150 ambulatory surgery centers with more than 3,400 physician partners across 16 states. Those ambulatory surgery centers have no emergency rooms. They do not accept unfunded patients. They perform elective procedures on commercially insured patients and return profits to both HCA and its physician co-owners. By the precise standard Mr. Hazen applied to physician-owned hospitals before the Ways and Means Committee, his own company's Surgery Ventures facilities are doing exactly what he described as an unfair advantage. The distinction HCA is actually drawing is not between facilities that serve whole communities and those that do not. It is between facilities that HCA controls and those that it does not. When physicians own a hospital independently, HCA calls it cherry-picking. When HCA installs those same physicians as partners in ASCs under its corporate umbrella, it calls it innovative care delivery.
The history of how HCA treats physician partners outside of its direct control is documented in a Harris County, Texas courtroom. Fondren Orthopedic Ltd., a group of orthopedic surgeons, entered a limited partnership with what was then Columbia Hospital Corporation in 1993 to jointly own and operate Texas Orthopedic Hospital in Houston. The agreement ran for 57 years. For roughly two decades it functioned as written. Around 2017, HCA, which had assumed Columbia's position, began employing orthopedic surgeons at competing facilities across the Houston area, ultimately opening 10 competing hospitals offering the same services as the joint venture, in direct violation of the non-compete provisions of the partnership agreement. Simultaneously, HCA invoked those same non-compete clauses against the Fondren physicians, blocking them from doing what HCA was openly doing. In September 2024, a Harris County jury returned a verdict of $25.6 million against HCA for breach of contract. Lead attorney Joe Ahmad stated publicly that HCA owned 60 percent of Texas Orthopedic Hospital with Fondren, but 100 percent of the competing facilities it quietly opened to redirect patients away from their jointly held hospital. The jury found that HCA had the size, the scale, and the power to disregard a contractual obligation it found inconvenient, approximately 28 years into a 57-year agreement.
The legislative response is already written. H.R. 4002, the Patient Access to Higher Quality Health Care Act of 2025, introduced by Congresswoman Van Duyne and Congressman Henry Cuellar (D-TX-28), would repeal Sections 6001 of the Affordable Care Act, which banned new physician-owned hospitals from Medicare participation in 2010 and capped existing facilities at their March 2010 capacity. That ban was not derived from patient outcome data. It was a lobbying achievement. The evidence accumulated in the 15 years since passage shows that physician-led facilities consistently deliver care at lower cost with higher patient satisfaction than large corporate systems.
Thank you @RepBethVanDuyne for being a champion for patients, physicians, and communities!