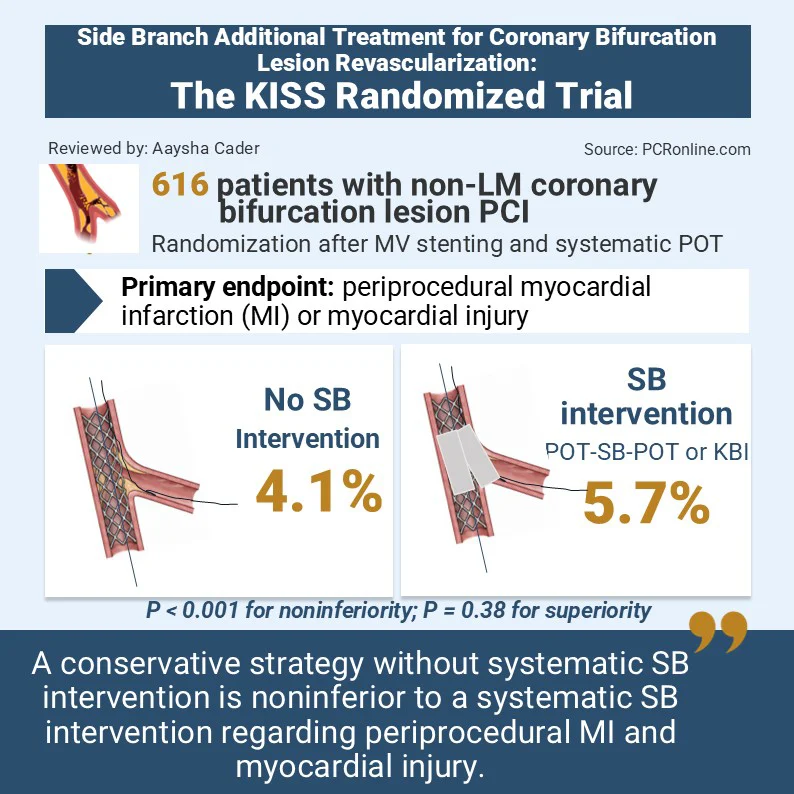
Journal Club: side branch additional treatment for coronary bifurcation lesion revascularisation: insights from the KISS 💋 randomised trial
🔗https://t.co/zHYDj2nY4E
@aayshacader reviews this trial that compares a strategy of no side branch intervention versus systematic side branch treatment in patients with non-left main coronary bifurcation lesions treated with provisional stenting and POT.
#interventionalcardiology #clinicalresearch #science
This is a 70y old lady had a syncope during Tawaf in Hajj. Transferred to the mobile cath lab in the Haram hospital in 10 minutes. Echo done immediately and revealed severe BAV and angio was normal coronary. Transferred same day to King Abdullah Medical City in Makkah. Next day got the TAVI and the day after went to Arafah to perform Hajj which was uneventful.
We are setting a new benchmark in mass gathering medicine.
The data of the mobile cath lab will be presented at the #TCTMiddleEast2026
The case was done by a brilliant young IC @MakkahCardio
Adverse Effects & short term Discontinuation of BP-Lowering Drugs 💊📊 Network Meta-Analysis RCTs: Discontinuation due to adverse effects varies by drug class. ARB-based therapies—alone or in combination—are often better tolerated 👍
https://t.co/WqzqBDRCIp
اللهم لك الحمد والمنه زراعة صمام اورطي لحاجه تركيه عن طريق القسطره بدون تدخل جراحي مما يمكنها من تكملت مناسك الحج بكل يسر...
كل الشكر موصول للفريق الذي قام بالقسطره وعلى رأسها اخي الدكتور عبداللطيف العجيمي
@MakkahCardio الذي قام بزراعة الصمام
الحمد لله رب العالمين، حمدًا يليق بجلاله وعظيم فضله، أن يسّر لي وشرّفني بقيادة مبادرة القسطرة القلبية المتنقلة في مستشفى الحرم ومستشفى شرق عرفات، لأسهم في خدمة ضيوف الرحمن من حجاج بيت الله الحرام.
ويمثل هذا المشروع مبادرة عالمية غير مسبوقة على الاطلاق، إذ تفوقنا بفضل الله على افضل التوصيات المعمول بها دوليا، إذ تُجرى القسطرة القلبية في اقرب نقطه للحشود الغفيره، مما يختصر الزمن والمسافة ويُسرّع الوصول إلى أفضل النتائج العلاجية.
وهذا يعكس حرص ولاة امرنا حفظهم الله لتقديم كل الامكانيات و افض�� الخدمات لضيوف الرحمن.
@AdelTash @Ahmed43101178 @mirvatalasnag
Just published on @ESC_Journals
Intracoronary imaging for left main percutaneous coronary intervention: a clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the European Bifurcation Club (EBC) https://t.co/Fe6iDNuwZD
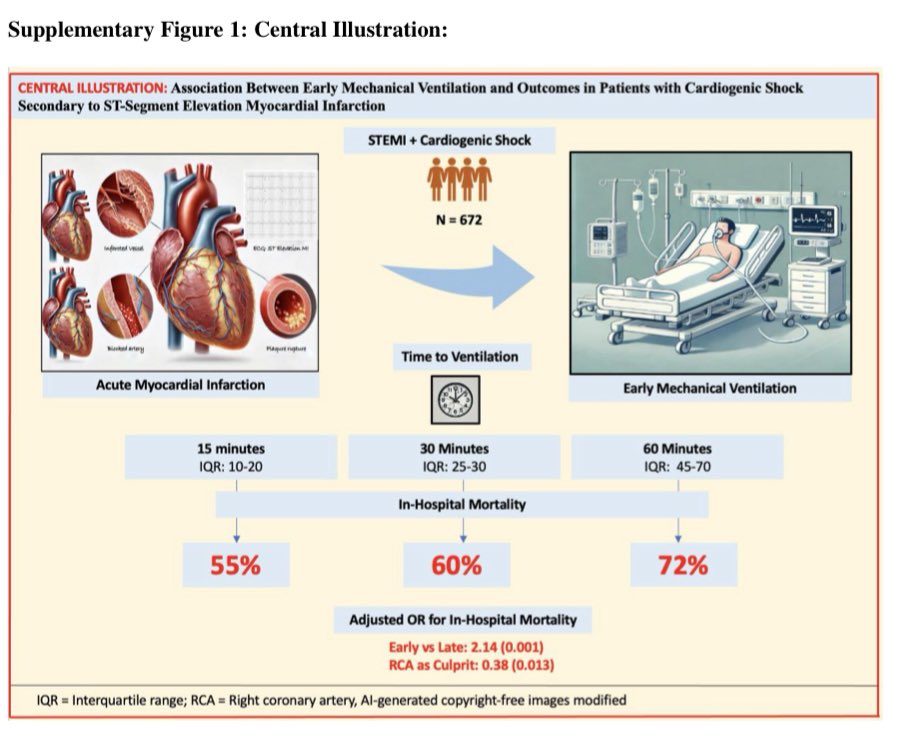
Ventricular free-wall rupture, ventricular pseudoaneurysm, and papillary muscle rupture complicating acute myocardial infarction: A clinical consensus statement of the ESC Working Group on Cardiovascular Surgery... Read more in the @EHJ at https://t.co/Aj1fXdgQsT #CardiovascularSurgery #AcuteMyocardialInfarction #CardioVascularCare @ESCardio@ESC_Journals
بعد ٤٨ عاماً من الخدمة اللامتناهية وبعد عديد من الإنجازات المشهود لها أودع مستشفى الملك فيصل التخصصي بالرياض والتي كانت منزلاً لي بعيداً عن منزلي.
" نرحل ويبقي الأثر "
Series of HCM cases:
Case 1:
https://t.co/AwUUNVxMrP
Case 2:
https://t.co/W4Ij1nZOlA
Case 3:
https://t.co/gaaopHhe4Z
Case 4:
https://t.co/8TAHL6cY3w
Case 5:
https://t.co/QK6tjUWsTD
Case 6:
https://t.co/bDz6lMwaQt
While surgeons have long been expected to perform at their peak on little sleep, new workplace standards and research trends are signaling a change in a workhorse culture that historically has made it difficult, if not impossible, for surgeons to admit when they’re too tired to operate.
Recently, the American College of Surgeons issued its first-ever proposed workplace standards for surgeons. They include a section on fatigue mitigation and recommend hospitals put formal policies in place for rescheduling or redistributing elective procedures following intense or extended duty.
Research shows fatigue can impair clinical decision-making, but whether it leads to surgical errors is less clear. “Looking at all of our available evidence, our patients do not have worse outcomes by being operated on by surgeons who were up the night before," said Jamie Coleman, MD, FACS, surgeon at UofL Health in Louisville, Kentucky. "However, that surgeon is more likely to wreck their car on the way home.”
Tap the link to learn more about the new lines of research that are exploring ways to help cognitively overloaded surgeons. https://t.co/Plq4jmRgbl
Clinical Experience With a Novel Percutaneous LV Assist Device in High-Risk PCI: Primary Results From the SUPPORT I Study: @CircIntv
🥸Does lower profile mean less vascular complications ???
😱 Summary
👇👇👇
Here is my algorithm:
1) Vasodilator therapy (if hemodynamic allow and pull)
2) Pull Rotawire. This works very effectively, 90% of times. It is frequently overlooked. The 0.014 tip works as a great way to bring back the stuck burr. Make sure wire is free with brake off for maximal efficiency. Pulling the driveshaft is less effective, as it is made of 3 coiled wires which gives some elasticity to the driveshaft.
3) If burr is free beyond lesion, can use short dynaglide runs and then pull. Prinicple is that dynamic friction is lower. Don’t overdo this and also with skipping rope technique, there is risk of driveshaft breakage and burr loss due to torsional forces with a fix s immobile burr!
4) Cut driveshaft and remove teflon sheath
5) Deliver GE over driveshaft to the burr and pull.
6) Intimal/subintimal wire and ballooning to dislodge burr and pull.
7) Re-deliver GE over driveshaft and pull.
8) Obtain second access and adding a ping-pong guide. Remember a ping-pong guide is not required in most cases. Once Teflon sheath is removed, a 6F guide can accommodate: Driveshaft + coronary wire, Driveshaft + Caravel microcatheter, Driveshaft + Corsair/Turnpike LP microcatheters, Driveshaft + 2.5-4mm balloons
9) Combine subintimal ballooning and GE over driveshaft and pull. Only these maneuvers requires ping-pong guides.
10) Call surgeons.