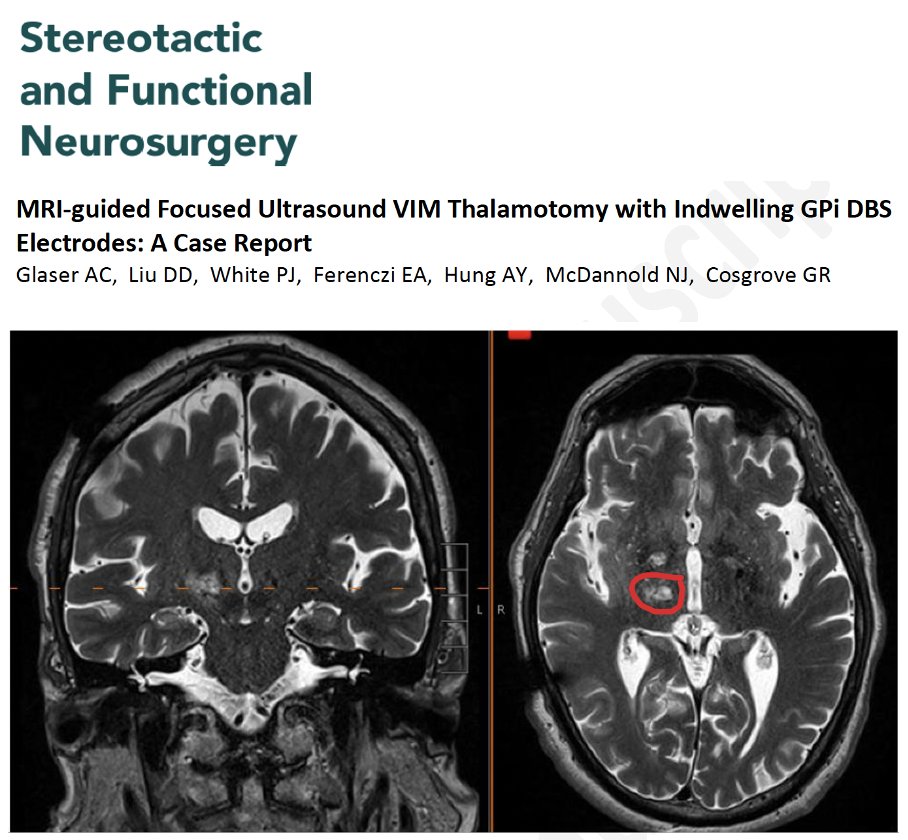
Can you 'zap' the brain with focused ultrasound if you have a DBS lead in place? A new possible twist for cases w/ both tremor and Parkinson's. For the first time, at least that I have read, focused ultrasound (FUS) thalamotomy was successfully used in a person who already had deep brain stimulation (DBS) leads implanted. Glaser, Cosgrove and colleagues open a potential path for tremor-dominant Parkinson��s disease w/ tremor recurrence despite GPi DBS. Their paper just published in the journal Stereotactic and Functional Neurosurgery.
Key Points:
- First human case I can find in a publication of MRI-guided FUS (MRgFUS) thalamotomy performed safely w/ indwelling GPi DBS leads still in place.
- They share a case of bilateral GPi DBS who developed progressive unilateral tremor unresponsive to DBS adjustments.
- The authors used 'no-pass zones' around the DBS hardware during targeting.
- The method employed the 'MRI-compatibility mode.'
- A single right-sided VIM thalamotomy via MRgFUS led to tremor improvement at 6 months following the procedure.
- The authors felt the side effects were mild and manageable (imbalance, fatigue, minor speech issues).
- They noted no hardware damage or thermal issues.
My take: If a person has a DBS lead or leads, we have, for safety reasons, not been performing focused ultrasound. If the leads are in GPi (a more lateral in the brain), the authors demonstrate it may be possible to add a focused ultrasound lesion. Here are 5 points in this work that resonated w/ me. 1- This is the first time I have read about a group combining DBS and focused ultrasound sequentially. Hopefully more groups will share experiences. 2- Tremor that returns after DBS doesn’t always mean failure. You can revise the DBS lead, add a DBS target or possibly use focused ultrasound if the lead is in the GPi target and far enough away from the FUS target. 3- Focused ultrasound, once off-limits to people with DBS, may in select cases be possible w/ careful planning. 4- Technology like this reminds us that Parkinson’s is not one size fits all disease and that there may be many innovative solutions for treatment(s). 5- Though more cases are needed, this opens a door. One important point for folks interested is the author's comment that, "FUS is not be possible with VIM or STN electrodes due to electrode overlap at the target zone." BRAVO to this team for pulling this off.
https://t.co/VXLpN2ord4 @DBSThinkTank @ParkinsonDotOrg @FixelInstitute @essentialtremor #parkinson #tremor #DBS
Today, we warmly welcome our new residents to BWH Neurosurgery! We're excited to see all the incredible things you'll accomplish during your time with us! #NeurosurgeryResidents#BWH#HMS 🧠 🤓 🥼
Thank you @CNS_Update - grateful to win best poster in neurocritical care / trauma section and thank you as always to @jh_kanterMD, Dr. Boone and such a supportive program @BWHNeurosurgery @lola_chambless
Kanter et al: The Effect of Antiseizure Medication Administration on Mortality and Early Posttraumatic Seizures in Critically Ill Older Adults with Traumatic Brain Injury
Link: https://t.co/2gBdnJU6WS
@neurocritical#NeuroCritCare
Anti-seizure medication for “patients over
65 years of age within 24 hours of admission to an #ICU after #TBI is associated with a significant
reduction of mortality…” Read more: https://t.co/EwWhYPeTp1…
Published in @NeurocritCareJ#research#neuroscience#Neurosurgery
The individual with this precuneus lesion experienced a dramatic change in how he perceived the passage of time after surgery of a glioma.
Minutes felt like hours… each time he would check his watch he’d be surprised how little time had passed. 👇
1/
I wanted to share a formative rabbit hole I went down prior to joining #NeuroTwitter. It was a project with one goal: to use neuroimaging to understand human consciousness. What ensued was fascinating. A 🧵, and you can read it in @GreenJournal here: https://t.co/AVfd6YpEuL