spends 4 years researching
women’s health apps
has thoughts
starts a Substack
Exploring what works (and what doesn’t) in period trackers, menopause apps, and digital health tools.
Evidence-based. Design-focused. Occasionally sassy.
https://t.co/9db4g69M2x
Sharing something I've been building for months. It's a data project mapping how menopause went from ignored to a policy and emergent investment in the US — told through five forces: community, capital, pharma, research, and policy: https://t.co/ocxbDm91HY
We now have a female Bryan Johnson.
It’s Kate Tolo.
She will become the most measured female in history.
+$2 million of spend per year
+ Developing a female-specific protocol
+ Sharing everything for free
To start, she will spend 3 months mapping her baseline. Men, in contrast, can get their baseline done in 1 or 2 weeks.
+ 3 months for baseline measurement
+ across 4 time points per cycle
+ doing the same thing every day
+ a dedicated full-time medical team
For context on the extensiveness of measurement, during the past 5 years, we’ve collected 1.5 billion data points on my body. I suspect Kate will exceed that given technology has improved since I started.
The goal is to create a repeatable waveform of hundreds of life-critical biomarkers. Once the baseline is acquired, she will begin interventions.
We will try to answer practically useful questions and share all of the data + learnings for free.
Can fertility be improved?
+ Should women cold plunge?
+ Can PMS symptoms be alleviated?
+ What should a female sauna protocol be?
+ Should dosage change throughout the month?
+ What keeps a cycle regular?
+ Does the body need more iron, magnesium, or protein at specific phases?
+ Should women fast?
+ Should recovery protocol change by phase?
+ What's the earliest detectable signal of perimenopause?
+ Can perimenopause be slowed?
+ How is cognitive load & mood affected?
+ Does stress impact men and women the same?
Kate has suspected endometriosis. 10% of all women do. We will try to tackle this too. I am excited for all of the surprising things we will hopefully uncover.
Unlike me, Kate does not have the innate desire to wake up at 4:30am and do six hours of longevity therapies.
She’s the cofounder of Blueprint, building in the trenches with me since day one. She understands the game and how hard it is.
In many ways, this is a sacrifice for her. She is a creative person, going from a life of freedom and spontaneity to a rigid protocol.
Traditionally, RCTs have been viewed as the gold standard. But RCTs have underserved women. The FDA banned women from clinical trials for 16 years (1977 to 1993), and most "medicine for women" is still medicine tested in men. Demanding RCT-only evidence for women's health is demanding evidence that doesn't exist. There is not enough practical scientific literature for women to reference only RCTs. It leaves half the population without a path to know what to do.
N=1 medicine is gaining ground and picking up where RCTs specifically fail. Individual science experiments give us signals that answer what to do on a day-to-day basis. This is even more important for women.
If you’re new to Kate and my world, I want you to understand that we have your back. Our intentions are to be a sturdy, reliable force in your life. To care for your best interest as we’d care for our own. We want what’s best for you and our loyalty is to your existence.
It’s pretty cool to be living in a time when we may be the first generation to not die. I’m not suggesting immortality, but lifespans so long that we stop thinking about lifespans.
At the end of the day, the one thing we each care about more than anything else is one more breath. I’m proud of Kate for taking on this responsibility. It’s painful, exhausting and costly.
The beginning of the world’s first n=2.
We now have a female Bryan Johnson.
It’s Kate Tolo.
She will become the most measured female in history.
+$2 million of spend per year
+ Developing a female-specific protocol
+ Sharing everything for free
To start, she will spend 3 months mapping her baseline. Men, in contrast, can get their baseline done in 1 or 2 weeks.
+ 3 months for baseline measurement
+ across 4 time points per cycle
+ doing the same thing every day
+ a dedicated full-time medical team
For context on the extensiveness of measurement, during the past 5 years, we’ve collected 1.5 billion data points on my body. I suspect Kate will exceed that given technology has improved since I started.
The goal is to create a repeatable waveform of hundreds of life-critical biomarkers. Once the baseline is acquired, she will begin interventions.
We will try to answer practically useful questions and share all of the data + learnings for free.
Can fertility be improved?
+ Should women cold plunge?
+ Can PMS symptoms be alleviated?
+ What should a female sauna protocol be?
+ Should dosage change throughout the month?
+ What keeps a cycle regular?
+ Does the body need more iron, magnesium, or protein at specific phases?
+ Should women fast?
+ Should recovery protocol change by phase?
+ What's the earliest detectable signal of perimenopause?
+ Can perimenopause be slowed?
+ How is cognitive load & mood affected?
+ Does stress impact men and women the same?
Kate has suspected endometriosis. 10% of all women do. We will try to tackle this too. I am excited for all of the surprising things we will hopefully uncover.
Unlike me, Kate does not have the innate desire to wake up at 4:30am and do six hours of longevity therapies.
She’s the cofounder of Blueprint, building in the trenches with me since day one. She understands the game and how hard it is.
In many ways, this is a sacrifice for her. She is a creative person, going from a life of freedom and spontaneity to a rigid protocol.
Traditionally, RCTs have been viewed as the gold standard. But RCTs have underserved women. The FDA banned women from clinical trials for 16 years (1977 to 1993), and most "medicine for women" is still medicine tested in men. Demanding RCT-only evidence for women's health is demanding evidence that doesn't exist. There is not enough practical scientific literature for women to reference only RCTs. It leaves half the population without a path to know what to do.
N=1 medicine is gaining ground and picking up where RCTs specifically fail. Individual science experiments give us signals that answer what to do on a day-to-day basis. This is even more important for women.
If you’re new to Kate and my world, I want you to understand that we have your back. Our intentions are to be a sturdy, reliable force in your life. To care for your best interest as we’d care for our own. We want what’s best for you and our loyalty is to your existence.
It’s pretty cool to be living in a time when we may be the first generation to not die. I’m not suggesting immortality, but lifespans so long that we stop thinking about lifespans.
At the end of the day, the one thing we each care about more than anything else is one more breath. I’m proud of Kate for taking on this responsibility. It’s painful, exhausting and costly.
The beginning of the world’s first n=2.
Or go to the Presidio, jump in the ocean, get a coffee at The Mill, watch sunset at Twin Peaks, ride a bike anywhere, see live music, eat a burrito, take a grass nap in GG Park, have beer at The Page, watch the Bay Bridge lights, wander Chinatown, wander Ferry building, run across GG Bridge, walk Fort Funston, eat the best meal of your life with friends…drive any direction for 2hrs. And be deeply grateful for the heavenscape you live in.
all daily life inconveniences were addressed by tech in the past decades. now all is left is the inconveniences of the mind: isolation and ego centrism.
western individualism is certainly a piece of the 'me, me, me' mentality, but another is just the natural cycle of life being a lot more comfortable today than it used to be.
when I was little, if we had to travel somewhere for a week my mom would call a friend and they'd drop us off / pick us up from the airport. We'd do the same for them. There was a lot of favor swapping because you just had to, modern conveniences weren't readily available.
now, you can survive without really interacting with a single human being in person. you don't HAVE to participate in the give-and-take, which means you throw away both the friction as well as the community and depth.
it's not just western culture anymore, even eastern cultures see this (look at the hikikomori in Japan).
@WoodyWoodys@sciencegirl Don’t care about their past is bold. Not caring actually means: Maslow pyramid of needs. Bigger fish to fry. Such a privileged perspective.
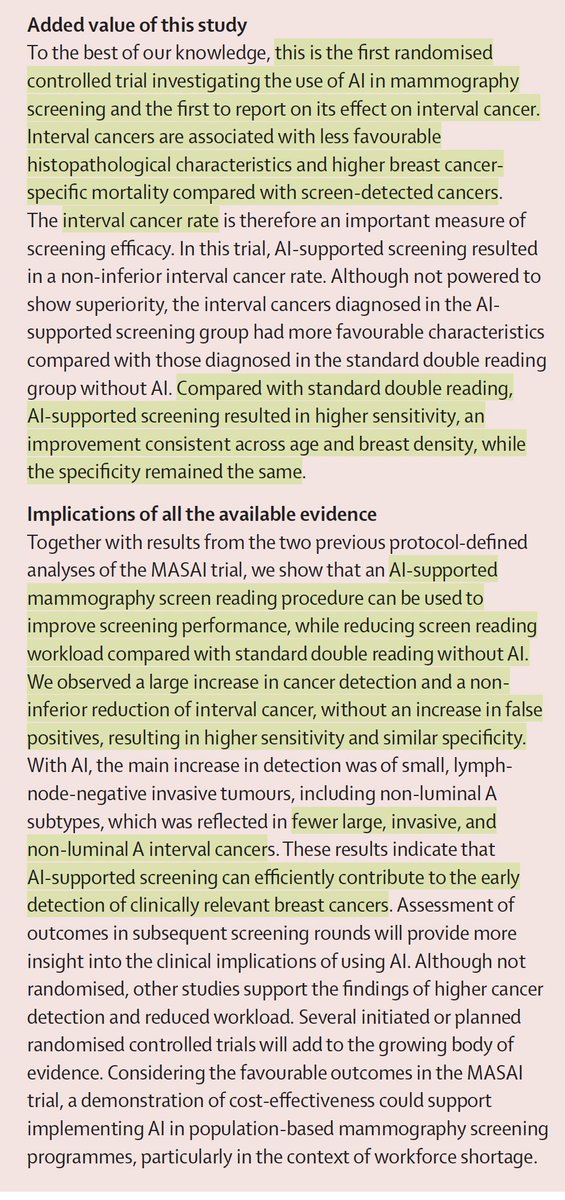
The largest randomized trial of medical A.I.
—Over 100,000 women in Sweden
—radiologist + AI vs 2 radiologists, in follow-up
—AI added led to 29% more cancer detected, 44% reduced workload, and
—Less cancer dx in subsequent 2 years, and, when found, less aggressive
https://t.co/e1hY3F0cGo
Maybe AI will finally open up space for truest UX to
emerge by taking care of pixel perfection and allowing designers to narrow in user mental models and flows
Design is the discipline of directing attention. It asks us to decide what deserves focus, what should support, and what should recede. https://t.co/JPmvrJ449Z
Finally met @joulee IRL! Loved our chat about growing design practice in places where design isn’t always the driver. A low-quality pic for a high-quality moment, thanks for sharing your wisdom!
📣 ANNOUNCING 📣
Marina Gerner @MarinaSGerner, award-winning journalist and author of The Vagina Business, will be interviewing IVG pioneer Dr. Paula Amato @PaolaAmato who was recently featured in @Nature@BBC@CNN and all leading publications around the world on the paper she published and the future of future of fertility and in vitro gametogenesis.
📆 Date: Thursday, November 20th
⏰ Time: 12:00 PM ET / 6:00 PM CET
📍 Location: Online Event
Details 👇