It's been an amazing two months learning from the best. Thank you, Dr. Daniel Van Wamelen, for letting me join your team. Thank you, Dr. Batzu and Dr. Mubs for sharing your knowledge at clinics. And thank you to the entire research team at Imark HD 🧠🧠 @KingsCollegeNHS
Most temporal lobe seizures are not localised by one symptom in OPD.
Not by déjà vu.
Not by lip smacking.
Not by one abnormal EEG line.
They are localised by watching the seizure movie in order.
Think of TLE as a subway map.
Station 1: Aura Gate
Ask: what happened first?
Rising epigastric sensation, fear, déjà vu, smell or taste aura
Think mesial temporal.
Auditory buzzing, ringing, vertigo, sound in one ear
Think lateral temporal.
Station 2: Consciousness Station
When did the patient stop responding?
Temporal seizures often build gradually and leave confusion behind.
Absence is brief.
Frontal can be abrupt and dramatic.
Tempo matters.
Station 3: Automatism Junction
The mouth says temporal.
The hands may tell the side.
Lip smacking, chewing, swallowing
Temporal network.
Manual automatisms
Often ipsilateral.
Dystonic stiff arm
Contralateral.
One OPD question can be gold:
Which hand was fumbling, and which arm became stiff?
Station 4: Lateralisation Signal Box
Dystonia, clonus, forced version
Opposite hemisphere.
Postictal nose wipe
Same side.
Aphasia or postictal dysphasia
Dominant hemisphere.
Ictal speech or vomiting
Often non-dominant, but interpret with caution.
Station 5: Temporal-Plus Trap Exit
Some seizures only look temporal.
Think insula, operculum, orbitofrontal or TPO network when there is:
throat tightness
painful aura
perioral sensory symptoms
early hypermotor behaviour
discordant MRI, EEG and semiology
failed temporal surgery
The temporal lobe may be the platform.
The train may have entered from another line.
OPD rule worth saving:
Localise TLE by the movie:
First symptom
tempo
automatisms
lateralising signs
postictal language
EEG/MRI concordance
Not one sign.
The whole seizure sequence. #Neurotwitter #Medtwitter #TLE
Neurology became irresistible once I realized diagnosis starts before the examination
Cadence of speech
Reduced arm swing
A tray neglected on one side
Apparent restlessness that is early chorea
The nervous system leaks information if you know how to observe
#Neurology#MedTwitter
The Japanese anime character Naruto Uzumaki has for generations inspired children and adults. in this study Naruto's running style was observed and described in children and interpreted as a evidence of a cultural meme rather than a pathological disorder of movement. https://t.co/bu9MnXvHp1
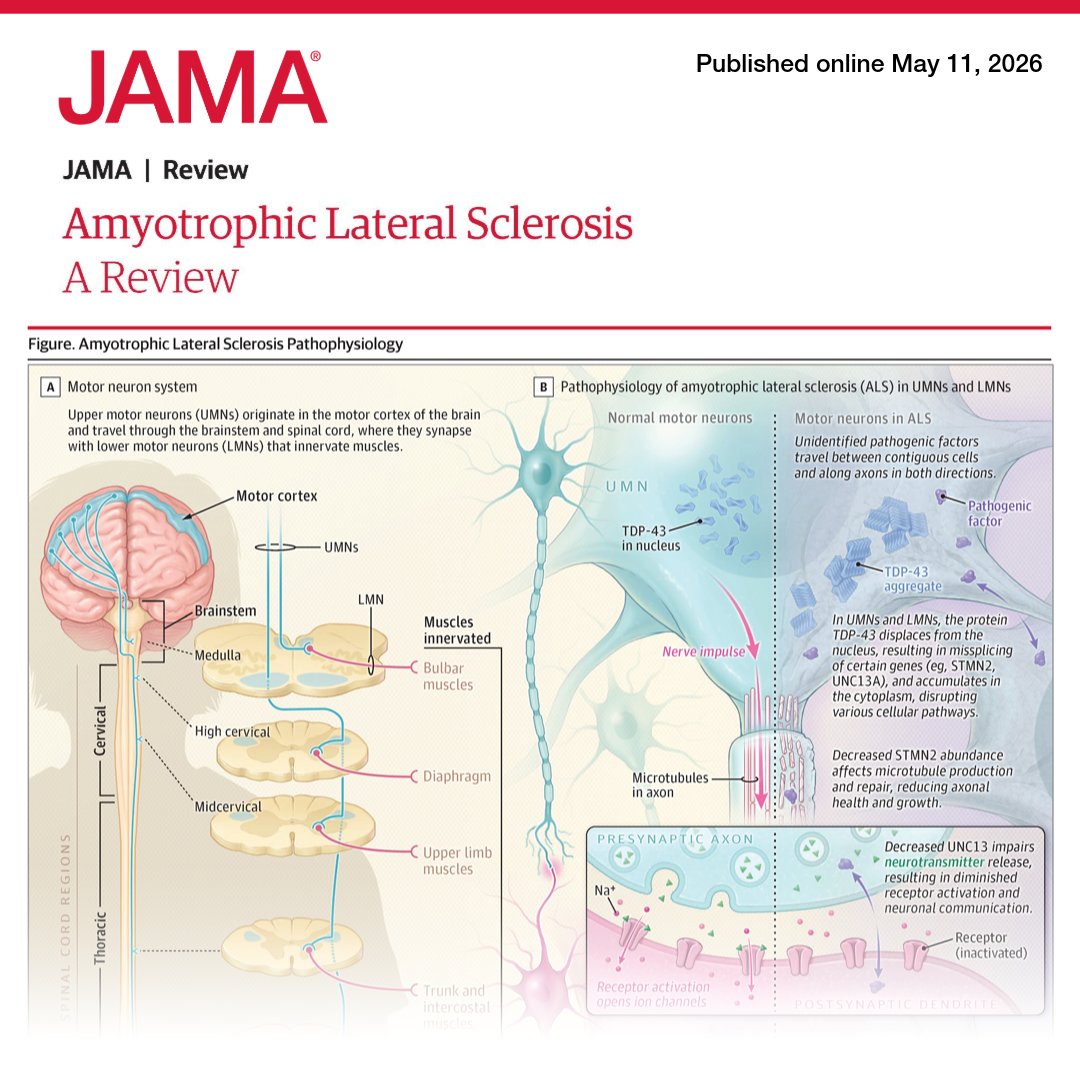
La revisión de hoy de Esclerosis Lateral Amiotrófica (ELA), una interesante y fatal enfermedad en la que hemos avanzado... casi nada. De JAMA (2026). Puntos clave:
🔴 La sospecha inicial debe enfocarse en la coexistencia progresiva e indolora de signos de motoneurona superior (espasticidad, hiperreflexia, reflejos patológicos) y motoneurona inferior (atrofia, debilidad, fasciculaciones, hiporreflexia). Primero suele ser focal, pero se disemina con el tiempo.
🔴El diagnóstico sigue siendo predominantemente clínico. La electromiografía es la herramienta de apoyo principal para demostrar denervación activa y reinervación crónica, pero sobre todo, es vital para excluir diagnósticos diferenciales (miopatías, neuropatías, miastenia). No existe ningún biomarcador diagnóstico definitivo.
🔴 Idealmente incluir paneles genéticos a todos los pacientes diagnosticados con ELA, no solo a los que tienen historia familiar. Aunque el 85% de los casos son esporádicos, identificar variantes genéticas es importante. El gen SOD1 tiene una diana terapéutica ya.
🔴 Hay +60 genes asociados a la ELA, pero el hallazgo neuropatológico en 97% es la mislocalización nuclear y la agregación citoplasmática de la proteína TDP-43
🔴 Sigue siendo fatal con una supervivencia de 3-5 años. Los fármacos orales aprobados (Riluzol y Edaravona) ofrecen un beneficio clínico apenas marginal. El manejo sintomático mediante equipos multidisciplinarios impacta más en la supervivencia. Tofersén es prometedor, una terapia antisentido intratecal que disminuye la progresión exclusivamente en el subgrupo de pacientes con mutación SOD1.
Pueden leerlo completo en el canal (https://t.co/3O93s10Td0).
From JAMA: Amyotrophic lateral sclerosis (#ALS) is an adult-onset neurodegenerative disorder characterized by progressive muscle weakness due to degeneration of upper motor neurons in the brain and lower motor neurons in the brainstem and spinal cord.
https://t.co/VvFlo5RKbX
Neuroimaging is an important tool for diagnosing genetic and sporadic ataxias. Dr. Malco Rossi breaks down his approach to imaging potential ataxia patients and what important clues and signs to look for. @AtaxiasARG https://t.co/VOxzOmv7tH
🚨 Burning Vertex Syndrome: A novel headache 🔥
A common problem in the Neurological OPD, well described by our colleague Pravin Thomas et al
🧠 Curr Opin Neurol 2025
➡️ Episodic, burning pain localized to the vertex (10–20 cm zone)
➡️ Mostly affects women (~65%), avg. age ~41
➡️ Duration: 1 min to 24 hrs, often <4 hrs
➡️ Frequency: daily to 1–3x/week
⚠️ Associated features in 76%:
•Nausea, vomiting
•Photophobia/phonophobia
•Autonomic signs
•Localized warmth (rare)
🧬Hypothesized mechanism? Small fiber scalp neuropathy
💉 Interesting finding: GON block helped in 2 patients
#NeuroTwitter #Headache
🧚♂️A previously healthy child presents with several days of fever, followed by rapid neurological deterioration and progression to severe motor impairment requiring intensive care.
🤔What diagnoses would you consider?
Clinical history
What EXACTLY happened before, during, and after the event?
-open-ended quest at begining, than close
-LOC, incotinence
-Witness and recurrence
*avoid term fainting
-Triggers (sleep dep, drugs, stand) vs premonitory symptoms
3/
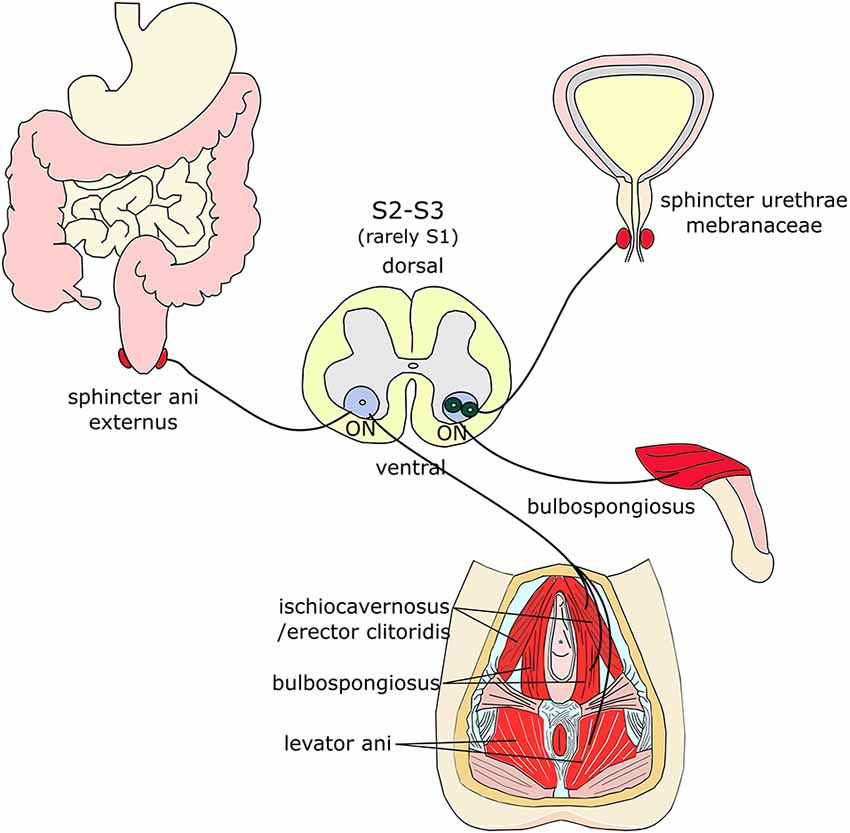
Onuf's nucleus, located in the sacral spinal cord (S2-S4), controls key muscles for urinary and fecal continence and plays a role in sexual function. Notably, it's resilient against degeneration in diseases like ALS, helping maintain continence longer. #Neuroscience#ALS #MedicalFacts
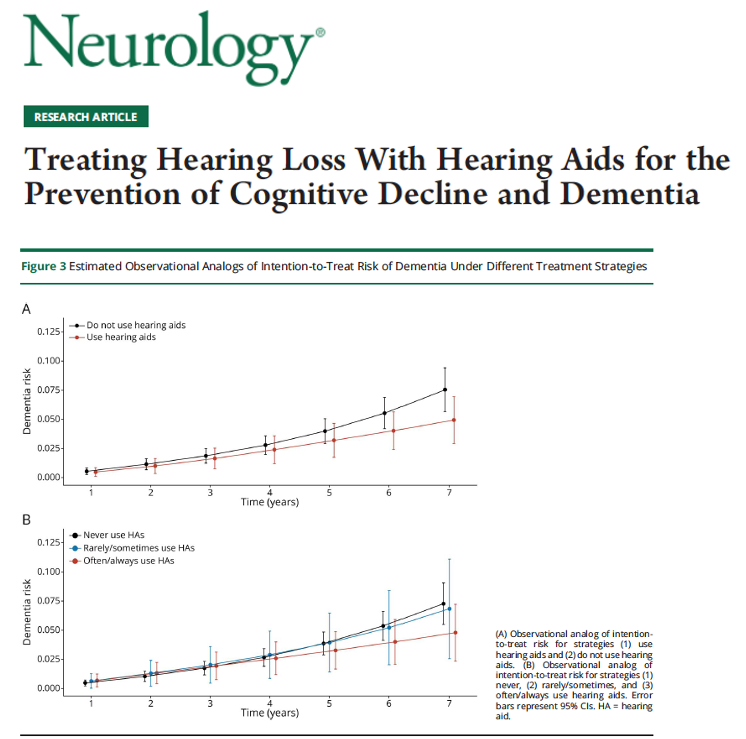
Can hearing aids help protect the brain? Evidence is coming into focus. What does dementia mean? Dementia is a group of conditions that cause progressive problems w/ memory, thinking and daily function beyond what is expected from normal aging. Cribb and colleagues describe in a new paper in Neurologyhow treating hearing loss w/ hearing aids may influence long term cognitive outcomes and dementia risk.
Key Points:
- Hearing aid use did not meaningfully change overall age related cognitive test scores over seven years.
- Hearing aid use was linked to a lower risk of developing dementia compared to not using hearing aids.
- More frequent hearing aid use was associated w/ lower risks of dementia and cognitive impairment.
My take: This study helps separate two ideas that are frequently lumped together. Hearing aids may not dramatically slow everyday cognitive aging for everyone, however they may reduce the chance of crossing the threshold into dementia, especially for some folks. That distinction matters.
Here are 5 points that resonated w/ me:
1- Hearing loss is a modifiable dementia risk factor and treating it is practical and good medicine.
2- Hearing aids may reduce dementia risk even if day to day cognitive scores look similar.
3- Frequency matters and folks who use hearing aids more consistently appear to benefit more.
4- Benefits may be greater in those w/ worse hearing or lower baseline cognition.
5- Long term randomized trials are still needed, however this evidence supports acting now rather than waiting.
https://t.co/ZCzivIPzFj @FixelInstitute@ParkinsonDotOrg@GreenJournal
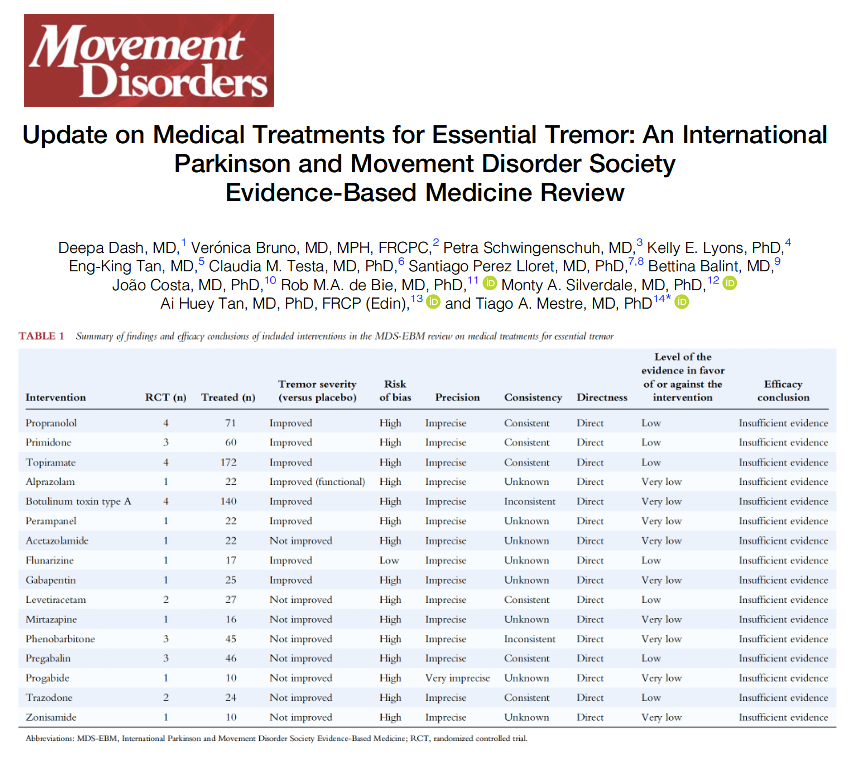
Do you know the essential tremor medication treatment updates for 2026? Spoiler alert: Medications for essential tremor are not awesome. Do treatment conversations need a reset? Essential tremor is one of the most common movement disorders and it results in action tremor that more commonly shows up when the hands are being used. Dash and colleagues describe in a new paper in Movement Disorders, an updated evidence-based review from the International Parkinson and Movement Disorder Society examining medical treatments for essential tremor. The group applied modern standards.
Key Points:
- Propranolol, primidone, topiramate and botulinum toxin showed tremor improvement in more than one trial, however the overall evidence quality was low.
- Many commonly used medications were supported by small studies w/ short follow-up and there were frequent methodological limitations.
- Using updated GRADE criteria, no available medical therapy met the threshold for confident efficacy due mostly to bias and imprecision.
My take: This is an important and sobering update. Essential tremor is common, disabling and frequently under-treated, yet our evidence base has not kept pace w/ the clinical need. Treatments do not help some folks, and we urgently need better designed, longer and more meaningful trials.
Here are 5 points that resonated w/ me:
1- Essential tremor remains a high burden condition affecting daily function and quality of life.
2- Widely used medications may help some folks, however the strength of evidence is weaker than many assume.
3- Short trials and small sample sizes continue to limit confidence in treatment recommendations.
4- Shared decision making matters and should incorporate benefits, side effects and individual goals.
5- The future of essential tremor medicines will depend on higher quality trials and innovation beyond incremental drug testing.
https://t.co/vfXtIsdjM1 @FixelInstitute@ParkinsonDotOrg #parkinson @tremorjournal@essentialtremor
we are DECADES behind on research on female health and this is what resources are being wasted on. studies about how males are collaterally affected by diseases that women suffer, studies about how men can’t get enough pleasure due to endometriosis . WHAT ARE WE DOING