Some tools to help you foster SELF-DISCIPLINE in 2025:
• BUDGET TRACKER: Follow your expenses: https://t.co/4dPiOB0kuu
• RECONSTRUCTION MODEL: Remodel your life in 90 days: https://t.co/joOpWK27bl
• MORNING RITUAL for beginners: Simple morning physical activities to keep your body moving: https://t.co/AKJySGhCLv
• MORNING RITUAL intermediate: Challenging bodyweight activities to keep your body moving: https://t.co/9ExY5JInwW
Prepare a 2025 of SELF-DISCIPLINE
#ManDay
Health was a key focus during the high-level engagement sessions, alongside breakout plenary discussions on vocational training, tourism, and the mining sector.
Additionally, a booth led by Dr. Jasdeep Bahra provided attendees with comprehensive information and live demonstrations of the department’s programs and services, emphasizing the county's commitment to accessible, quality healthcare.
Afcon final, if:
1. You have panic attacks.
2. You had a stroke in the past.
3. You had a 'partial stroke' in the past.
4. You had a heart attack in the past.
5. You have high blood pressure that is not controlled.
Please, DO NOT watch the match!
- the end -
Stop doing things for free, people don’t appreciate free things. Build your skill competently, know your worth, and put a price on it. They’ll adjust with time as long as you’re valuable.
#skill.
Correct blood pressure monitoring is essential in reducing Hypertensive-related emergencies. Here is a quick refresher on how to accurately take your readings.
Resuscitate Before You Intubate!!!
Remember, our patients in critical condition may often deteriorate following intubation. Ever wondered why? It's usually because they're not adequately resuscitated before the procedure. This tends to happen predominantly with patients needing emergency intubations, as these individuals are often in precarious hemodynamic states and might be volume depleted.
Let's dive a little deeper into the physiology. Ordinarily, our respiratory process operates under negative pressure - when the diaphragm descends, it lessens intrathoracic pressure and draws air into the lungs. Intubation switches this to a positive pressure system where air is forcibly delivered into the lungs by a ventilator. In patients with low intravascular volume, this increase in intrathoracic pressure may precipitate hemodynamic instability. This situation is further exacerbated by sedatives and paralysis, which hinder the body's ability to adapt to these sudden changes.
It's essential to note, though, that this deterioration is seldom abrupt and can often be anticipated.
Whenever possible, which is the majority of cases, always aim to resuscitate before intubation. But be aware, indiscriminate fluid administration is not the answer. A timely bedside echo can ascertain their volume status and assess their right ventricular condition - key information before intubation. Also, remember to use the Shock Index, calculated as heart rate/SBP. A value ≥ 0.9 may indicate the need for further resuscitation.
Emergency intubation, a common Pre-Hospital, ER and ICU procedure, although aimed at supporting the patient, brings about substantial changes to normal cardiopulmonary physiology. This could be detrimental for critically ill patients, unless the necessary precautions are taken during the peri-intubation period.
During positive pressure ventilation, normal cardiopulmonary interactions are disturbed due to the increase in intrathoracic pressure, leading to decreased preload and increased RV afterload.
Patients in need of emergent intubation often come with compromised hemodynamics, maintained mainly by increased sympathetic activity and elevated endogenous catecholamine levels. In addition, their illness often leads to hypovolemia due to decreased intake and increased losses. Sedatives used during rapid sequence intubation can further compromise the sympathetic response.
Failure to address hypovolemia and reduced sympathetic activity can lead to post-intubation hypotension and, in severe cases, cardiac arrest. Hence, thorough planning and preparation are more crucial than the intubation itself. Secure resuscitative access before intubation, preferably using two US-guided 18G IVs. Then, consider using point-of-care echo, especially in patients with SBP < 90 or a Shock Index > 0.9.
These patients may benefit from volume resuscitation using pressure-bagged fluids and low-dose vasopressors to raise BP. Push-dose epinephrine can be useful in situations where adequate pre-intubation resuscitation is not possible, or the sympathetic drive is so high that removing it may cause severe decompensation.
The mantra remains - "Resuscitate before you intubate."
High Quality CPR hands only, can be the difference between life and death. Take every opportunity to be up to date on your BLS and ACLS
@AARHealthcare@flexxoti
You can now take ACLS and BLS classes at our Mombasa branch located in Tononoka, along Wajir rd. Be the First to Care. Go beyond First Aid in saving lives. #TrainWithStJohn
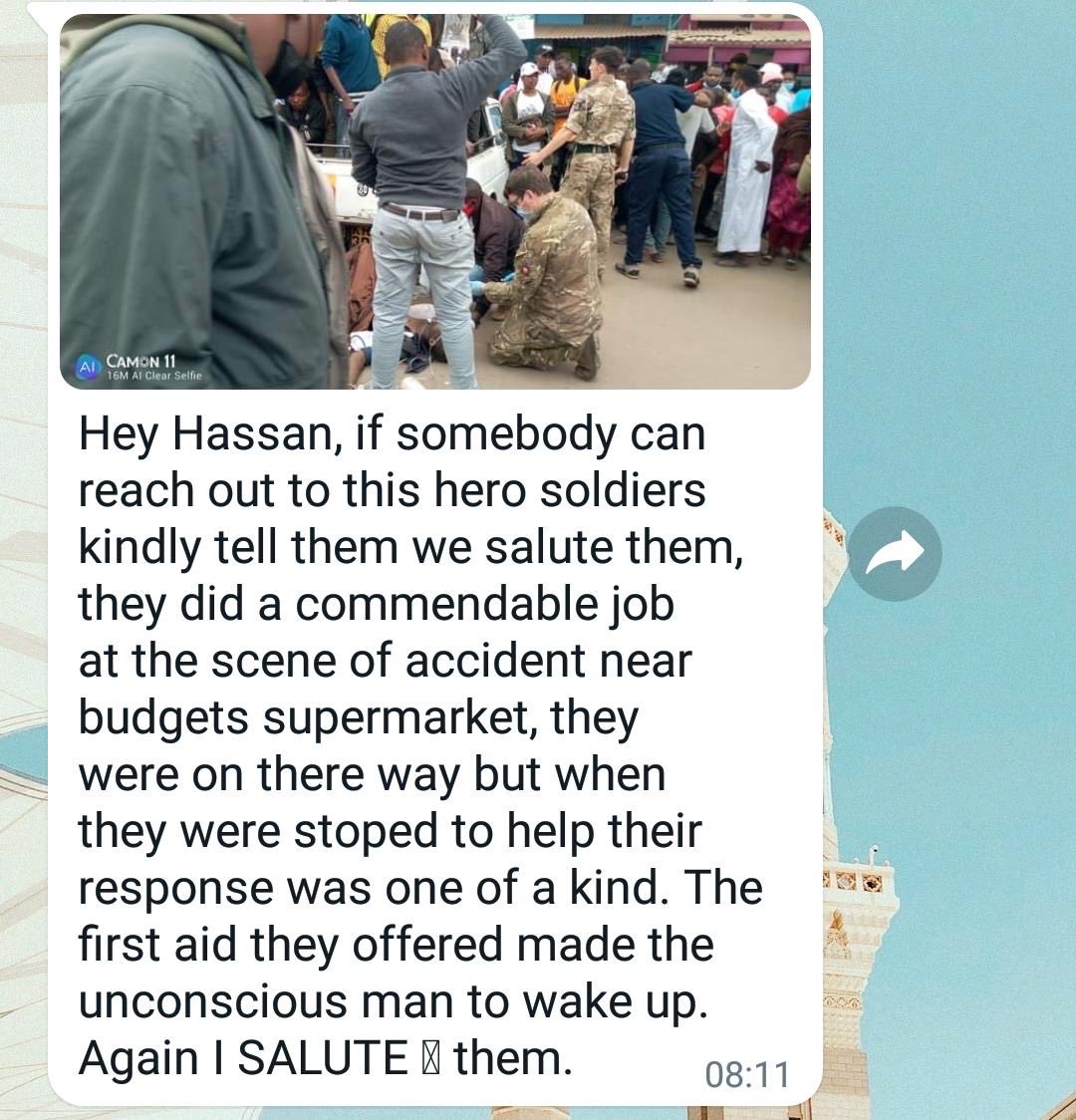
On Friday afternoon, members of the @BATUKOfficial Medical Emergency Response Team came across an accident in Nanyuki and stopped to give assistance. It isn’t technically part of their job but it is part of being a good neighbour. #community#Nanyuki#Kenya
Looks like simping in Nigeria is an economic activity.
From what I read about them on Twitter, the emasculation of men and the feminization of boys is on another level.
Men there cry on Twitter when rejected by women.
Man up!
#ManDay