One year outcomes of TAVR in young low risk patients make it into @NEJM boasting great outcomes and driving massive change in practice. @JoChikweMD and colleagues show a 220% increase in 6 year mortality for matched patients undergoing TAVR compared to SAVR. #DontDrinktheKoolAid
https://t.co/2UyDjY9tdn
My two cents: inpatient research studies/trials should consider this before using mortality as the primary endpt in trials; morbidity endpts honor the dead & living by focusing on quality of life, rather than days alive.
Building relationships is the end all be all to affect change in the workplace. Doesn’t matter how smart a person is if they can’t build trust & relationships they won’t be effective.
@propofolpapi661 We learn more when we are humble enough to admit when we don’t know or when we are wrong. It’s liberating & I wish it were more normalized. Constantly reminding my learners (& myself) of this
I light of ANNEXa-I, I am even more excited for a [possible] TEG DOAC cartridge as I think/hope it could help us personalize whichever reversal agent we use in order to achieve max hemostasis without tipping scales to the hypercoagulable side
ANNEXA-1
(nearly) direct comparison of andexanet alfa (AA) & 4FPCC
Quick 💭
🚩multiple protocol changes
🚩 AA NNH 21 for thrombotic events (driven by MI & ischemic stroke) at 30 days (replicated effect)
🙅🏼♀️No difference in mRS at 30d
It’s gonna be a no from me dawg. PCC4me.
@ralphadelta Thx for context. Difficult to choose given pages and pages of amendments. Typically excludes more patients & ⬇️ external validity. Not saying the drug doesn’t work, it
does. Inc risk of MI & isc CVA is concerning & I typically don’t view VTE ppx as effective for most MI/CVA
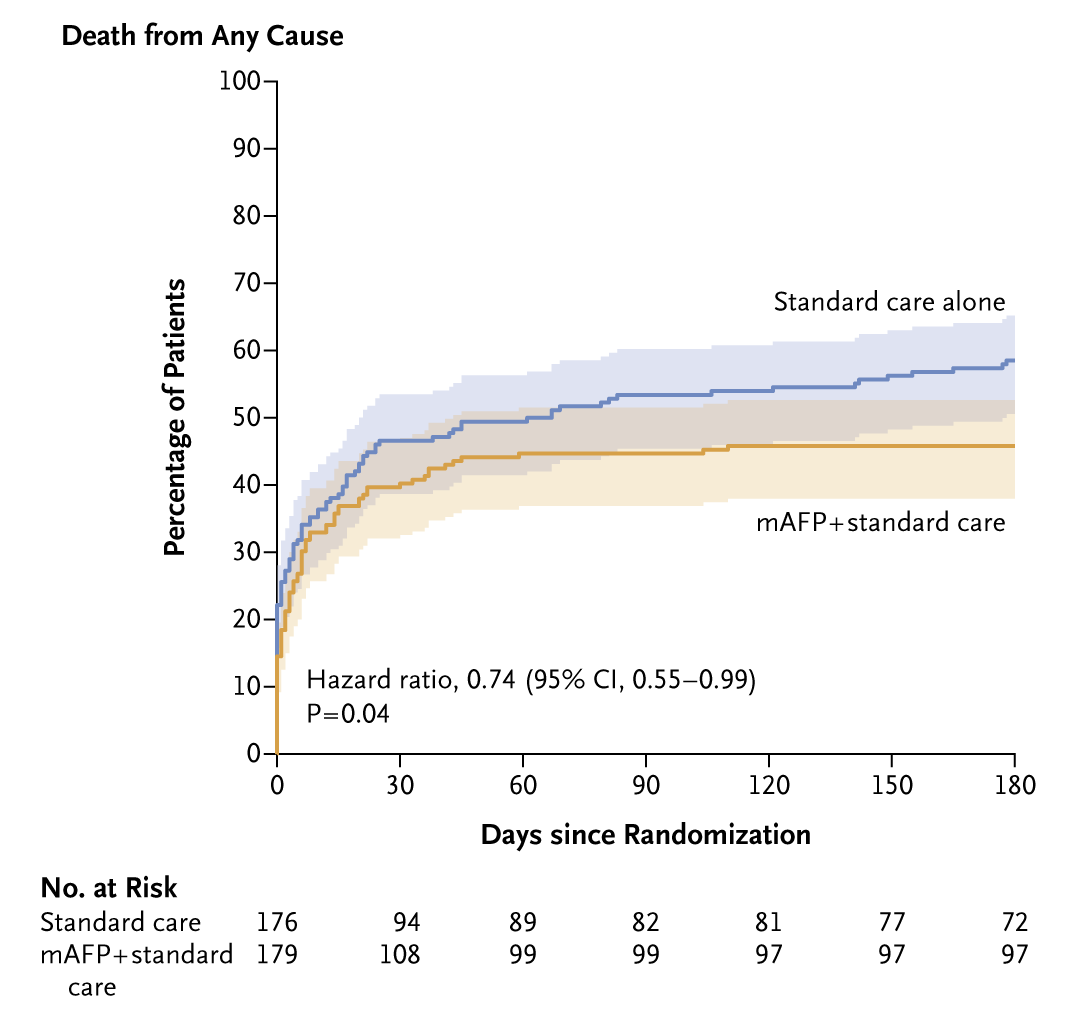
Presented today at #ACC24:
In the DanGer Shock trial involving patients with STEMI and cardiogenic shock, mortality at 6 months was lower with mechanical circulatory support with a microaxial flow pump than with standard care alone. Full trial results: https://t.co/3625asvzu8
treatment needs to focus on re-stimulation of the GABA receptors with barbiturates (phenobarbital), benzos (lorazepam), propofol...
Dexme doesn't treat the underlying problem, it just masks the adrenergic symptoms & should never be used alone as therapy for etoh withdrawal
ICU Pharmacology Secrets - Etoh withdrawal:
I heard today from a resident (when I asked if a pt had received phenobarbital): "my attending prefers Precedex (dexmedetomidine) for etoh withdrawal"
Friendly reminder: Dexme is not etiologic treatment for etoh withdrawal. The real
6/
Lessons learned:
🩸PV pts are at ⬆️ risk of bleeding events from acquired vWD and also at ⬆️ risk of thrombosis d/t high blood viscosity
🧪TEG was not able to detect vWD, however the TEG Platelet Map did show significant PLT inhibition & aided w treatment
👩🏼⚕️🧪🩸
1/
Interesting recent cardiac surgery case.
Pt w/ hx of polycythemia vera controlled on Jakafi. Other meds were ASA 81 mg & protonix daily (hx of GIB)
Baseline Global TEG normal, however the PLT map showed ~ 30% inhibition of ADP pathway.
5/
Which product(s) contains vWF?
- FFP
- cryo
Didn’t want to give FFP with shortened R time.
Cryo it was! Patient received two units & bleeding slowed.
Starting post operative aspirin today for graft patency 🤞🏻