People always love intriguing data with a plot twist (or two) in the tail and this review highlights several key angles to watch out for.
So just who's the apple of some productive researchers' eye?
https://t.co/5fByQ6TzA5
Sometimes when mired in a morass of data you have to stop and face the dragon. For companies developing ADCs, this moment may be coming sooner than many realise:
https://t.co/BTUz5bRhDZ
When it comes to new ideas, the myeloma niche is full of them w/ plenty of new regimens to explore. Some are breaking new ground, others may be left behind before they get going.
We discuss five promising ones, including an unexpected sleeper option:
https://t.co/8q4b6Wx6fD
AML progress is no illusion, neither are the traps. Where we offer some highlights and challenges in this disease – who's standing out from the crowd?
https://t.co/diy8xqziQr
Roche just paid $700M upfront for a BTK degrader this month. We're not sure the patient population it needs will still exist by the time it reaches the market.
Our #EHA26 take: https://t.co/rGZO904wcU
Keeping a beady eye on the data. Time to apply the Feuerstein-Ratain rule to a clinical readout from #ASCO26 – a specific use case with a stark reminder:
https://t.co/42HZx6wAjJ
Time for some reviews of gems from the #ASCO26 poster halls. In the first example we explore how targeting resistance in a novel and tolerable fashion may be helpful in the KRAS niche:
https://t.co/L2UNi53kwa
Our latest review from #ASCO26 explores KRAS inhibitors and why potency doesn't equal durability:
https://t.co/5HBTWpGVH2
All is not what it seems.
I still find it amazing what was one such an intractable target is now made druggable by a wide range of different inhibitors.
Beyond the hype: some reflections on half a dozen key trials presented on Day 1 at #ASCO26... what the data actually shows, where it falls short, and what comes next:
https://t.co/gCjrLDwtYp
Our final #ASCO26 Preview ahead of the meeting illustrates how an unexpected event can shoot a warning shot across competitors bows.
A great example of a cat amongst the pigeons! https://t.co/3L5SWasvN1
In the wake of the #ASCO26 data drop, we reflect on 20 key phase 3 trials which could make a significant impact. Some of these may make their competitors irrelevant if they change the standard of care:
https://t.co/EGtw35EsSk
A short, if rather provocative BSB post where we ask if naked antibodies are back in fashion – and also explore a novel bispecific ADC too! What's not to like?
https://t.co/F4wyVx7qw8
After the CAR-NK hype peaked in 2022 and several companies / products since went by the wayside, what's next in store for NK cells?
@EricVivier1 had some candid thoughts on this topic to share: https://t.co/E51hVTv2fU
Who's putting the boat out at #ASGCT26 when it comes to in vivo CAR-T cell therapies and what to watch out for.
Some surprises in store...
https://t.co/8vf35LEDpt
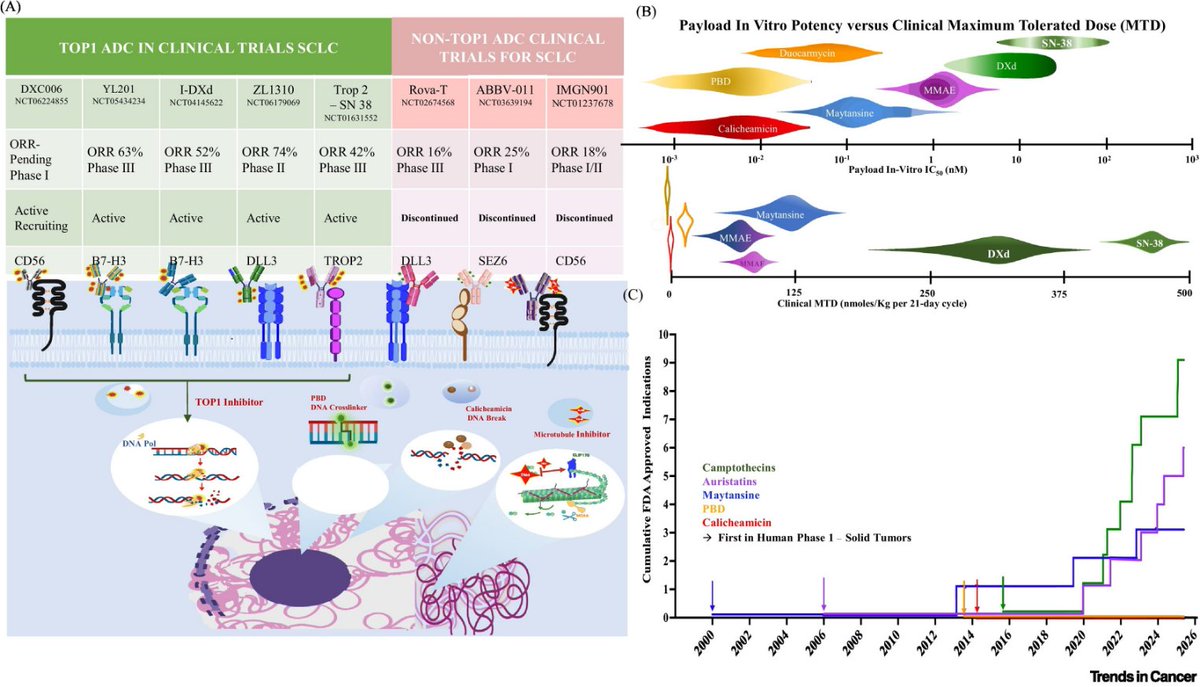
🔥Repurposing payloads: next generation of ADCs
🆙 @TrendsCancer
☑Most ADC programs on a narrow set of ultrapotent payloads
🎯Legacy cytotoxins (e.g., Deruxtecan) are being reengineered into effective ADCs
🎙Dr. Katherine Shatzer
@OncoAlert@Larvol
https://t.co/ZJpjKxpRJu
Daraxonrasib in PDAC now published in NEJM.
We have had press releases and presentations, but now a publication.
And yes, the data still look very real. 🧬
Pancreatic cancer is a RAS disease.
90% have activating RAS mutations.
G12D, G12V, G12R dominate.
And historically we have had essentially nothing direct to do about it (G12C inhibitors exist but they are a subpopulation).
Phase 1/2
Previously treated RAS-mutant PDAC
n=168
Oral RAS(ON) multi-selective inhibitor
Phase 3 dose: 300 mg daily
• ORR 35%
• mDoR 8.2 months
• mPFS 8.5 months
• mOS 13.1 months
As context; 2L chemo w/ PDAC has ORR <10% with OS ~5-7 months and significant side effects. So yes, this is huge.
Toxicity is real too:
• Any-grade TRAE 96%
• Grade ≥3 TRAE 30%
• Rash, diarrhea, nausea, mucositis, vomiting, fatigue
This is not a “write the script and see them in a month” drug.
Up-front oncoderm involvement is going to be critical. Rash needs to be anticipated, managed early, and dose modifications need to be normalized rather than viewed as failure.
BUT this is a absolute game-changer in pancreas cancer (and other KRAS driven diseases).
Importantly, this no longer exists in a phase 1/2 vacuum.
By press release, RASolute 302 met its primary and key secondary endpoints, with PFS and OS benefit versus standard chemotherapy. Full data still matter, but the confirmatory study appears to have confirmed the signal.
Terrible disease.
Great signal.
Real (but manageable) toxicity.
Practice-changing.
https://t.co/lJ8IbQydlP
@OncoAlert@TheGutOncLab@Onco_Nexus
🧬 New paper out in @Nature! We used CRISPR to selectively kill cancer cells based on a single-letter mutation in their RNA. The story I want to highlight: KRAS — one of the most notorious drivers of human cancer. A short thread on what we found 🧵
"Synergistic combinations, without disease specificity, commonly fail due to toxicity"
"Synergistic combinations should be assumed to also synergize in non-disease tissues"
Can't stress enough how this is so relevant for dual payload ADCs considering ADC disposition!!