Thank you @RepLuna and @chelliepingree for your leadership on the Paraquat Prevention Act. This bill represents an important step toward reducing environmental risk factors associated with Parkinson’s disease.
Treatment-AE in 21 (39%) after unilateral treatment; one (2%) had a persistent moderate AE at 6 months. After bilateral, 22 (55%) had AE; ten (25%) had persistent moderate or severe AE at 12 months mainly speech, gait, and balance. One developed anarthria. https://t.co/53UPDqC4Zk
Every professional organization in medicine should denounce the involvement of private equity in healthcare. They should send a clear message to their young physician members that PE is bad for hospitals, private practices, and patients.
They won’t do it, but they should.
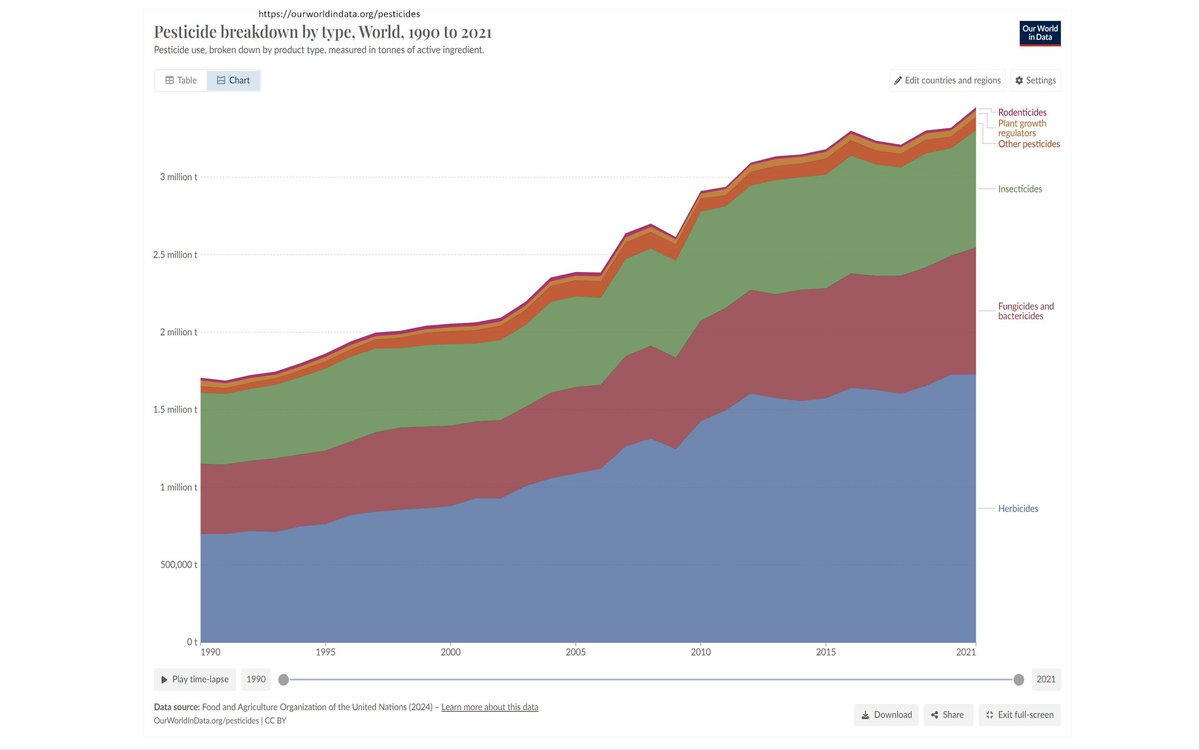
Some people believe that #pesticide use in the world has declined in the past years. I am afraid that quite the opposite is true.
https://t.co/hz2PCfr1WX
The apomorphine pump (ONAPGO) has finally been FDA approved for treatment of Parkinson's. This will be another excellent option for treating 'off medication time' in Parkinson's, and the evidence has been there for a long time. We review the key points of @TheLancetNeuro TOLEDO trial by Regina Katzenschlager, @ajlees and colleagues that was published back in 2018 and provides the solid evidence base for this therapy.
Key Points:
- In their original trial apomorphine infusion reduced medication off time compared with placebo (~2.0 hours).
- Seemed to be safe and well tolerated.
- Skin reactions and nodules have been the most talked about side effect.
- The name it will be sold under is ONAPGO.
My take: This will be a nice addition to the treatment armamentarium for Parkinson's disease folks w/ motor fluctuations. It is a wearable subcutaneous infusion device similar to what is used for diabetes. Guess what folks? There is a ~30 year history of apomorphine use in Europe. This now FDA approved subcutaneous apomorphine pump joins the new subcutaneous foslevodopa/foscarbidopa pump, as another potential choice for treatment of Parkinson's symptoms. We will need to double down on our efforts to better identify and to match appropriate folks for treatment with each pump. We will need to learn how and when to pull the trigger for the more aggressive treatments, like DBS and focused ultrasound. It will be interesting to observe whether these pumps will be a huge add for those w/ gastric dysmotility and variable absorption of medication; and of course how well tolerated they will be in the real-world. Finally, how necessary will a good care-partner be to ensure success of a pump; I suspect this will be critical. I believe that we will – docendo discimus – learn by teaching, sharing and of course publishing our experience.
https://t.co/qm7NSUr9Ir
Press release on approval:
https://t.co/T04VdwjhzC #Parkinsons
The randomized trial results are in for the GLP-1 drug Exenatide for Parkinson's disease. Spoiler: NO symptomatic or disease modifying effect. Tom @foltynie@DavidStandaert and I interviewed in the @nytimes@ginakolata on the latest paper just published in @TheLancet by Tom and his colleagues.
Key Points:
- 'Rigorous' study randomly assigned Parkinson’s folks to take exenatide (a relative of Ozempic).
- 194 folks enrolled in the UK.
- "No benefit or slowing of the course of Parkinson's after 96 weeks."
- "No effect on patient symptoms, no effect on brain scans, no subgroup that showed any benefit. No matter how the researchers sliced the data the results were the same."
My take: “This is a sobering moment. This is a really well done study, and it came up empty-handed.” Animal studies and small human studies previously suggested benefit. Another recent smaller study of a similar drug, lixisenatide, in the @NEJM was positive. “Researchers started digging into claims databases...and asked if patients who had taken GLP-1s might be less likely to get Parkinson’s or, if they had it, would have a disease that progressed more slowly...the results were promising." "They looked at epidemiological studies. They found that people with diabetes who took GLP-1s were less likely to have Parkinson’s." When the first study came out Gina quoted me as saying we were “nibbling at the edges of disease modification.” We were however all humbled and this reminds us how important it is to do the science, and not to rush to market or judgement. Dave commented that “he wouldn’t do another study like this unless you learn what is the target...what is the biochemistry you are trying to change in the brain? How do these drugs work, anyway?” Good science means replication. Good science protects the public and in the case of GLP-1s, there can be associated weight loss and loss of muscle mass, and that is something we probably want to avoid in Parkinson's. Ab uno disce omnes – from this one example we learn (all the rest). Let's stay humble, but keep learning and advancing the science for the benefit of those w/ Parkinson's and beyond.
https://t.co/7N3xmGkqwH
NYTimes article:
https://t.co/FvVMm3spo7 #Parkinsons #GLP1 #ozempic #diabetes
Do you know the pathophysiology underpinning the stiff-person syndrome? Can you make the correct diagnosis by undertaking the right examination and supporting laboratory tests? Marinos Dalakas writes a delightful and complete article in @Nature Reviews Neurology.
Key Points:
- Stiff person is the most common form of glutamic acid decarboxylase (GAD) antibody spectrum disorder.
- It is autoimmune.
- On exam look for stiffness, muscle spasms and task-specific phobias.
- GAD antibody titers are essential for diagnosis.
- If GAD titers are low in blood, it may require spinal fluid.
- Stiffness and task-specific phobias are underpinned by 'impaired reciprocal GABAergic inhibition, reductions in brain levels of GABA, and cortical hyperexcitability.'
- Common treatments include GABA-enhancing antispasmodic drugs, 'baclofen, gabapentin and diazepam.'
- Some cases get IVIG or rituximab.
My take: This is an outstanding review article, however remember than many clinicians have made the mistake of 'jumping' to a stiff person syndrome diagnosis, without walking through proper diagnostic steps. In Aspen, the experts discussed how the rate of misdiagnosis is high so let's all read the article and make sure we get it right! Finem respice – consider the outcome, if you rush and make the wrong diagnosis.
https://t.co/pjaApNZm1t #stiffpersonsyndrome #GADantibody #autoimmune
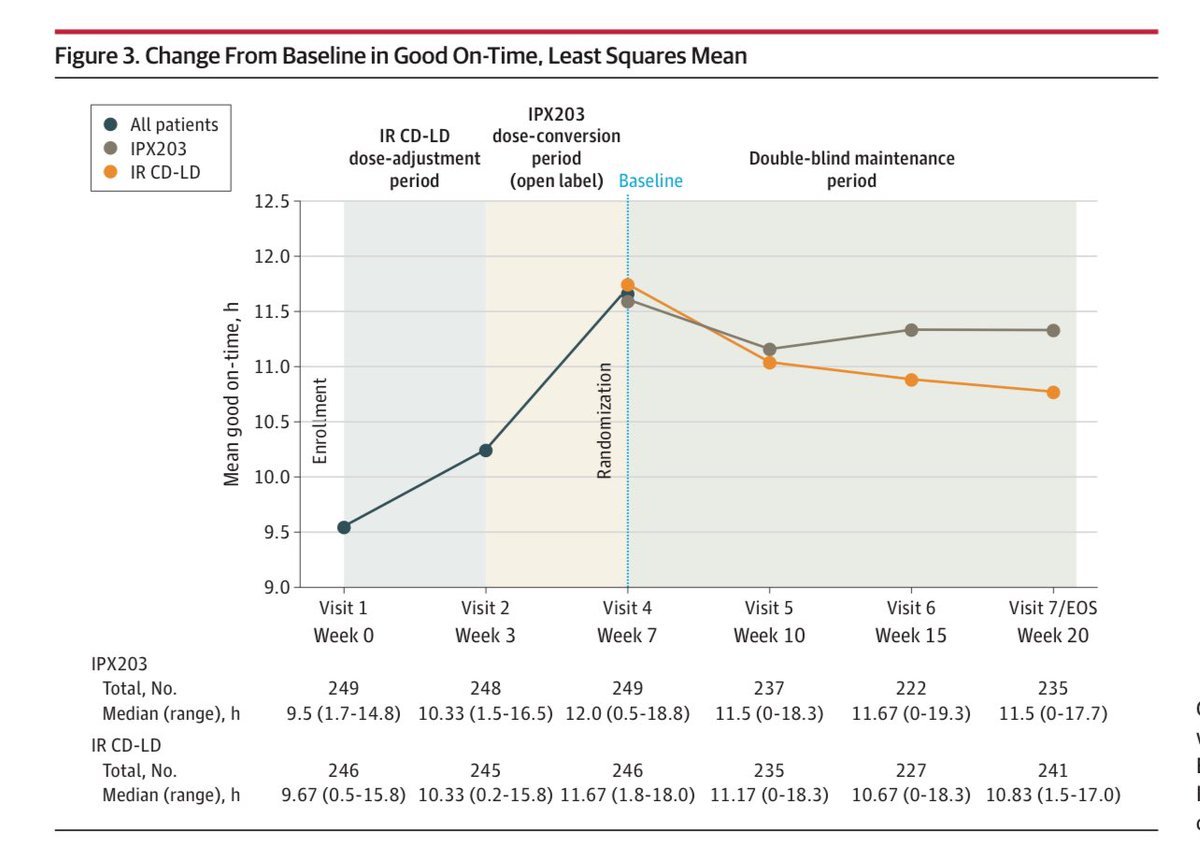
Do you have a plan of when to pull the trigger on new FDA approved drugs for Parkinson? What did the data show on the newly FDA approved drug for Parkinson in the publication in @JAMANeuro by Hauser and colleagues.
Key Points:
- IPX203 was tested against immediate release levodopa for treatment of motor fluctuations.
- Called in the RISE-PD trial.
- It was a randomized trial.
- The drug tested was an extended-release carbidopa levodopa.
- 506 folks in the study.
- The key change was improvement in daily good on-time compared to immediate-release carbidopa-levodopa ‘when dosed a mean of 3 times per day compared to 5 times per day for immediate-release carbidopa-levodopa.’
My take: It is always great to see another drug approved for use in Parkinson. How do you know when to use a new formulation? There is no right answer. The way I approach it in my clinic is simple. I tend to not change formulations of carbidopa levodopa if folks are doing well. If there is wearing off and a desire to not move doses of PD medications closer, I check to see the cost for the person w/Parkinson for any new drug whatever and whichever one it is. I like to give persons choices and partake in active shared decision making. If for example the cost is thousands of dollars a year, and we can achieve a similar outcome changing intervals with regular release levodopa, we may recommend that option; for some folks that is rent for the month or a mortgage payment; the stakes of the discussion can have serious ramifications for a family unit. We tailor the therapy and use what fits the whole person and their complete situation. The data from this new study on this new drug showed 1.55 hours of additional on time per day. Dialogue is the key to success.
https://t.co/QNAyDIHG2I #parkinson #dopamine
Improved Sleep Correlates with Improved Quality of Life and Motor Symptoms with Foslevodopa/Foscarbidopa @KRayChaudhuri1@BrunoBergmans https://t.co/YlKVs2rTOC
What were the results of the randomized clinical trial of Fecal Microbiota Transplantation for Parkinson's? It was safe, but not effective as just published by Filip Scheperjans in @JAMANeuro and colleagues.
Key Points:
- The authors were interested in whether fecal microbiota transplantation was safe and may improve symptoms of Parkinson's?
- They recruited 45 folks.
- There were only transient gastrointestinal adverse events.
- There were no clinically meaningful improvements.
- Though transplant induced stronger, donor dependent, microbiota changes, 'dysbiosis resolved more frequently after placebo.'
My take: Folks have been asking us this question recently about the microbiome and the excitement of getting a fecal transplant. It is a 'hot' topic. This study reminds us that it is complex and there are a lot of unknowns. @jbeck_PhD@ParkinsonDotOrg nailed it when he said, "the key question that needs to be solved is how to best perform these transplants. One issue is that you cannot plant grass when the yard is full of weeds. However, if you take too hard an approach killing the weeds — that is, with powerful antibiotics — you jeopardize the new grass, or in this case, the bacteria in the transplant. Solving that issue will be important as we consider whether this is effective or not." It is really interesting that we commonly find dysbiosis among Parkinson's folks, and we are learning more and more about the gut-brain connections. However, whether modified approaches or bowel cleansing will change the outcome, only time will tell. We continue to search for mens sana in corpore sanō – a sound mind in a sound Parkinson's body. https://t.co/hZivy8ffBV #Parkinsons #microbiome #fecaltransplant
Restless Legs Syndrome (RLS) always draws questions on iron and iron therapy. So how about everything you need to know in a single slide? Ok, maybe not everything, but a lot! #RLS#restlesslegssyndrome
Anticholinergics can worsen facial dyskinesia in tardive syndromes and guess what Professor @DrSusanHFox reminds us that anticholinergics are probably not such a hot idea to treat tardive syndromes. This is an historical approach and probably needs to be 'sun-setted.'
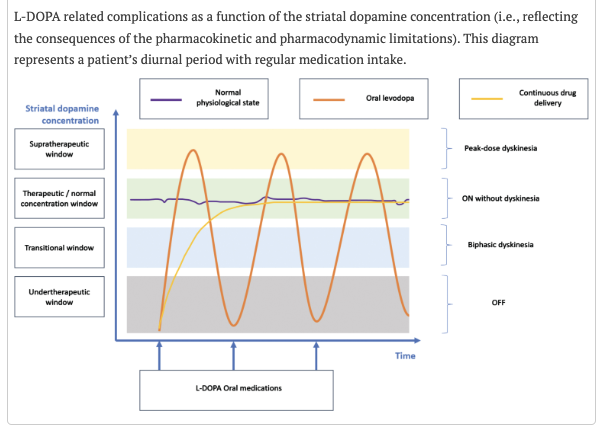
How effective are continuous dopaminergic therapies in Parkinson’s? Can you name 6 limitations in current therapy? The shortcoming seems to be at least in part linked to the L-DOPA pharmacokinetics and pharmacodynamics as well as disease progression. Demailly, Moreau and Devos highlight the key parts of this story in their new paper in @journal_PD.
Kep Points:
- The authors remind us that dopamine cannot cross the digestive and blood-brain barriers.
- It is therefore the precursor drug levodopa that we use to get the drug to the brain.
- There is a complex interplay of Parkinson's disease progression which is coupled with the pharmacokinetic and pharmacodynamic properties of L-DOPA which render it tricky to deliver; and perhaps why we must make changes in dose and timing of dose over time for any given person.
- Many authors and experts have opined that motor and non-motor complications could be better addressed by 'continuous dopaminergic delivery therapies.'
- The authors identified 6 key limitations of levodopa including "1- restricted digestive and cerebral absorption; 2- unnecessary peripheral distribution; 3- short half-life; 4- age- and PD-induced decline of central aromatic L-amino acid decarboxylase; 5- misdistribution in many cells; and 6-pulsatile stimulation of dopaminergic receptors."
My view: The authors hit the nail on the head when they 'honestly' share with us that the pharmacokinetic and pharmacodynamic 'constraints' have not been adequately addressed by current Parkinson's therapies. There have been many attempts at continuous dopaminergic stimulation, and we must now ask ourselves; is it the methods that will require refinement or do we need to pivot to a different or more nuanced approach? Either way, clinicians hopefully will appreciate that the 'timing of medications' remains a critical factor in the long-term management of Parkinson's disease. Summum bonum – the highest good dictates that we care for the people today, while we 'continue' to ponder the mystery of the optimal dopamine delivery system of tomorrow. https://t.co/lmcuY5HpFO #parkinson
This our moment to raise awareness and protect our children. Corey Booker’s dad had Parkinson’s and now he is sponsoring a bill to ban paraquat and other pesticides. This is not a blue or red issue; It is a shared community challenge. #pdenviron conference @RayDorseyNeuro
Rest in peace to the term, extrapyramidal system. @AbhiLenka11 and @JankovicJoseph put the final nail in the coffin in their new piece in @GreenJournal Neurology Clinical Practice.
Key Points:
- Johann Prus coined the term extrapyramidal in 1898.
- He experimented on dogs and thought there must be dual motor control outside the pyramidal tracts.
- He established 'beyond doubt that in the case of transection of the pyramidal tracts the pathways by means of which transmission of cortical epilepsy is effected must lie outside the pyramidal tracts and outside the so-called pontine tracts.'
- Other like Kinnier Wilson applied acronym 'EPS.'
- The authors argue the term has a lack of clinical, anatomical, and physiologic definition.
- They argue that 'contrary to traditional assumptions, pyramidal and extrapyramidal systems are not mutually exclusive.'
- They poke holes in the reasons why we use EPS to describe drug induced movement disorders.
My take: RIP EPS. You have reached your expiration date, and we retire you to the neurological descriptor 'hall of fame.' Thank you for your service, as we will now use 'specific phenomenologic descriptors to illustrate to colleagues and readers the broad spectrum of hypokinetic and hyperkinetic movement disorders.
https://t.co/RbyuNRr6Zh #Extrapyramidal #basalganglia #neurology #neurologicalexamination
@MichaelOkun@MDJ_Journal I don't think every idea needs to be tried in real world. It's unlikely be comfortable to wear for 16 hours. What happens when patient needs to eat or drink? How will excess saliva impacts this?
Aspen Neuroscience @AspenNeuro announces that the first participant has been dosed in their Phase 1/2a open label ASPIRO trial, assessing safety & tolerability of ANPD001, an autologous, dopaminergic neuron cell replacement therapy for #Parkinsons
https://t.co/GklKq6iraz