#WashUMed Neurology represented at #AANEMinSanFran this year!
Michael Petrany, MD, PhD, and Carolina Parra Cantu, MD (@caropact), both presented posters.
Kierkegaard said the function of prayer is not to influence God, but rather to change the nature of the one who prays, and the same is true of hope, dreams, so many things. The fruits are internal
We are excited to report the discovery of TIGRs, a widely-occurring RNA-guided system found in bacteria and their viruses. TIGRs consist of a peculiar repeat region which is transcribed into RNA and processed into multiple guide RNAs to direct TIGR-associated proteins to their DNA targets. https://t.co/ketXqFVQqw
The diagnostic criteria of CIDP is not simple.
Trying to make it easier, our @MayoClinicNeuro PN group lead by @grace_swart , Mike Skolka and Chris Klein created the CIDP calculator. It’s open access and If the probability of CIDP is >= 92% the sensitivity and specificity for CIDP is 100% and 93%, respectively, after exclusion of the most common mimics.
https://t.co/emThZiCk5o
Insular Ribbon Sign on CT:
A subtle but crucial early sign of MCA infarction. Loss of the normal gray-white differentiation in the insular cortex due to cytotoxic edema (left side). Right side for comparison, bright normal insular cortex.
Always check the “insular ribbon” in acute stroke!
— my reporting list
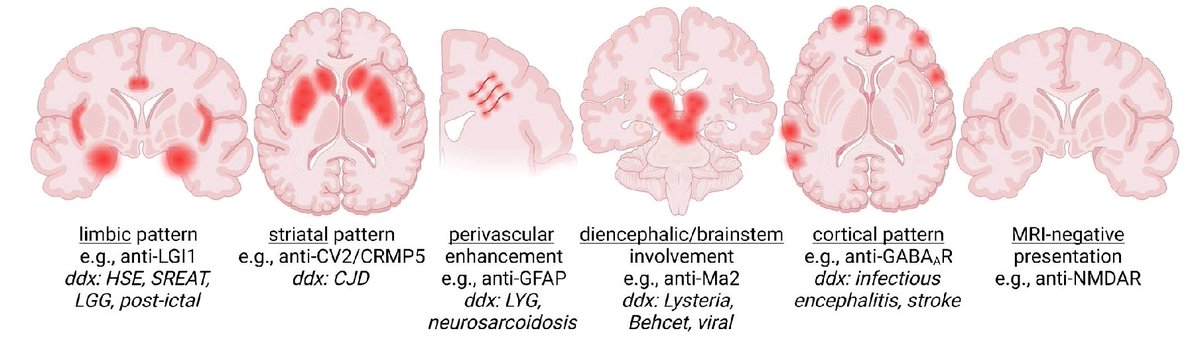
This is PSP, right? Neurodegenerative and progressive, right? Wrong. This is autoimmune encephalitis associated with autoantibodies directed against the GABAB receptor. Great teaching case presented by Mustafa, Garg and colleagues @MDCP_Journal
Key Points:
- Progressive recurrent backward falls for 3 months.
- Slowness w/ unclear speech, body stiffness and a poker face.
- Abnormal walking for one month (ataxic).
- Vertical upgaze palsy w/ preserved vestibulo-ocular reflexes.
My take: The clue was the subacute onset of atypical parkinsonism w/ a PSP-like phenotype accompanied by gait ataxia. Mark Hallett always says in Aspen, think about autoimmune ataxia when there is a subacute presentation. Be aware that the anti-GABAB receptor-mediated encephalitis can be observed in "drug refractory epilepsy, anterograde amnesia, limbic encephalitis and rapidly progressive dementia." Only half of cases will end up being associated with a hidden cancer. Docendo discimus – we learn by teaching – and we should be aware that PSP-like phenotypes can rarely be associated with autoimmune disorders.
https://t.co/FtuouD83dd #PSP @ParkinsonDotOrg@FixelInstitute
Here's an excellent review of NMO spectrum of disorders .https://t.co/SxUbtXXMYL. Brilliant illustration of differences in CNS involvement in NMO MS and Anti MOG disease.
#neurotip#Neurology
When I have a new fellow or resident in our peripheral nerve clinic, I always teach them the importance of defining the neuropathy clinical syndrome. NCS/EMG are valuable, but the neurological exam is the most important (as it should be in neurology but many have forgotten).
This is the neuropathy clinical phenotype classification I find the most helpful:
- Isolated small fiber neuropathy
- Length-dependent peripheral neuropathy (or distal symmetric polyneuropathy)
- Multiple mononeuropathies
- Mononeuropathy
- Asymmetric neuropathy
- Polyradiculoneuropathy
- Plexopathy (brachial or lumbosacral, many times a radiculoplexus neuropathy)
- Sensory neuronopathy
- Motor neuronopathy
I always tell my trainees they don’t have to memorize the causes of each phenotype. If you define the syndrome correctly, you can ask Google or ChatGtp what are the most likely causes. 😊
Definitions 👇👇👇
#NeuropathyBites
1/x
My most significant contribution to ALS Research until today.
We used F-waves and AI to estimate the likelihood of ALS and their survival risks @WashUNeurology@MayoClinicNeuro.
https://t.co/ePPLymVdW9
Diagnosing PML relies heavily on CSF JC virus PCR. Our study finds excellent PPV of PCR performed at our national testing site, and highlights suggestive neuroimaging findings that can facilitate PML diagnosis. Illustrative images of these findings below:
https://t.co/KGEg75mALc
Will you recognize myoclonus dystonia or will you miss it? Peng, Lei and Hei in the @GreenJournal refresh us on this important hyperkinetic presentation.
Key Points:
- Myoclonus is the fastest movement disorder.
- The authors remind us to look for brief, lightning-like involuntary movements.
- In this case the neck is triggered by handwriting.
- There was also a sustained hand twisting during writing that we refer to as a dystonic writer's cramp.
My take: Surprisingly, this diagnosis is missed more than it should be. Many people obtain the genetics and look for the epsilon-sarcoglycan (SGCE) gene variants (DYT-11). It turns out however, that myoclonus dystonia cases frequently turn up negative for SGCE and have other causes (only ~30-40% may be positive for this SGCE gene). Interestingly, in the classic cases only ~5% who inherit the gene from their mother turn up w/ symptoms. Always ask about alcohol responsiveness (in adults) and associated psychiatric symptoms. When you see myoclonus dystonia, it can be tricky to pin down the causes. Think about DYT-1 genetic dystonia, dopa-responsive dystonia due to the GTP-CH gene, vitamin E deficiency, mitochondrial diseases and beyond.
https://t.co/BJDzXexJ6J #dystonia