Really amazing critique of a terribly flawed paper. What were the editors thinking? Just say no to stuff like this. Or... publish the paper and then another paper explaining the flaws--like below. The flaw-explainer offers 10x the value
In an era of new energies & catheters, we went back to the ECG.
The notch in OT PVCs isn’t just morphology, its timing grounded in a mechanistic framework predicts the site of origin. Full data now out in @JElectrocardiol@HappyEP@YigitYilanci@umutinevi https://t.co/vsrPSjOmt2
🔱Documento de consenso ESC @escardio 2026 sobre las Complicaciones Mecánicas del IAM. 🫀💥
🟥Rotura de pared libre ventricular, pseudoaneurisma ventricular y rotura del músculo papilar. Aunque hoy ocurren en <1% de los IAM gracias a la reperfusión temprana, siguen siendo complicaciones devastadoras, con mortalidad intrahospitalaria de 30–40%. ⚠️📈☠️
🔺️Rotura de pared libre ventricular (RPLV): suele aparecer entre las primeras 24–48 h, aunque clásicamente se describía a los 5–7 días post-IAM. Puede manifestarse con dolor torácico, disnea, choque cardiogénico, taponamiento o paro cardíaco. Factores de riesgo: presentación tardía, IAM extenso, sexo femenino, edad avanzada e hipertensión.
🔺️Pseudoaneurisma ventricular
Es una ruptura contenida por pericardio o trombo, con alto riesgo de ruptura franca. Su incidencia actual es 0.1–0.3%. Suele localizarse en pared inferior o posterolateral y puede debutar semanas o meses después del IAM. El riesgo de ruptura espontánea puede alcanzar 30–45%. Datos clásicos: cuello estrecho (relación cuello/fondo <0.5) y flujo turbulento Doppler. El riesgo de ruptura espontánea puede alcanzar 30–45%.
📜🆓️⤵️
https://t.co/rMc1LU3xqn
https://t.co/jU8OGv1XW0
🔍 #EHRATopicWeek on Atrial Tachycardias
Atrial Tachycardia is more complex than we once thought
Traditionally, rapid regular atrial arrhythmias were divided into “atrial tachycardia” and “atrial flutter” based mainly on ECG appearance. Today, high-resolution mapping shows these distinctions are often oversimplified.
📌 Current concepts classify all regular atrial rhythms >100 bpm as AT:
• Non-reentrant AT
• Reentrant AT (localized or macro-reentrant)
Importantly, many arrhythmias previously labeled as “flutter” may actually represent different AT mechanisms.
⚡ Differentiating AT from organized AF can be challenging, especially in scarred atria or after ablation. ECGs, EP studies, intracardiac mapping, and even wearable devices all play an important role in diagnosis.
💡 Precise classification matters — for diagnosis, treatment strategy, and improving ablation outcomes.
Find out more in the #EHRA_ESC Consensus document on Management of patients with atrial tachycardia 🔗https://t.co/T5EGaHI51q
@escardio@EuropaceEiC
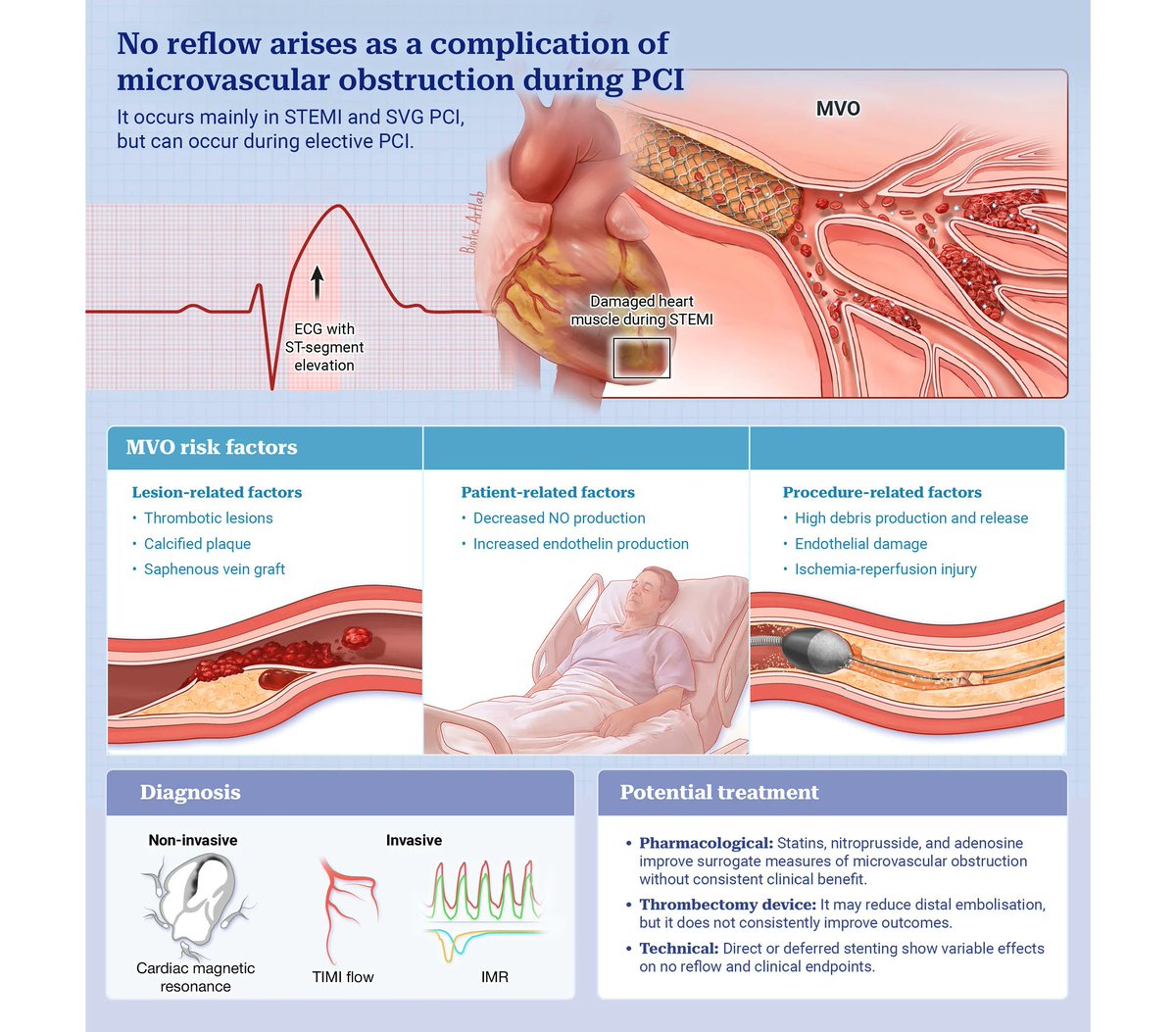
Despite successful primary PCI in STEMI, impaired myocardial reperfusion (“no-reflow”) may occur due to microvascular obstruction.
This state-of-the-art review provides a comprehensive overview of the underlying pathophysiological mechanisms, as well as invasive and non-invasive diagnostic tools, and pharmacological and interventional treatment strategies, highlighting current gaps in the field.
🔗https://t.co/UaXeekKr5i
#STEMI #InterventionalCardiology #NoReflow #cardiotwitter
@sbrugaletta@Ortega_Paz@josepgomezlara@LaudaniClaudio
Activation patterns and electrophysiological characteristics of Marshall Bundle related left atrial tachycardias post atrial fibrillation ablation
https://t.co/OqxoMbv4dj
This state-of-the-art review provides a comprehensive overview of the pathophysiological mechanisms underlying the no-reflow/slow-flow phenomenon, covering invasive and non-invasive diagnostic tools, pharmacological and interventional treatment strategies, and the key clinical gaps that still need to be addressed in the field. https://t.co/glYW3u2X2z
New @NEJM
For persistent atrial fibrillation, first-line pulsed field ablation (PFA) superior to medical therapy (AAD) in a randomized trial for preventing recurrent atrial arrhythmias @omwazni
https://t.co/VN4t1OwYON
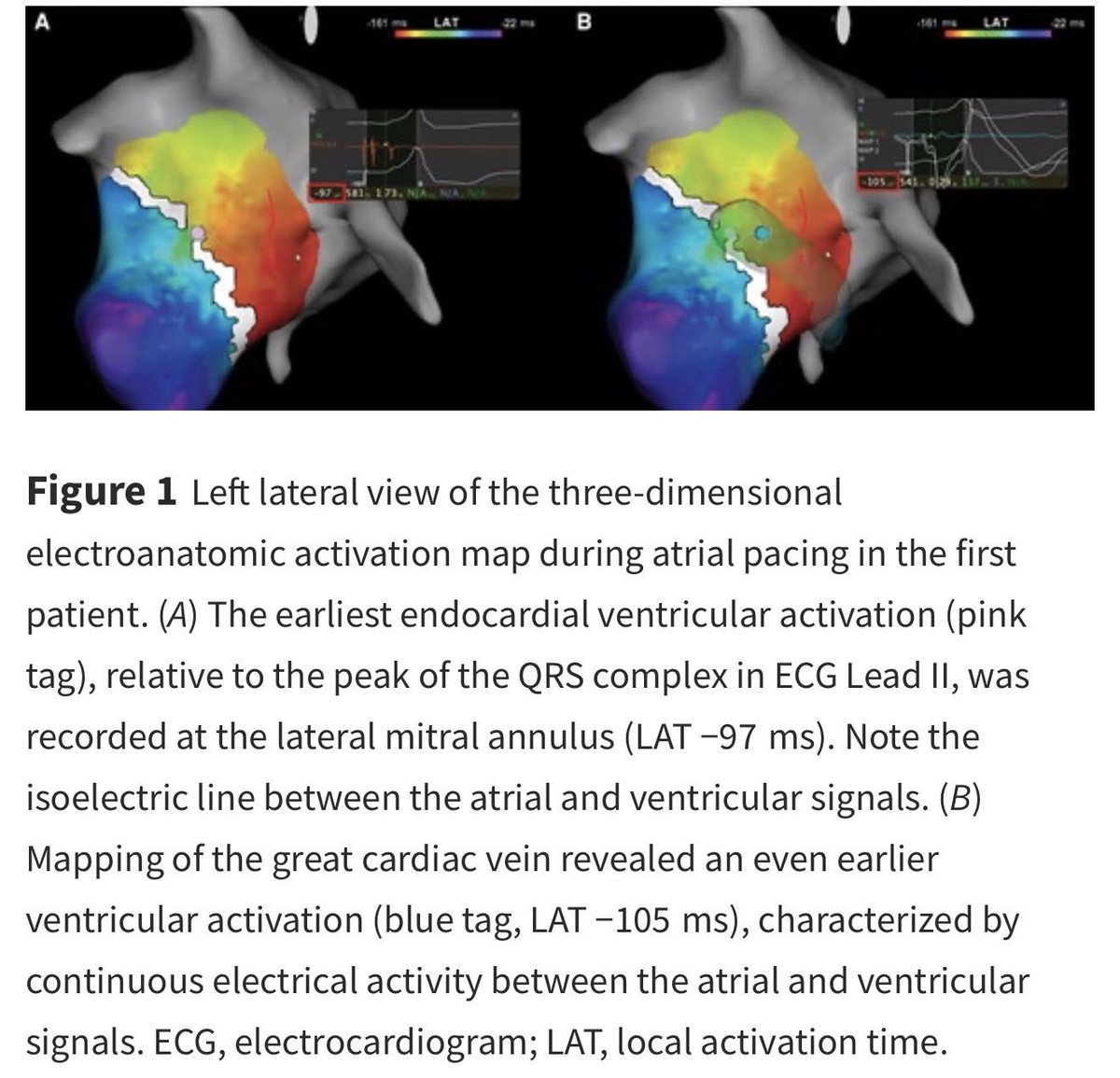
Precise Localization of the Ventricular Insertion of a Bystander Concealed Nodoventricular Pathway in Fast–Slow Atrioventricular Nodal Reentrant Tachycardia #OpenAccess@Koichi16423232
https://t.co/eeCqZmxTbY