Just published my new article “Computational Modeling Of @PalisadeBio's PALI-2108 Tissue Penetration In Fibrostenotic Crohn's Disease” (free link in comments). $PALI
I spent weeks building a computational reaction-diffusion model in Python to simulate whether PALI-2108 can penetrate strictures in FSCD deeply enough to intercept fibrosis. Looking forward to your feedback!
The $ABVX situation this week was a valuable lesson and a fantastic opportunity to learn about my (investment) behaviour under stress.
Yes, I held my shares through the panic, but I didn’t add when Mr. Market handed me such a unique opportunity. I never doubted the potential of obefazimod, yet I wouldn’t be honest if I claimed the uncertainty that surfaced this Tuesday didn’t affect me at all. I must always stay humble and never stop being a student of the markets.
Therapy-refractory IBD is anything but abstract to me. I see these patients regularly when surgery, frequently with a life-impairing ostomy, is the last option left. Still, I passed on this chance to increase my position in what could become a true game-changer for these patients because of a “signal” that might just turn out to be noise in the long run.
The $ABVX situation this week was a valuable lesson and a fantastic opportunity to learn about my (investment) behaviour under stress.
Yes, I held my shares through the panic, but I didn’t add when Mr. Market handed me such a unique opportunity. I never doubted the potential of obefazimod, yet I wouldn’t be honest if I claimed the uncertainty that surfaced this Tuesday didn’t affect me at all. I must always stay humble and never stop being a student of the markets.
Therapy-refractory IBD is anything but abstract to me. I see these patients regularly when surgery, frequently with a life-impairing ostomy, is the last option left. Still, I passed on this chance to increase my position in what could become a true game-changer for these patients because of a “signal” that might just turn out to be noise in the long run.
Preclinical data published in a peer-reviewed manuscript in Science Advances, published by @aaas, demonstrated robust T cell activation, durable immune memory, and a lymph node-targeted mechanism that supports next-generation immunotherapies. https://t.co/3Ftgb91aEi $ELTX
Today, we are pleased to announce that the U.S. FDA has granted Fast Track designation (FTD) for VS-7375, an investigational oral KRAS G12D (ON/OFF) inhibitor for the treatment of KRAS G12D-mutated locally advanced or metastatic non-small cell lung cancer (NSCLC).
FDA’s FTD program helps to advance the development and review of new drugs that are intended to treat serious or life-threatening conditions and that demonstrate the potential to address unmet medical needs.
The FDA previously granted FTD to VS-7375 for the treatment of KRAS G12D-mutated locally advanced or metastatic pancreatic cancer, underscoring the urgent need for new treatment options for patients with KRAS G12D-mutated cancers, including NSCLC and pancreatic cancer.
Read the press release: https://t.co/fsxQjH57Vm
Learn more about VS-7375 on our web site: https://t.co/vrgNBVHOh8
#NSCLC #KRAS #KRASG12D $VSTM
In retrospect, it’s almost sweet.
French biotech $ABVX just wanted to show everyone the cool maintenance results they got and did not expect biotech to be the shark tank it is.
How can this happen with a multi-billion-dollar company? Never underestimate how crucial the right management is, even with an asset like obefazimod.
Always be a student of the market. You never stop learning.
To my best knowledge there’s no biologic evidence for $ABVX's obefazimod *causing* cancer, and even if it could facilitate malignant transformation, which I highly doubt given the MoA, you wouldn’t see it at 44 weeks. Solid tumors like breast or prostate cancer grow over years, not months, so based on what we know about tumor kinetics these were most likely already present (and occult) at baseline.
Besides this, you’d expect colorectal cancer for epithelial tumors in a UC cohort, since these patients already carry elevated CRC risk. Instead it’s one (anecdotal) prostate cancer and one breast cancer case, the most common background cancers with age, and no CRC (the one colonic finding was dysplasia, exactly what UC surveillance is built to catch). That’s the fingerprint of incidental age-related disease.
Statistics speak the same language: two invasive non-skin cancers, both at 50mg and none on placebo (p≈0.50); 3 vs 0 if you fold in the colonic dysplasia (p≈0.25); and 4 vs 1 for skin cancers (p≈0.37). With so few events, two of them landing in one arm is roughly a one-in-three coincidence, not a signal of drug-driven carcinogenesis.
Across the broader program the picture holds: over 1,000 patients and volunteers dosed historically, hundreds of patient-years at 50mg, a consistently favorable safety and tolerability profile, and no clustering of malignancies.
What remains is a best-in-class efficacy profile in UC. Thanks to @A_May_MD for this fantastic pick!
@RevMedicines Thank you for your fantastic work from the bottom of my heart! The kind of breakthrough you delivered is precisely why I invest in biotech and why I believe that capitalism and freedom are the very basis for the innovation that ultimately serves all of humanity.
Nevertheless, even in the best case, some suspicion of a cancer link will probably stick to $ABVX's obefazimod. That's the cruel thing about biotech investing: nobody can predict how it plays out, and there will always be risks you do not see coming.
To my best knowledge there’s no biologic evidence for $ABVX's obefazimod *causing* cancer, and even if it could facilitate malignant transformation, which I highly doubt given the MoA, you wouldn’t see it at 44 weeks. Solid tumors like breast or prostate cancer grow over years, not months, so based on what we know about tumor kinetics these were most likely already present (and occult) at baseline.
Besides this, you’d expect colorectal cancer for epithelial tumors in a UC cohort, since these patients already carry elevated CRC risk. Instead it’s one (anecdotal) prostate cancer and one breast cancer case, the most common background cancers with age, and no CRC (the one colonic finding was dysplasia, exactly what UC surveillance is built to catch). That’s the fingerprint of incidental age-related disease.
Statistics speak the same language: two invasive non-skin cancers, both at 50mg and none on placebo (p≈0.50); 3 vs 0 if you fold in the colonic dysplasia (p≈0.25); and 4 vs 1 for skin cancers (p≈0.37). With so few events, two of them landing in one arm is roughly a one-in-three coincidence, not a signal of drug-driven carcinogenesis.
Across the broader program the picture holds: over 1,000 patients and volunteers dosed historically, hundreds of patient-years at 50mg, a consistently favorable safety and tolerability profile, and no clustering of malignancies.
What remains is a best-in-class efficacy profile in UC. Thanks to @A_May_MD for this fantastic pick!
For transparency: I am long $ABVX and may add to or trim my position at any time. This is my own view and analysis of publicly available trial data only. Not financial or investment advice. Do your own due diligence.
To my best knowledge there’s no biologic evidence for $ABVX's obefazimod *causing* cancer, and even if it could facilitate malignant transformation, which I highly doubt given the MoA, you wouldn’t see it at 44 weeks. Solid tumors like breast or prostate cancer grow over years, not months, so based on what we know about tumor kinetics these were most likely already present (and occult) at baseline.
Besides this, you’d expect colorectal cancer for epithelial tumors in a UC cohort, since these patients already carry elevated CRC risk. Instead it’s one (anecdotal) prostate cancer and one breast cancer case, the most common background cancers with age, and no CRC (the one colonic finding was dysplasia, exactly what UC surveillance is built to catch). That’s the fingerprint of incidental age-related disease.
Statistics speak the same language: two invasive non-skin cancers, both at 50mg and none on placebo (p≈0.50); 3 vs 0 if you fold in the colonic dysplasia (p≈0.25); and 4 vs 1 for skin cancers (p≈0.37). With so few events, two of them landing in one arm is roughly a one-in-three coincidence, not a signal of drug-driven carcinogenesis.
Across the broader program the picture holds: over 1,000 patients and volunteers dosed historically, hundreds of patient-years at 50mg, a consistently favorable safety and tolerability profile, and no clustering of malignancies.
What remains is a best-in-class efficacy profile in UC. Thanks to @A_May_MD for this fantastic pick!
$tenx Want to address some bear points regarding tenx in one place.
1. bear point: 6mwd is an unreliable endpoint and even if levosimendan works in pH-HFpEF there is a high risk the 6mwd is to noisy/sensitive to outliers/other factors. 1/11
Sorry, I might have to fix this title:
“Phase 3 Readout Of Daraxonrasib In 2L Metastatic PDAC Marks **THE** Inflection Point For Pancreatic Cancer”
$RVMD
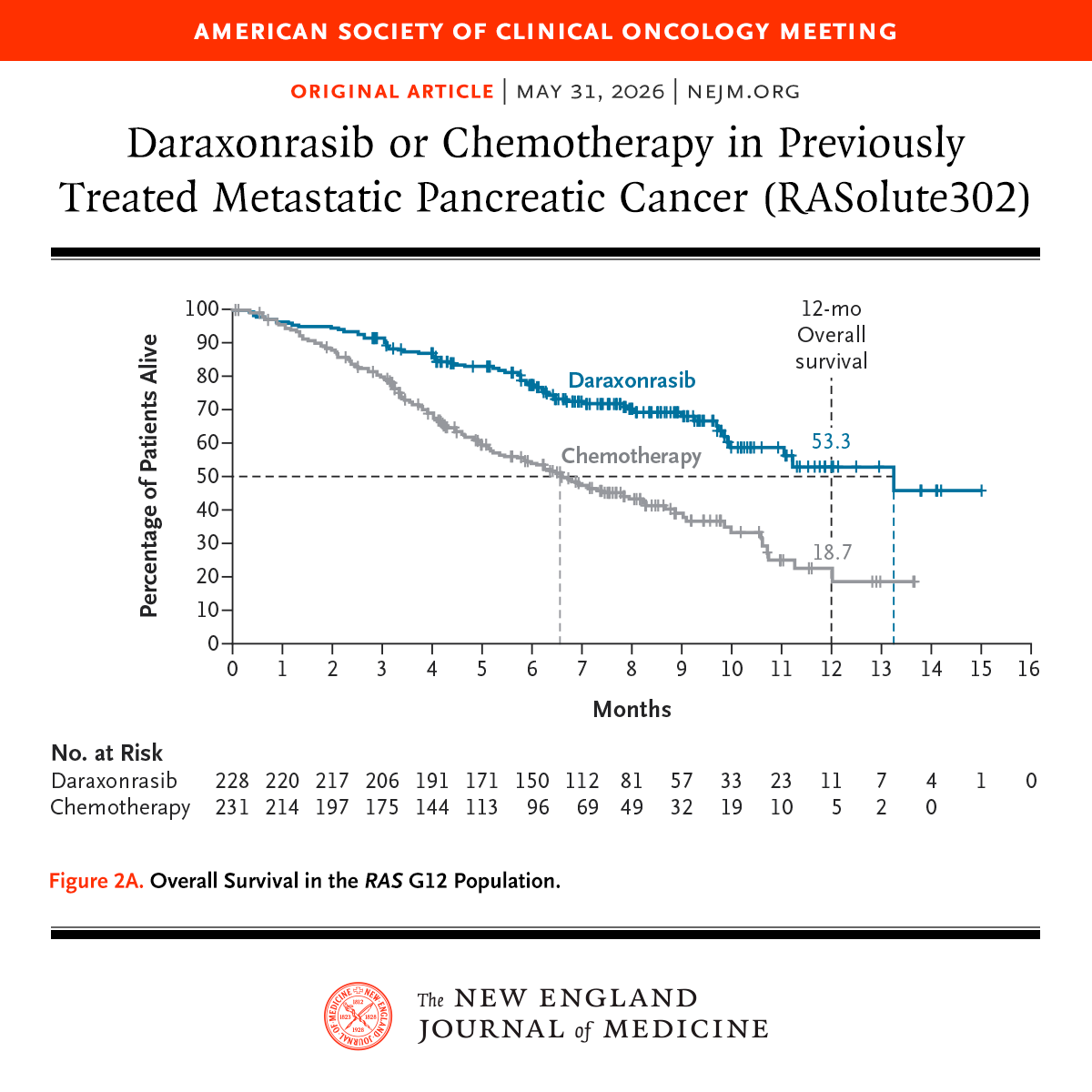
Just published my new article “Phase 3 Readout Of Daraxonrasib In 2L Metastatic PDAC Marks An Inflection Point For Pancreatic Cancer” (free link in comments). $RVMD $ERAS
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
I am not sure if you really know what you are talking about. It’s Group 2 PH, not ‘Type II PAH.’ Levosimendan acts mainly by reducing venous congestion and preload, not through the arterial pulmonary dilation. LEVEL’s primary endpoint is 6-minute walk distance, not wedge pressure, so your point on Phase 3 hemodynamics misses what the trial is judged on.