En sistemas sanitarios fuertes (Alemania, Países Bajos, Suiza, Dinamarca) el médico tiene un rol clínico diferenciado y protegido, con condiciones laborales y retributivas que lo mantienen dentro del sistema público. España acaba de aprobar lo contrario.
Un estatuto que consolida la precariedad médica y borra la identidad profesional de los médicos va a acelerar la fuga hacia el extranjero que ya estamos viviendo. Y ese daño no se reparará fácilmente. Pero lo más grave no son las condiciones laborales de los médicos, sino un cambio deliberado de modelo sanitario, aprobado mientras el ciudadano mira a otra parte, con una negociación diseñada para excluir a los propios médicos de la mesa del ámbito. Lo que está en juego no es un convenio colectivo. Es la calidad de la atención que recibirás. Es la seguridad cuando enfermemos. Es la confianza en un sistema que todos hemos construido durante décadas.
Eso merece, como mínimo, que lo sepas.
¡SOMOS DE PRIMERA FEDERACIÓN!
Ha sido un camino duro, lleno de esfuerzo, trabajo y momentos difíciles… pero nunca dejamos de creer
Ni el equipo, ni el club, ni una afición que ha estado siempre ahí
Este logro es de todos
Gracias por no rendiros nunca, por empujar cuando más lo necesitábamos
Esto es por vosotros 💜
Seguimos haciendo historia
#RealjaénCF #VolverASentir
Prasugrel, Ticagrelor, or Clopidogrel After Percutaneous Coronary Intervention
🔊 prasugrel provided the optimal balance between efficacy and safety compared with ticagrelor and clopidogrel
https://t.co/3ZakzJjICi
INCLISIRAN
✍️Fast-track lipid-lowering treatment early after an acute coronary syndrome
🌏Real-World-Data on ACS patients
⬇️LDL: 147->30 mg/dl
👍🏻50% achieved goals at 15d
👍🏻100% achieved goals at 30 d
https://t.co/vZg76U1abD
Diuretic resistance is not a therapeutic dead end → it’s a signal that we need a smarter strategy.”
The perfect closing slide from Dr. Ana Belen Mendez Fernandez at #HeartFailure26 👏
5-step framework for smarter decongestion:
1️⃣ Recognize the problem
Multifactorial, common, predictable — requires a structured approach
2️⃣ Objective assessment
Weight, ultrasound, BNP, renal function, volume status, urine output
3️⃣ Optimize loop diuretics
Adequate dose & frequency, IV route, check absorption
4️⃣ Sequential nephron blockade
Target different nephron segments, overcome compensatory mechanisms
5️⃣ Treat the drivers
Venous congestion, low cardiac output, neurohormonal activation
And the line that should be on every HF ward wall:
“Decongestion is not just symptomatic relief. It changes outcomes.”
#CardioTwitter #HeartFailure #Cardiology #Decongestion #Diuretics
📄 2025 ESC/EACTS Valvular Guidelines: imaging perspective
🔗 DOI: https://t.co/X7MTuO2DZF
🫀 Core message
The new guidelines mark a major shift:
👉 from a single decision (surgery vs transcatheter)
👉 to a lifetime management strategy
➡️ In this framework, imaging becomes central to Heart Team decision-making.
🔑 Key clinical updates
Aortic stenosis:
👉 Age threshold for TAVI lowered to ~70 years
👉 Decisions now based on lifetime strategy (redo options, coronary access, anatomy)
Primary mitral regurgitation:
👉 Surgery remains the gold standard
👉 Earlier intervention recommended in selected asymptomatic patients
Atrial secondary MR:
👉 Recognised as a distinct entity
👉 New indications for surgery and transcatheter therapies
Tricuspid regurgitation:
👉 Transcatheter therapies enter mainstream guidelines
👉 Strongly dependent on RV function and pulmonary hypertension
🧠 New role of imaging
👉 No longer just to “confirm severity”
👉 But to shape the entire clinical pathway
Three key shifts:
From single parameters → integrated phenotyping
Right modality at the right time
Standardisation and reproducibility
🖥️ Role of imaging modalities
Echocardiography: first-line, now expected to be integrative (3D, stress)
CT: crucial for anatomy, feasibility, and lifetime planning
CMR: reference for volumes, regurgitation, and myocardial damage
Multimodality imaging: essential for complex decision-making
🔄 Paradigm shift
👉 Imaging-driven pathway:
DEFINE → SELECT → DELIVER → TRACK
➡️ Moving from thresholds → personalised, predictive care
🤖 Future: AI in imaging
👉 Not just automation, but:
standardisation
detection of discordance
guideline-based decision support
⚠️ Must remain transparent, validated, and clinically accountable
🚨 Bottom line
👉 Imaging is now:
a continuous, central, decision-making tool in valve disease
👉 Not just measuring valves
➡️ but guiding lifelong patient management strategies
Médicos y estudiantes, a la vez, pidiendo la dimisión de Mónica García.
Decía que venía a mejorar el sistema sanitario y se lo ha cargado en unos meses. Tremendo.
#MónicaGarcíaDimisión
¿Cómo estudias cardio? ¿Con el Topol o con el Braunwald?
Yo con el Braunwald !
Pregunta esencial para los resis de cardio de mi época.
Se ha ido uno de los padres de la cardiología moderna.
Eugene Braunwald.
Su visión pionera en investigación grupo #TIMI, su aportación en entender la fisiopatología de la IC, CI….
Nos deja un gran legado.
Nuestro referente.
DEP🕯️
Especial médicos🩺⚕️🏥👨🏻⚕️👩🏻⚕️.
Os dejo esta carta en JAMA. Se la pondré a mis alumnos en la próxima clase:
He elegido estas frases :
👇🏻⏰
«La medicina puede tener un significado extraordinario. Pero no puede sustituir el estar presente en tu propia vida. El mundo puede necesitarnos como médicos. Pero las personas que nos aman nos necesitan como nosotros mismos. Y ese es el rol que nadie más puede llenar.»
«La residencia refuerza la lección de que las instituciones están diseñadas para perdurar más allá de los individuos. En cambio, las familias no.»
«Creo en formar a la próxima generación. Creo en el significado de este trabajo. Lo que ha cambiado es mi disposición a absorber el desgaste sin cuestionarlo.»
«Ya no estoy dispuesta a seguir posponiendo la vida. La medicina exige mucho. Y nosotros damos profundamente. Pero no puede tomarlo todo.»
«El significado de mi trabajo es profundo. El significado de mi presencia en casa es irremplazable.»
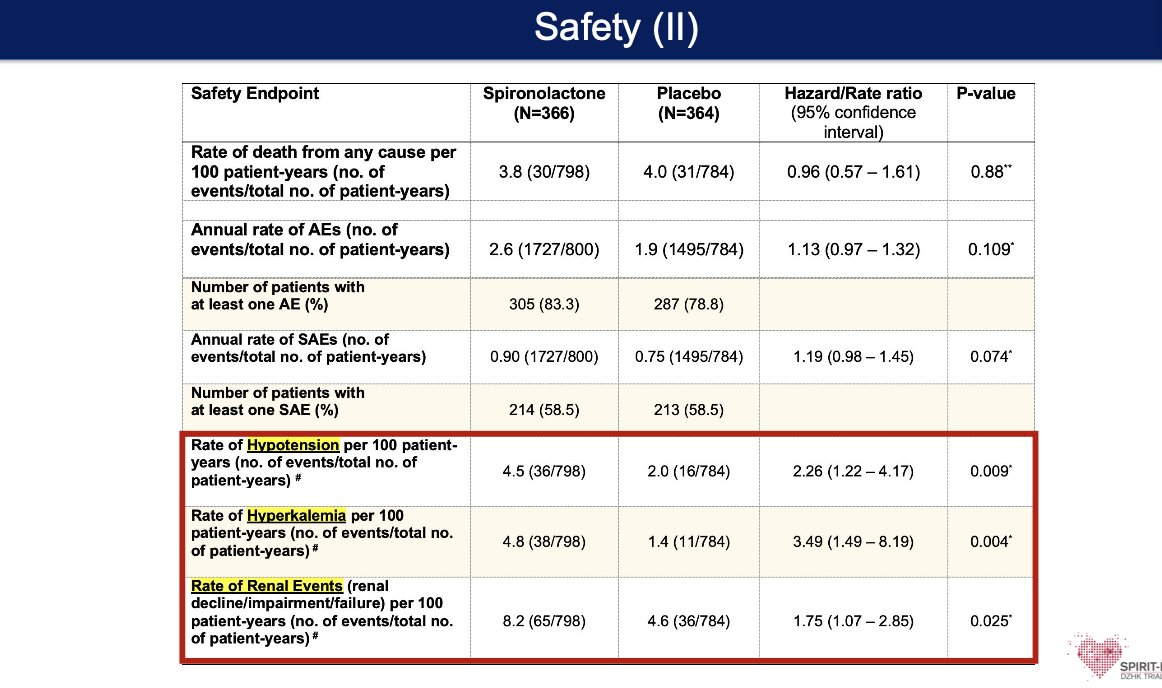
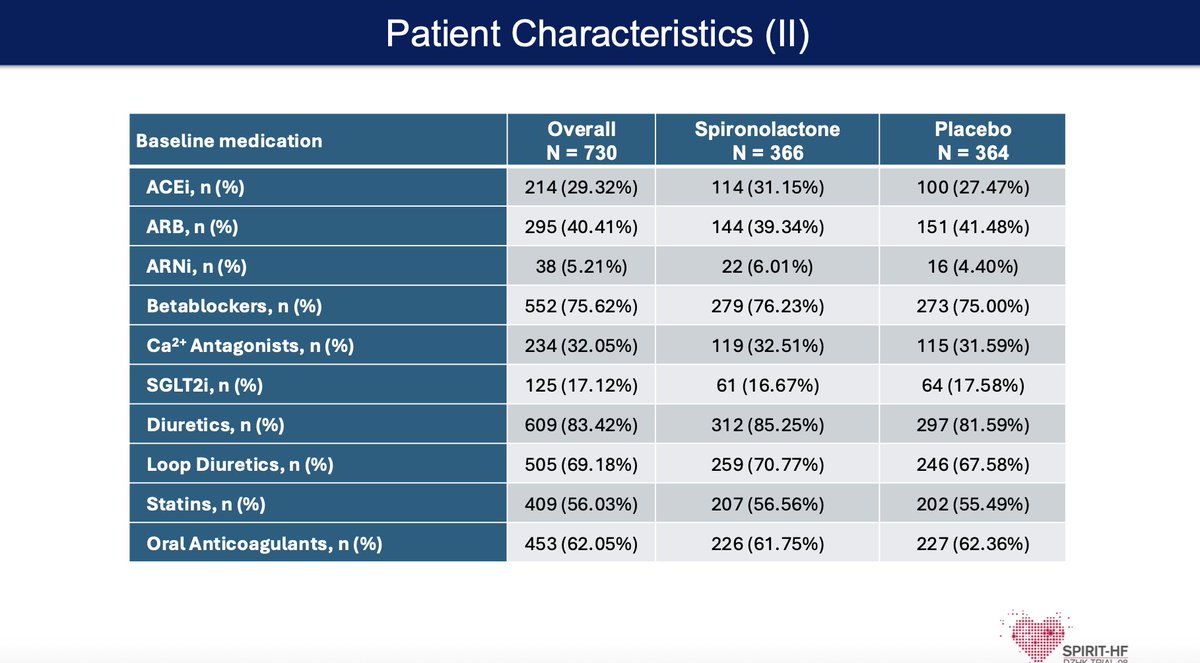
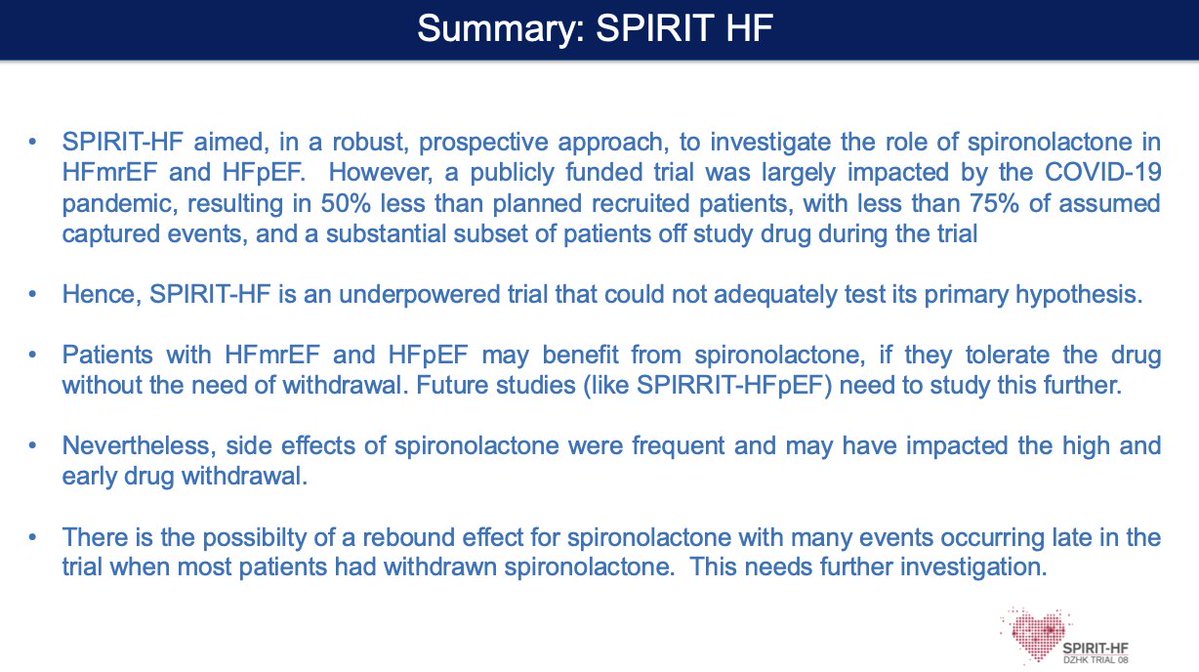
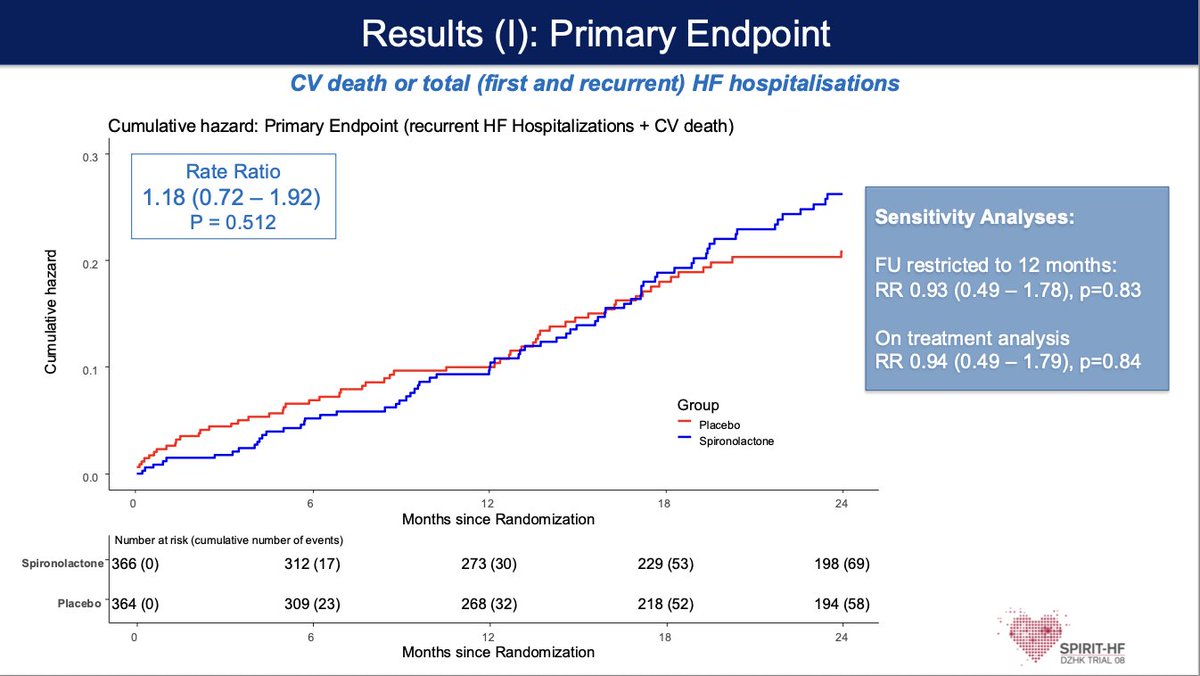
#SPIRIT-HF #ACC26
🧑⚕️ HF with preserved or mildly reduced EF (HFpEF/HFmrEF)—a large, underserved group with limited therapies
🧠 Does Spironolactone reduce CV death and HF hospitalizations, building on signals from prior trials like TOPCAT
📊 Trial was underpowered (COVID impact, lower enrollment, high drug discontinuation) → unable to definitively test hypothesis
⚠️ No clear primary outcome benefit; side effects and drug withdrawal were common, potentially blunting efficacy
💡 Takeaway:
Signal for benefit may still exist—but tolerability + adherence remain the real barriers in HFpEF therapy
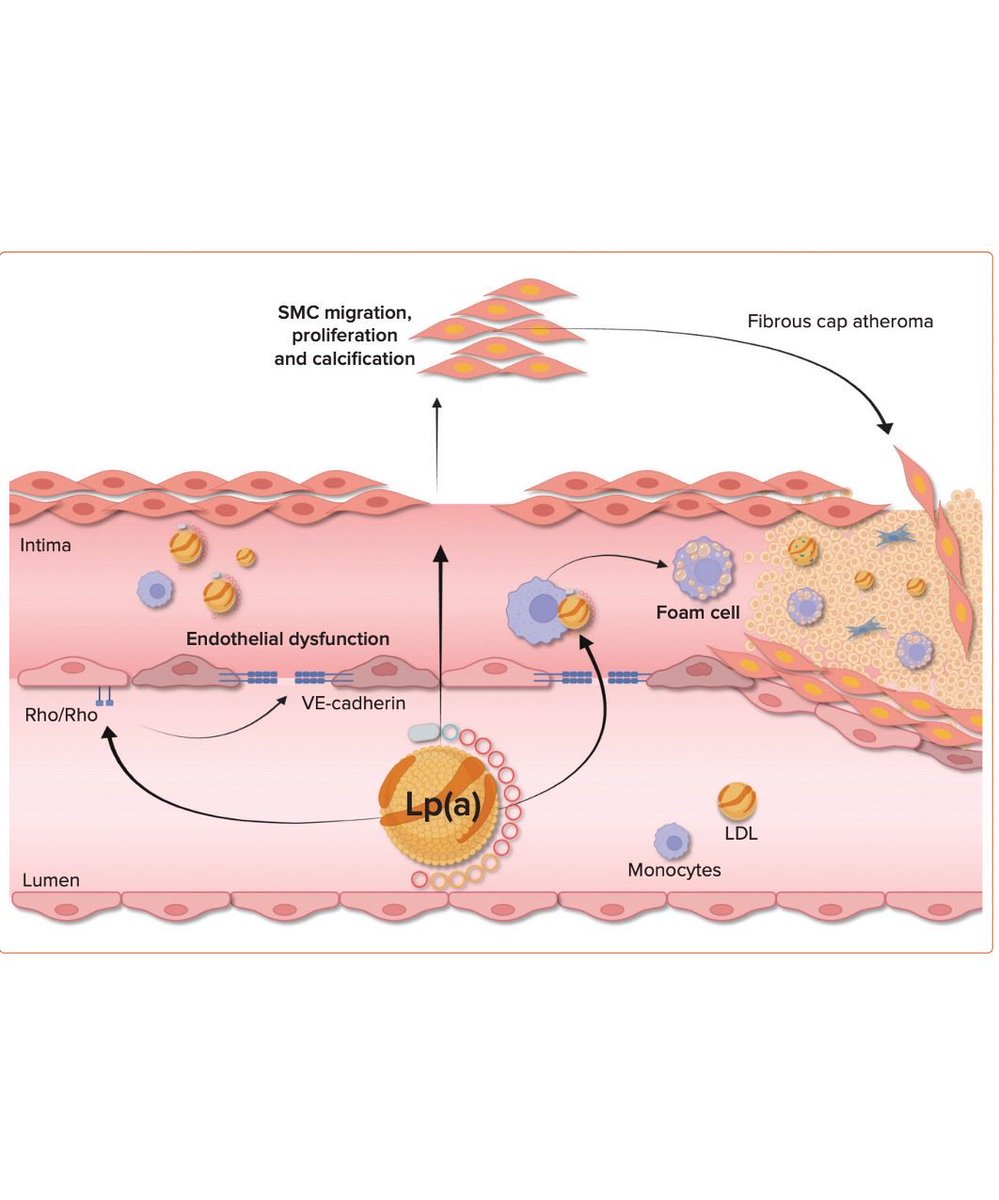
Great Discussion by @dranulala 👏👏
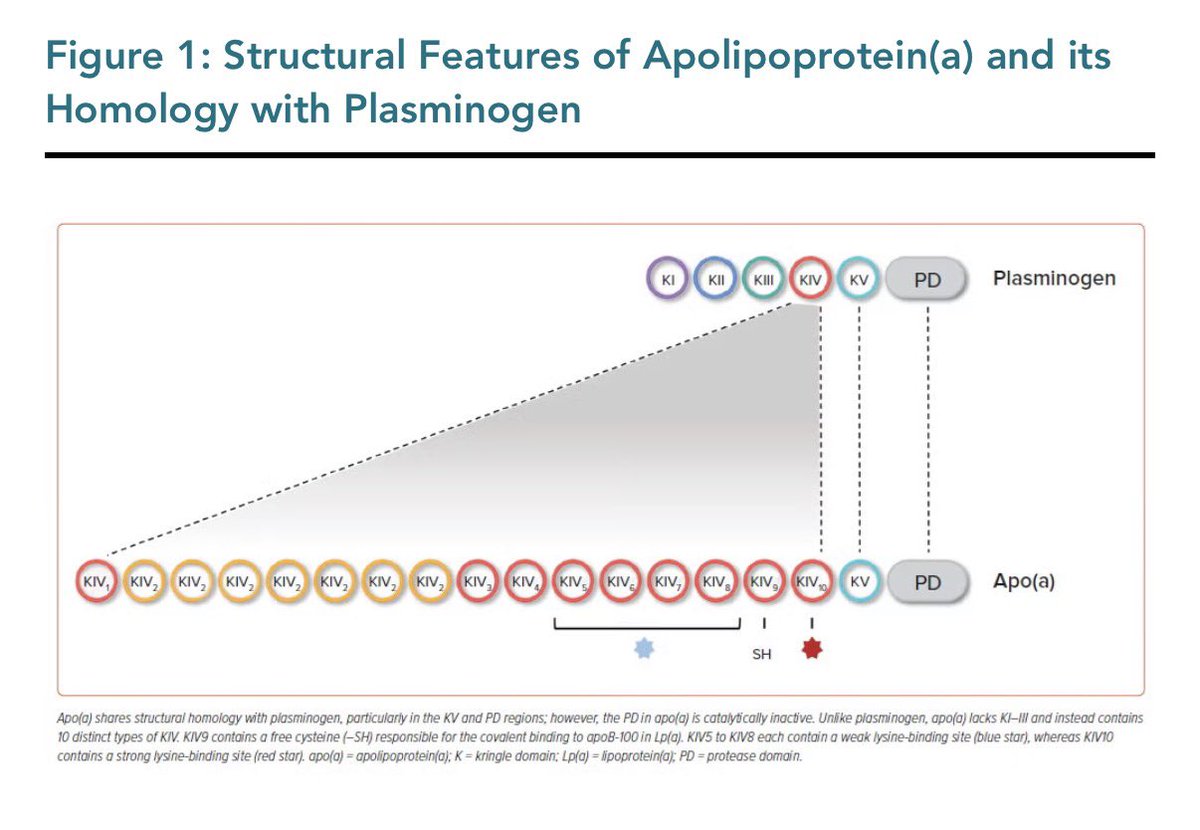
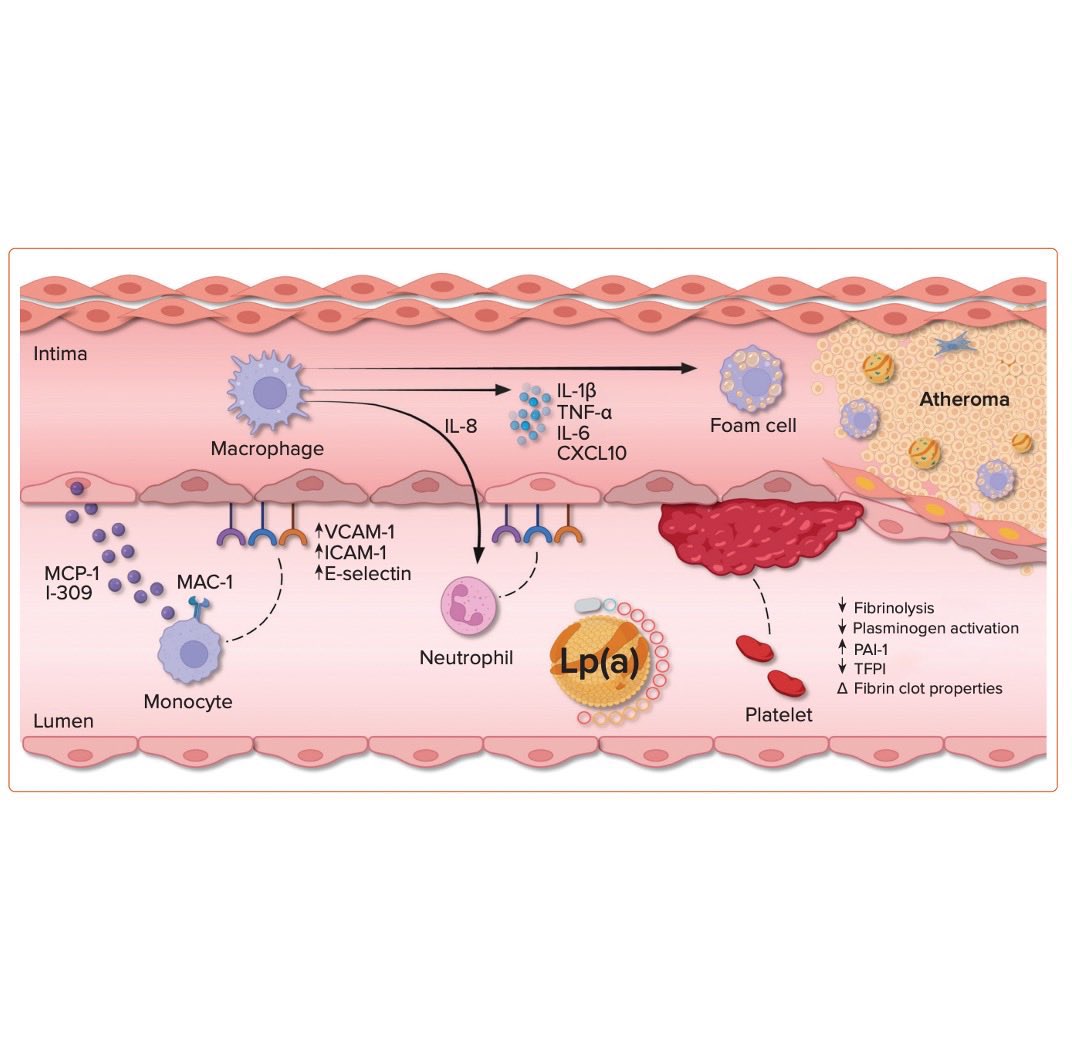
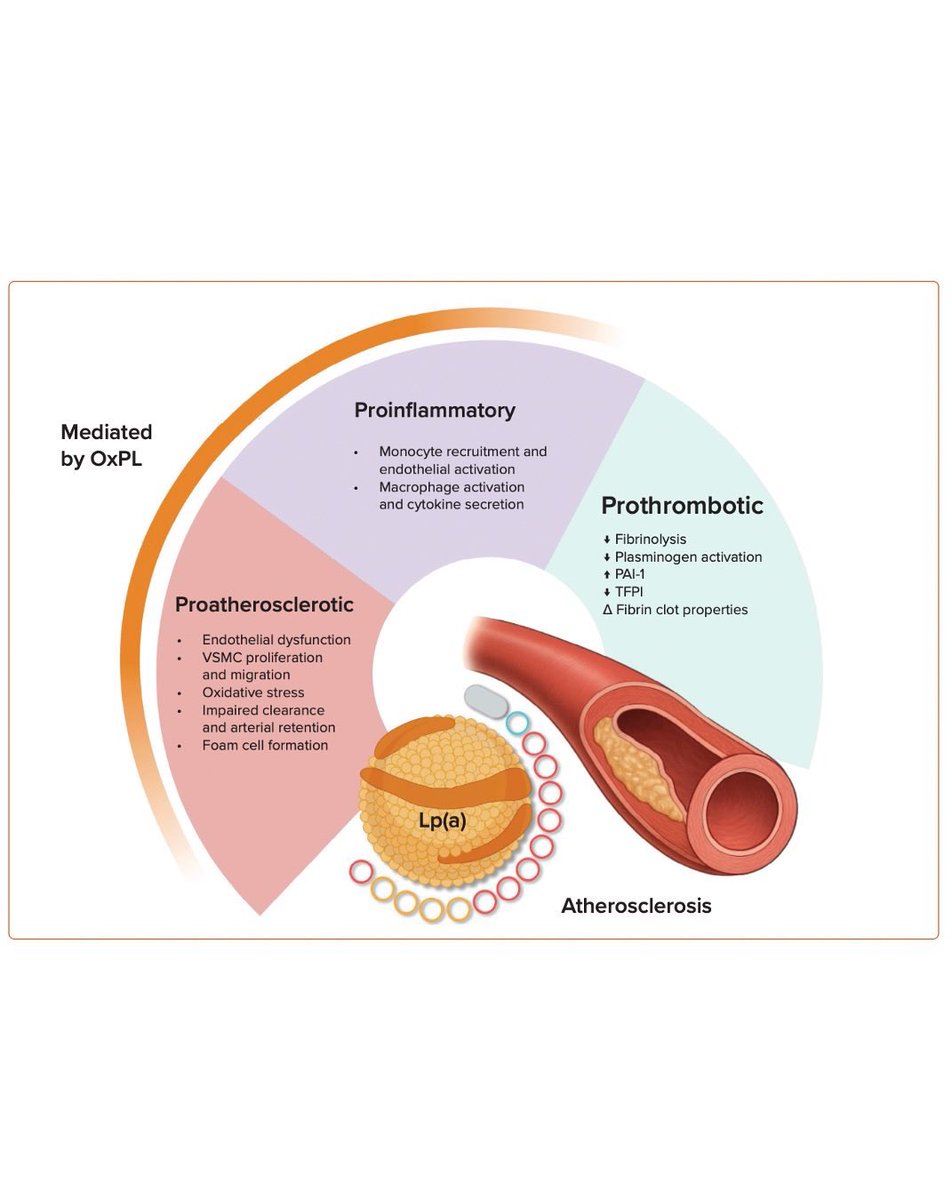
How does Lp(a) drive atherosclerosis?
🫀Delivers cholesterol to the arterial wall
🫀Carries oxidized phospholipids → vascular inflammation
🫀Interferes with plasminogen → impaired fibrinolysis
🫀Promotes an atherothrombotic environment
Understanding these mechanisms strengthens the case for targeted Lp(a) therapies
📎 https://t.co/ja7sUhNbRj
@drmarthagulati@AnnalisaFiltz@CardioMDPhD
🙏🏽 @DrDerekConnolly for inviting this review
#Lpa #CardioTwitter #CVprev
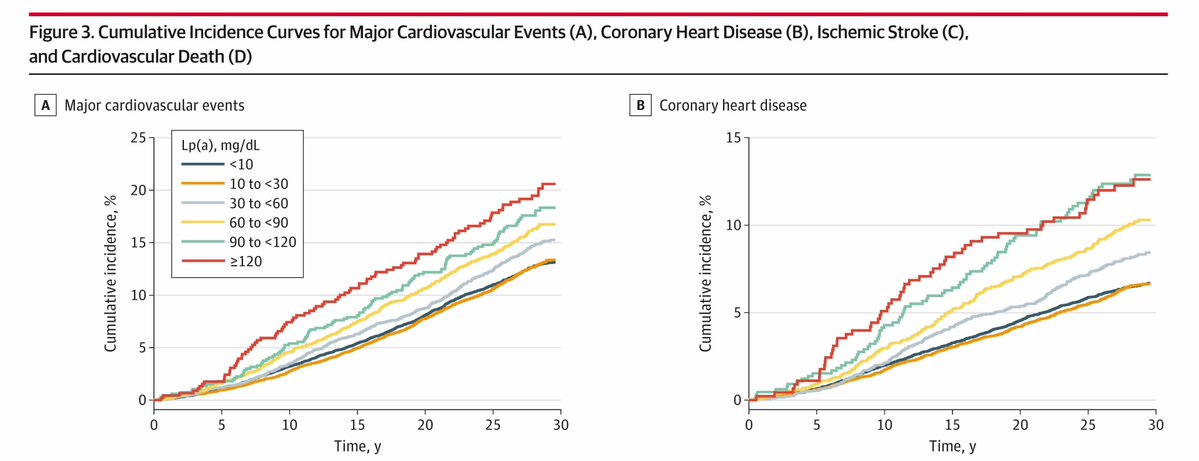
Very high lipoprotein(a) levels are associated with increased 30-year risk of major #cardiovascular events, coronary heart disease, ischemic #stroke, and cardiovascular death among healthy women.
https://t.co/9ufhrgyTbU
🧪🌿 Colchicine slows coronary plaque progression in stable CAD — first randomized imaging evidence
A new randomized, double-blind, placebo-controlled trial in European Heart Journal – Cardiovascular Imaging tested whether low-dose colchicine — a classic anti-inflammatory drug — affects coronary plaque progression in patients with stable coronary artery disease (CAD).
📍 Study design:
• 84 adults with angiographically confirmed CAD or a high coronary calcium score (>400)
• Randomized to colchicine 0.5 mg/day vs placebo for 12 months
• Standard care continued in both groups
• Serial coronary CT angiography (CCTA) assessed plaque change
🧠 Why this matters
Inflammation is a key driver of atherosclerosis progression and vulnerability. Prior clinical trials showed colchicine reduces cardiovascular events, but its direct effect on coronary plaque morphology and progression was unclear.
🫀 Key findings:
• Colchicine significantly reduced progression of total plaque volume, particularly low-attenuation plaque — a marker of high-risk, lipid-rich, unstable plaque
• Slower plaque progression was evident even when LDL levels were similar between groups
• Treatment was generally well-tolerated at 0.5 mg daily
📊 Clinical implications:
This trial provides mechanistic evidence that colchicine’s event-reducing benefits may be mediated through direct influence on plaque biology, not just systemic inflammation. Slowing plaque progression — especially of vulnerable components — aligns with reduced risk of future events.
⚠️ Nuances:
• Modest sample size and single-timepoint imaging limits broad generalization
• Plaque imaging biomarkers predict risk but are surrogate endpoints
📌 Bottom line:
Low-dose colchicine, added to standard therapy, slows coronary atherosclerosis progression in stable CAD — supporting its emerging role in targeted residual risk reduction beyond LDL lowering.