I am so grateful to share that I passed oral boards and am officially boarding certified in #radonc! Huge thank you to @radoncresidency & my study group. While residency is still fresh in my mind, I look forward to sharing some advice to any residents that may find this useful.
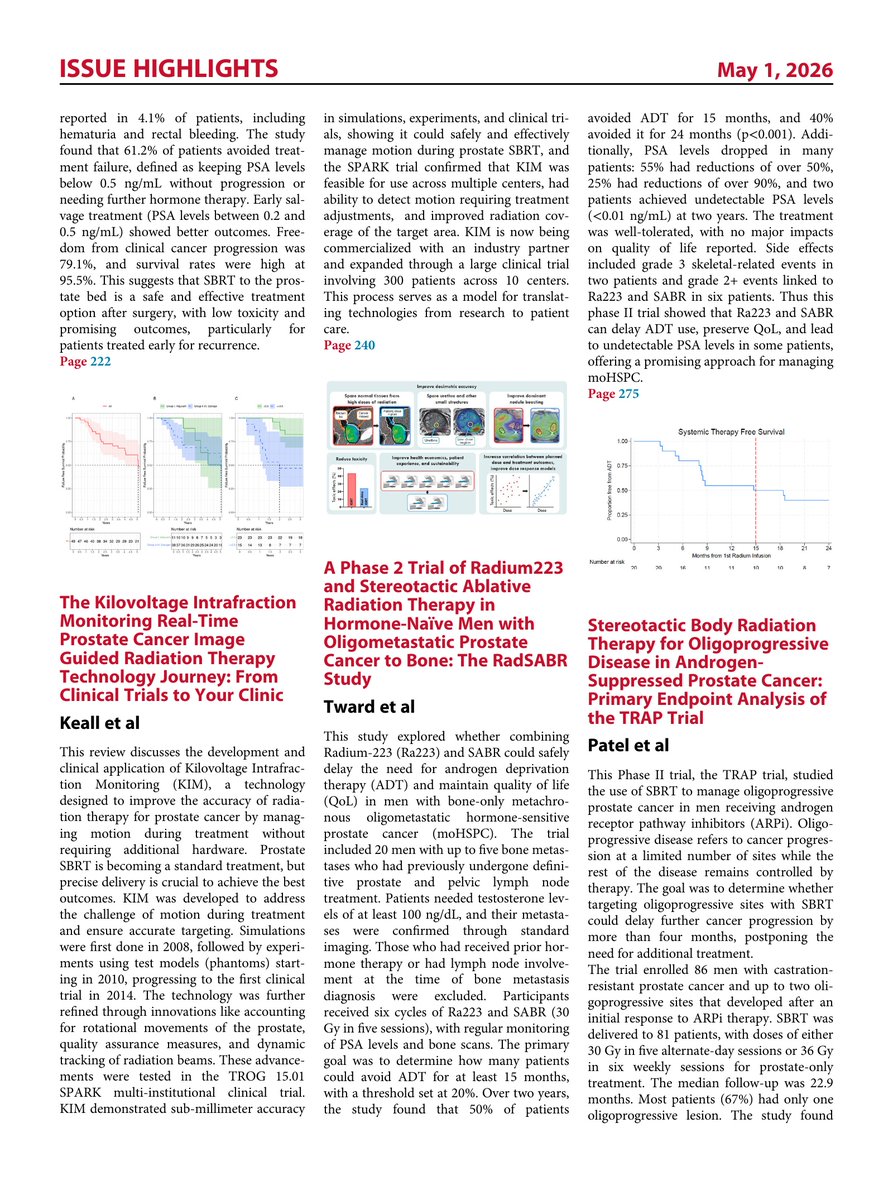
Just released! Volume 2 of SBRT: From Clinical Trials to your Clinic in @IJROBP
Truly amazing papers from end to end. Have a look at the issue highlights here.
https://t.co/1U0ryJHIjw
📌 Top 10 Tips for Stereotactic Body Radiation Therapy Contouring and Planning in Oligometastatic Disease: Lessons Learned From the UK SBRT QA Program ☢️
🔗 https://t.co/WkZDZSoA4I @OncoAlert#OncoAlertAF@IJROBP@fifimcdrmh@royalmarsdenNHS 🔹Standardize definitions. 🔸 Optimize use of supporting imaging.
🔹 Motion management.
🔸 Optimize patient preparation.
🔹 Use all available TPS tools to optimize contouring.
🔸 Check auto-contouring output.
🔹 Appropriate use of OAR dose-volume constraints.
🔸 Maximize PTV coverage.
🔹 Conform tightly to the PTV.
🔸 Managing multiple lesions.
📣 DON'T FORGET: The next #ISRSWebinar
The Role of the Biological Effective Dose (BED) in SRS
🗓️ April 1, 2026 | 2pm CET
🥼 Ian Paddick, MSc, MIPEM, CSci
Consultant Physicist Past-President of the BRSS Co-Chair of the ISRS Certification Committee Honorary Research Fellow at UCL
The role of the Biological Effective Dose (BED) was developed to account for sub-lethal DNA repair effects during exposure and the resulting decrease in the clinical effect of the radiation. In conventional radiotherapy, where treatment times are short (≤10 minutes), sub-lethal repair is minimal. However, in radiosurgery, where treatments can take tens of minutes to deliver, the overall treatment time can reduce the BED of a treatment by a significant amount. This effect, evidenced originally in clonogenic cell survival studies, then animal models, has now been shown to have an important influence in clinical outcomes of SRS. The rationale for prescribing according to the Biological Effective Dose will be explored.
👉 REGISTER: https://t.co/EO5xl98jvk
What is the rate of sacral fracture (SF) after short course pelvic ☢️ for rectal cancer?
In this single institution series (n=171), pts w/ rectal adeno received short course RT (25 Gy in 5 fx), consolidative chemo, and surgery (or non-operative management). From mFU 2.2yrs:
🔘 Crude incidence SF = 7.6%
🔘 2yr cumulative incidence SF = 8.8%
🔘 Median time to SF = 1.64 yrs
🔘 Most (84.6%) SF were asymptomatic
🔘 On MVA, 🔼 SF risk if ♀️ (aHR 6.01) and hx of osteoporosis (aHR 7.37)
🔗 - https://t.co/MoUKtqA3Ke
@JHMRadOnc@ASTRO_org #radonc
FREE for ASTRO members-in-training!
Join us on Thursday, April 2 at 1:00 p.m. ET for a Live Webinar:
"eContouring for Functional Radiation Medicine - Osteoarthritis & Fibromatosis," with speaker Jessica Schuster, MD, from the University of Wisconsin-Madison.
Supported by Speed of Light - The ASTRO Foundation's Juan A. del Regato Fund
Register now: https://t.co/G5R1lqETDX
@ARRO_org@RadOncPDs@UW_RadoncDHO
CONVERT V/S PROSPECT in Rectal cancer
Radiation for all LARC? Not anymore.
CONVERT + PROSPECT challenge routine CRT.
✔ Comparable DFS & OS
✔ Local control >96%
✔ Major reduction in long-term toxicity
MRF uninvolved?
Low-risk T2N+/T3N0–1?
Selective RT is here.
#RectalCancer #Oncology #ASCO #MedTwitter @NiuSanford@OscarTahuahua@OncoAlert@hoperugo@ASCOPost@JCO_ASCO@NEJM@dr_yakupergun@myESMO
Can we skip pelvic RT in selected LARC? CONVERT says maybe. 🎯🧠
CONVERT trial | JCO 2026
In locally advanced rectal cancer with uninvolved mesorectal fascia (MRF-negative), neoadjuvant CAPOX alone achieved very low local recurrence, similar DFS and OS, and less long-term toxicity compared with standard chemoradiation.
🧪 Study population
LARC within 12 cm from anal verge
MRI-confirmed uninvolved MRF
Median follow-up 48 months
⚔️ Treatment strategy
🟦 CAPOX x4 cycles → surgery
🟥 Pelvic RT + capecitabine → surgery
📊 Key 3-year outcomes
LRRFS 97.4% (CRT) vs 96.3% (CAPOX) | HR 1.40
DFS 89.2% vs 87.9% | HR 0.88
OS 95.0% vs 94.1% | HR 0.86
🛡️ Long-term toxicity matters
Grade 2-4 late AEs 26.3% (CRT) vs 16.0% (CAPOX)
Chronic proctitis 41.7% vs 33.6%
🧠 Clinical interpretation
Non-inferiority was not formally met due to extremely low event rates.
But efficacy is comparable and toxicity clearly favors CAPOX-only.
This supports RT de-escalation discussions in carefully selected MRF-negative LARC.
🔖 Save for MDT discussions
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #RectalCancer #ColorectalCancer
@OncoAlert@myesmo@esmo_open@asco@JCO_ASCO
📌 Radiotherapy With a 12-Gene Expression Assay for Ductal Carcinoma In Situ
A Randomized Clinical Trial
🔗 https://t.co/O95CMEGq0o
@OncoAlert#OncoAlertAF@JAMAOnc
Cumulative dose evaluation in clinical reirradiation – Consensus guidance
on technical considerations by the ESTRO reirradiation focus group
https://t.co/VCkl4vnOxG