Professor of Respiratory Medicine, CHU Grenoble-Alpes. Honorary president IFCT Intergroupe Francophone de Cancérologie Thoracique. My opinions are my own.
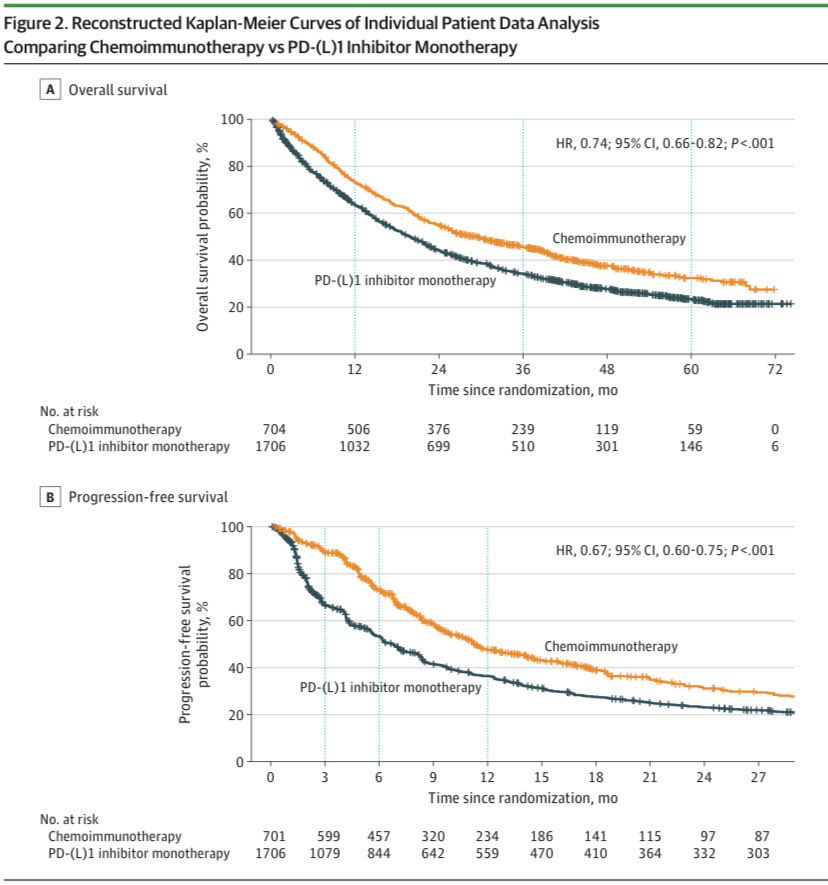
What does chemo add to immunotherapy in pts w/ PD-L1-high NSCLC?
In our meta-analysis of 24 trials w/ reconstructed individual patient data, we observed a meaningful improvement in both median PFS (11.3 vs 6.8 months, HR 0.74) and OS (29.2 vs 19.8 months, HR 0.67) w/ chemo-ICI.
🫁 Thanks to @StephenVLiu for joining us at #ASCO26 for an excellent interview on new data and key updates in SCLC!
🌟 Stay tuned for the interview!
➡️ Find more lung cancer news from #ASCO2026 here: https://t.co/0ZzNtp5Gk1
#SCLC#lcsm
LORIN; neoadjuvant lorlatinib
pCR 47% MPR 81% in both resectable and unresectable stage III; P2; 3cycles of lorla preop or preCRT; this is stellar and dare I say practice changing where possible #ASCO26
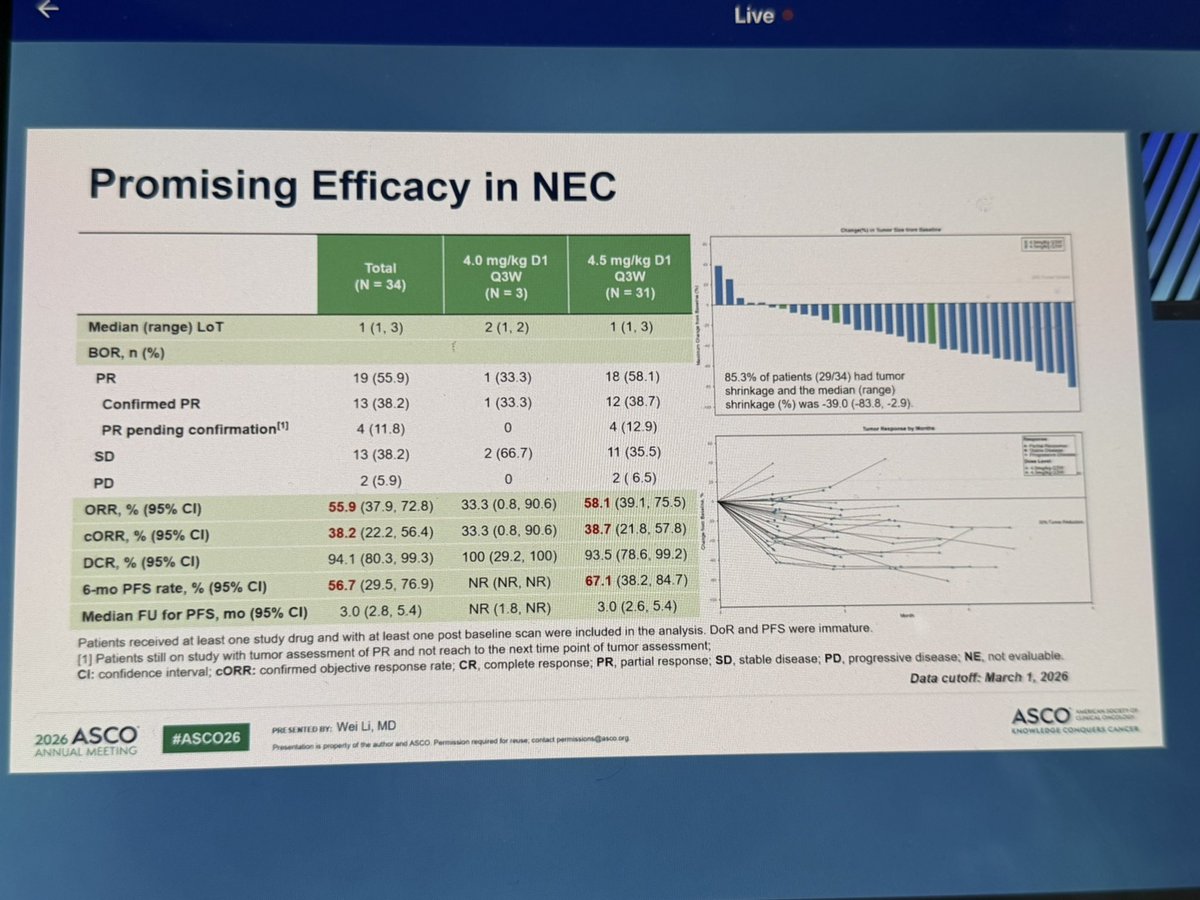
Novel ADCs for SCLC with TOP1 inh payload include CD56 (NCAM) and DLL3, both neuroendocrine markers. Impressive ORR in pretreated patients and no sign of ILD. Interesting finding of encouraging responses in patients previously exposed to irinotecan. #ASCO26#LCSM
🧵 Should we ditch etoposide in SCLC chemo-IO combos?
data from IFCT-2203 TAXIO (Abs 8091) suggests it might be time
⚡ Rationale: potential antagonism between etoposide & immunotherapy has long been suspected — this trial tests a first-line etoposide-free regimen + durva
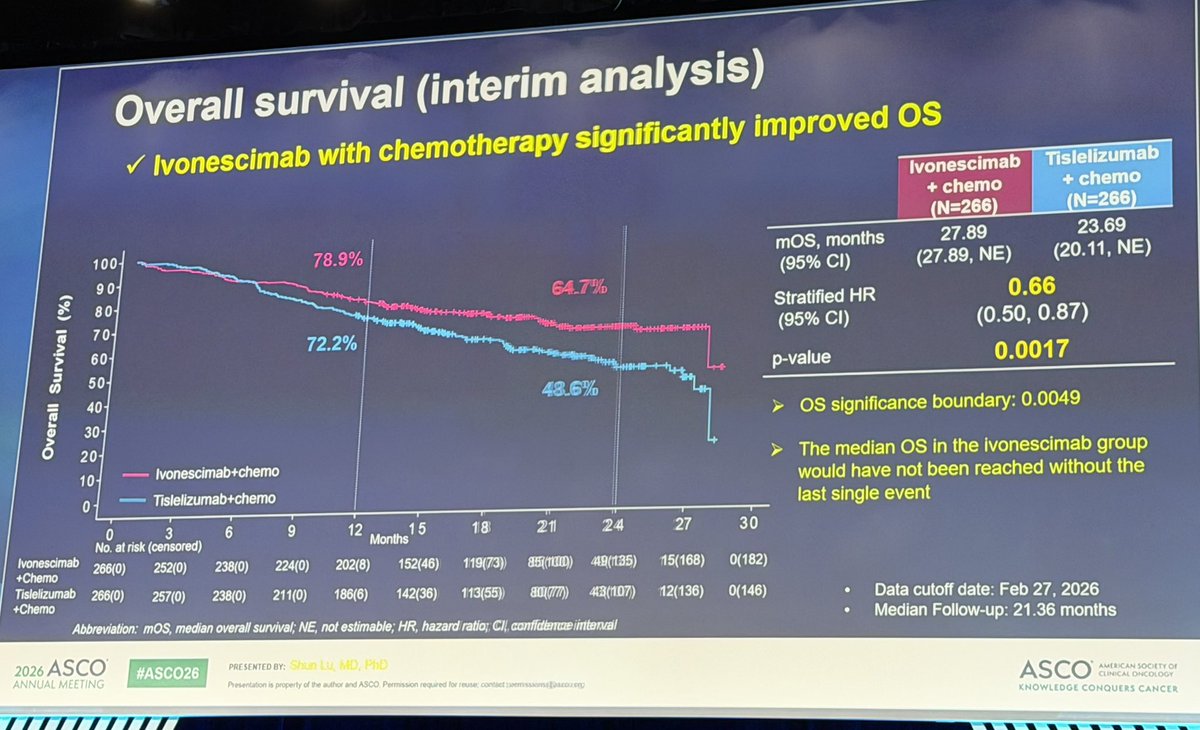
💥 Ivonescimab overperforms tislelizumab in combination with chemotherapy in squamous lung cancer in Chinese population.
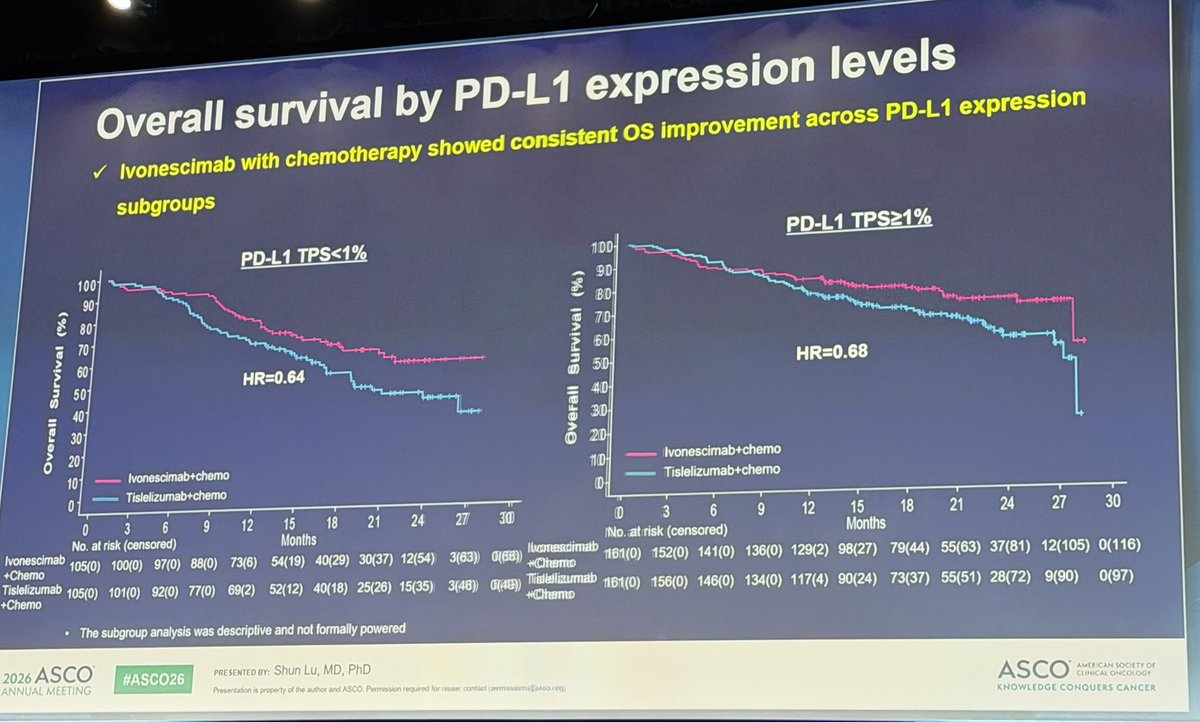
Better OS regardless of PD-L1 expression.
While global confirmatory trial is underway, these results may have immediate implications.
#ASCO26#LCSM
LBA4 #ASCO2026
Ivosnescimab + chemotherapy improved OS vs tislelizumab + chemotherapy in untreated advanced squamous NSCLC:
• Median OS: 27.9 vs 23.7 months • HR 0.66 (34% reduction in risk of death) •
PD-L1 <1%: HR 0.64 •
PD-L1 ≥1%: HR 0.68
In keynote 407 - pembrolizumab plus chemo median OS was 17.2 months .
End of An ERA ? @dr_yakupergun@Alfdoc2@JackWestMD@RManochakian@OncoAlert@ASCO #asco26
TAXIO/IFCT-2203 (Abs 8091): paclitaxel/carbo/durva in 1L ES-SCLC.
👉ORR 82.4%,
👉12-mo OS 57.4%,
👉mOS 14.5 mo,
👉mPFS 4.6 mo.
Safety: grade 3-5 TRAEs 48.5%; 2 treatment-related sepsis deaths.
Bottom line: active + convenient one-day regimen, but toxicity is real and PFS does not scream “better than EP/IO.” would be nice especially for inpatients induction.
#ASCO26 1L elisrasib + pembroizumab in KRAS G12C NSCLC with RR 81% with DCR 98%, mDOR NR with 73% at 12m, mPFS NR with 54% at 12m and 12m OS rate 89%. Illustrative cases showing rapid, deep responses including CNS responses.
Dr. Vincent Lam presents ARCHER trial at #ASCO26: ALK-Vac (prophylactic peptide vaccine) in pts receiving ALK TKI therapy ≥4m with goal of preventing acquired on-target resistance. No SAEs or unacceptable toxicity, encouraging immune responses, only 1 PD so far (KRAS bypass).
Krescendo 170 trial
Supports in 1st L in KRASG12Cmut NSCLC we can avoid platinum-CT as divarasib + pembro reported impressive outcomes in PDL1+ and PDL1- with mPFS in PDL1 + of 19.3 mo. Benefit mainly in high PDL1. Need data from KRESCENDO2 to confirm this important data #ASCO26
Dr. @peters_solange with phase II results from ROSETTA Lung-02 #ASCO26: global study of 1L pumitamig (PD-L1 / F+VEGF-A bispecific antibody) plus chemo in NSCLC. Preclinically, pumitamig an effective PD-L1 and VEGF-A antagonist and forms complexes that lead to internalization.
Dose-reduced lorlatinib (50mg or 75mg) works just as well as full-dose lorlatinib (100mg). Don’t be afraid to reduce the dose (or even start at a lower dose) if patients are struggling with or worried about toxicity! @ALKPositiveinc#ASCO2026
Sacituzumab tirumutecan +pembro ⬇️ 65% risk of PD vs pembro alone in PDL1>1% mNSCLC in interim analys including Sq!!
Crowded space of ADC antiTROP2 in 1st line combined with IO
Geographical representation of the trial (only in China) may limit regulatory approval by FDA?#ASCO26
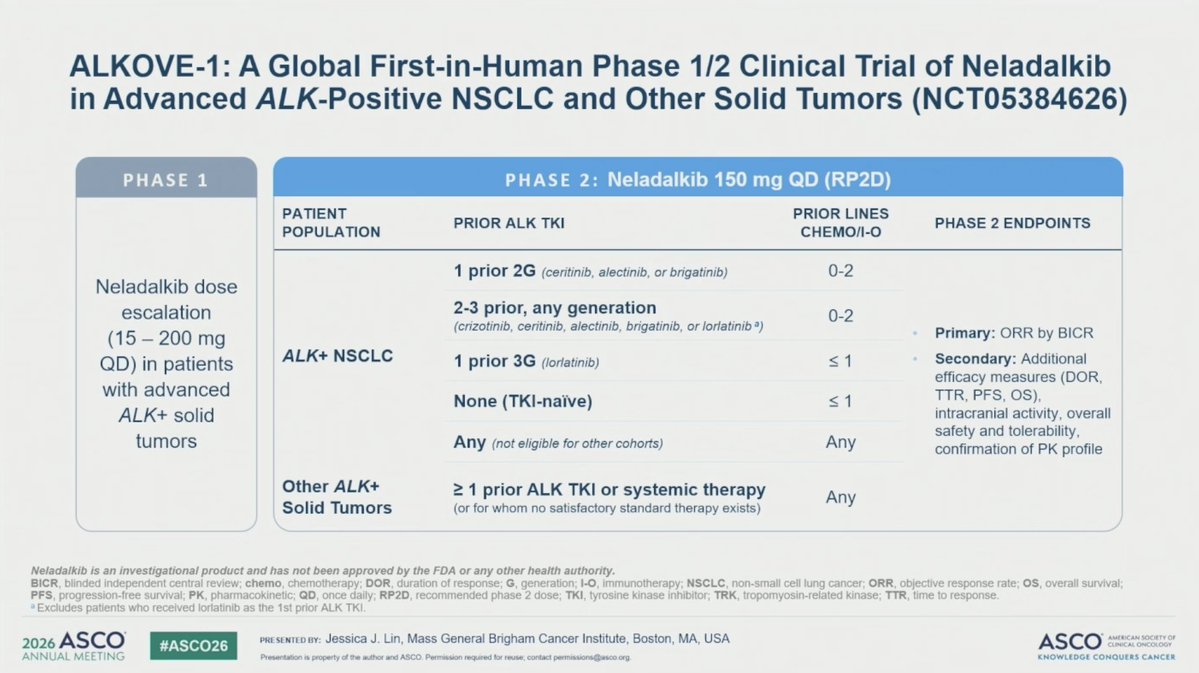
Dr. @JessicaJLinMD at #ASCO26 with an important update from ALKOVE-1: phase 1/2 study of neladalkib (NVL-655) in ALK+ NSCLC. Included 253 patients previously treated - median 3 prior lines, 95% had prior 2G TKI, 75% with prior lorlatinib.
‼️ Phase 3 WU-KONG28: 1L Sunvozertinib v Chemotherapy in EGFR exon20 NSCLC
▫️mPFS 10.3 v 7.5 mos (HR 0.65)
▫️ORR ~60% v 30%
Keep in mind, 1L PAPILLON (Amivantamab + chemo) is currently our SOC (mPFS 11.4 mos, ORR of 73%)
#ASCO26@ASCO