1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
Whole blood in trauma has generated enormous interest. Today, @SWiFT_trial in @NEJM provides the clearest randomised evidence so far on whether prehospital whole blood improves outcomes in life-threatening traumatic haemorrhage: https://t.co/iqgPNZNdfk
Everyone who works in healthcare needs to read this mum's live account of the ongoing plight of her young son's emergency NHS care - but most of all, @wesstreeting, you need to read it.
This is the reality of NHS 'improvement' on your watch, and it is soul-destroying.
I am so very sorry you and your son are enduring this, Victoria, & that all the staff around you are enduring the same.
Our latest systematic review is now live in @EmergencyMedBMJ. We looked at the association between intra-arrest DBP & CPP and ROSC. The data supports a move toward physiology-guided CPR, with 35mmHg DBP emerging as a potential target. @EMManchester
📄https://t.co/667aBRzlza
Day 2 ESC : Part-2 :
BB in post MI no heart failure studies :
REBOOT- MI: Post MI with EF more than 40%, Beta blocker is not associated with reduction in death or MI or Ischemic events
BETAMI- DANBLOCK: BB helps in pts with MI w/o heart failure
REBOOT/ BETAMI DANBLOCK/CAPITAL RCT: IPD Metanalysis: BB helps in post MI in reducing MACE.
REFINe-ICD: ICD in patients with LVEF 36%-50% with abnormal markers ( Holster abnormal Heart rate turbulence and T-wave alternans) : No use of ICD in reducing all cause mortality or CV death or sudden death.
@RameshSank1975@escardio@NEJM #ESCCongress @SRIHER_Official@SRMC_official
Common pitfalls in airway management
📌I can intubate all my patients with VL
📌I am experienced (but do you have expertise?)
📌Incomplete airway assessment (only looking at anatomical factors)
📌Incomplete airway strategy (no transition points defined)
📌Intubating without muscle relaxants
📌Incomplete pre-oxygenation
📌Awake intubation indicated but not done
📌Underestimation of risk of high BMI
📌Call4help not done in time
📌Never practised EFONA
📌SGA used but tube was indicated
📌No peri-oxygenation technique used
#airwaytriage #patientsafety #meded
Today marks the beginning of Black Inclusion Week, an opportunity to listen to Black voices in Emergency Medicine. Start the week by reading Dr Janos Baombe's story, which is about overcoming obstacles and the positive impact of diverse perspectives in healthcare: https://t.co/Oyj1A6F436
The Intensive Care Society is deeply concerned by the Supreme Court’s recent decision regarding the naming of doctors involved in court of protection proceedings.
Read our full statement below👇
https://t.co/ka9hBVQbzy
While I agree “no one too sick to intubate” I suggest it’s important that this message does not get jumbled into
-don’t be scared to intubate
-don’t be a pussy & hold off intubation
-let’s just intubate
The physiologically high risk intubation is a real thing
-in ED/PHEM
-in ICU
-in emergency theatre
Defo a thing & caused by
-drug choice at induction (avoid prop/remi switch to ket)
-too rapid induction (do you really need this to be an RSI?)
-too big a dose (cut the dose in the sick, go slow)
AND don’t forget
-initiation of positive pressure ventilation. Bad for those with low reserve…..
Definitely a thing in NAP7
https://t.co/nHqbT7mqWA
&
https://t.co/bSuFtCn78K
Cardiac arrest in the critically ill at induction is pretty consistently around 2%.
(We all think we’re an exception….but the data seems to come up with this time & again ….are we really!!)
Yes intubate - if indicated
Be cautious
Be prepared
Consensus statement here
https://t.co/qfOgU0kdwo
The Intensive Care Society congratulates the Faculty of Intensive Care Medicine (FICM) on their announcement that they will transition to become the College of Intensive Care Medicine (CICM) in July 2026.
@FICMNews
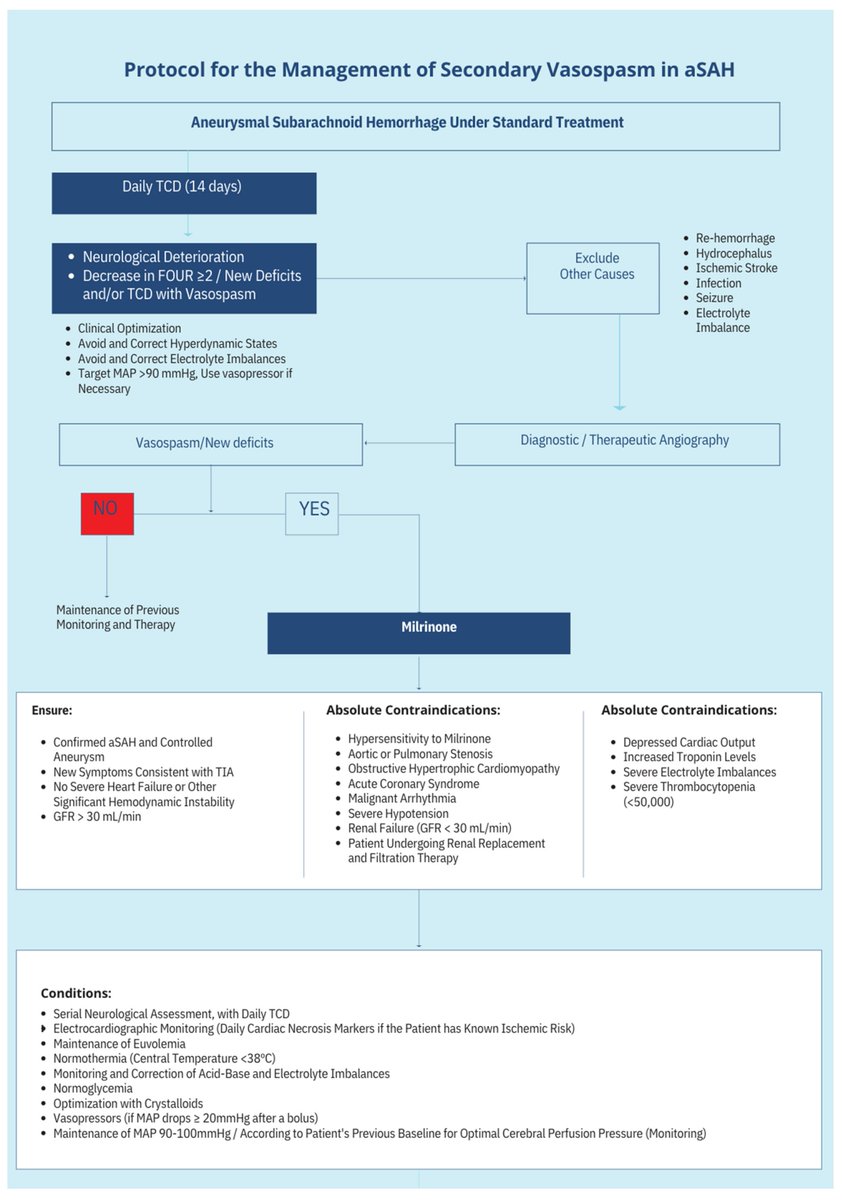
Evidence-Based Approach to Cerebral Vasospasm and Delayed Cerebral Ischemia: Milrinone as a Therapeutic Option—A Narrative Literature Review and Algorithm Treatment Proposition
CCR Journal Watch
https://t.co/Sp06oA6IDG
@pmcbcs
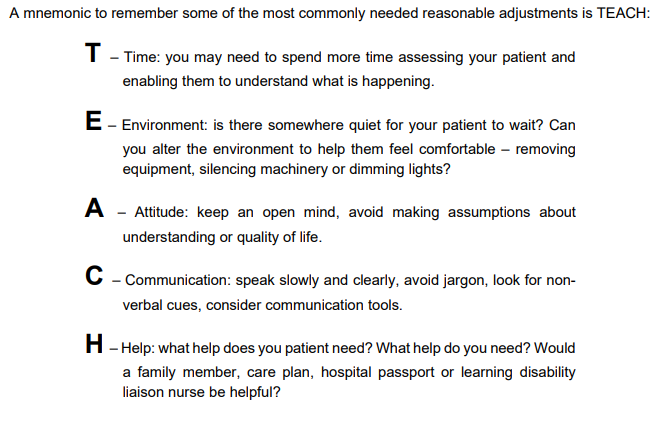
#IDPwD It's International Day of Persons with Disabilities. We have a insightful range of learning to support healthcare workers.
@RCEMevents Caring for patients with learning disability, autism or complex needs in the ED (RCEM On-demand video).
▶️ Register: https://t.co/ycSJRi6Pyu
▶️ More details: https://t.co/Hm0o5qbcSY
▶️ Learning Disabilities Toolkit: https://t.co/S5CYgeld1c
@RCEMLearning
▶️ Down Syndrome for Emergency Physicians: https://t.co/oMrrYUzJQE
▶️ Author: @DrLizHerrieven https://t.co/nFkHc1nx4Q
#IDPD2024