The power to SAVE A LIFE is in YOUR HANDS! A person is 2-3x more likely to survive a cardiac arrest if a bystander gives them Hands-Only CPR. It’s truly miraculous! Don’t know how & want to learn? Let #PBCFR teach you, watch this! Your Safety. Our Priority.
PREACH Jimmy! There are a select few conditions where patients benefit from rapid transport--#EMS is highly capable of stabilizing and treating on scene... Slow Down and Buckle Up, my friends!
@armyemdoc I would disagree for several reasons.
1. Little harm if placed appropriately
2. Other studies have shown reduction in blood product use
3. Physical exam is inaccurate at identifying unstable pelvic fractures when pt are unstable
4. Adjunct to other early resuscitation efforts
Reminder that applications are now open for our 2024 Carolina Wilderness EMS Externship! We will select two Externs (fourth year medical students or resident physicians) and give them an extraordinary field medicine training experience in September 2024. If this sounds like something for you, or someone you know, you can access the application here: https://t.co/r5H6jcpC1n
All applications due by April 1 so don't delay!
[Pictured: MD-67 Stephen Hobson and MD-68 Abigail Wehner, our 2020 Externs, on a night operation]
@CWEMSE@HawkVenture@unch_blue@WPCC_Pioneers@WakeEMresidency@NCparks
🚑 Rural Cardiac Arrest Care in Texas: Despite higher bystander CPR rates, outcomes are worse in rural areas. The study delves into the factors affecting care and survival.
🏥 Read the findings here: https://t.co/Zb4E6TTiHp
Stay tuned for more from @joshkimbre and I on this hot topic. So far it's looking like TCP attempts prehospitally may not reliably result in capture. Exciting as this AHA class IIb treatment may result in more harm than good if it leads to unrecognized failure!
“Does a Cardiologist work in an internal medicine clinic? Then why does an EMS physician feel the need to continue working in an ED? If EMS is your subspecialty, then work in your subspecialty.” - @erdoc1491#NAEMSP2024
I'm getting excited for #NAEMSP2024. Always great catching up with #EMSDoc colleagues and friends and hearing the latest science and updated practice standards. Even more excited to be giving a talk this year with my bro @BrianMillerMD!
Another study on pressors post-arrest?
Researchers studied 221 admitted OHCA patients with Epi vs Norepi infusions with 6 hours of arrest.
No diff in arrhythmias
Epi more likely to die (90.0% vs 54.3%)
Epi more likely to re-arrest (55.7% vs 14.6%)
https://t.co/XpcBGJOeut
Debating rocuronium vs. succinylcholine for RSI?
New research from #UWashEMS shows that within @SeattleFire they have similar Cormack-Lehane grades, first-pass success, & rates of peri-intubation hypoxemia.
Full Paper: https://t.co/cCL8G1XTmN
@DrJeffJarvis A cursory read through this review has a few studies cited that might be helpful.
Hyperventilation in Severe Traumatic Brain Injury Has Something Changed in the Last Decade or Uncertainty Continues? A Brief Review https://t.co/xMYb11rFCO
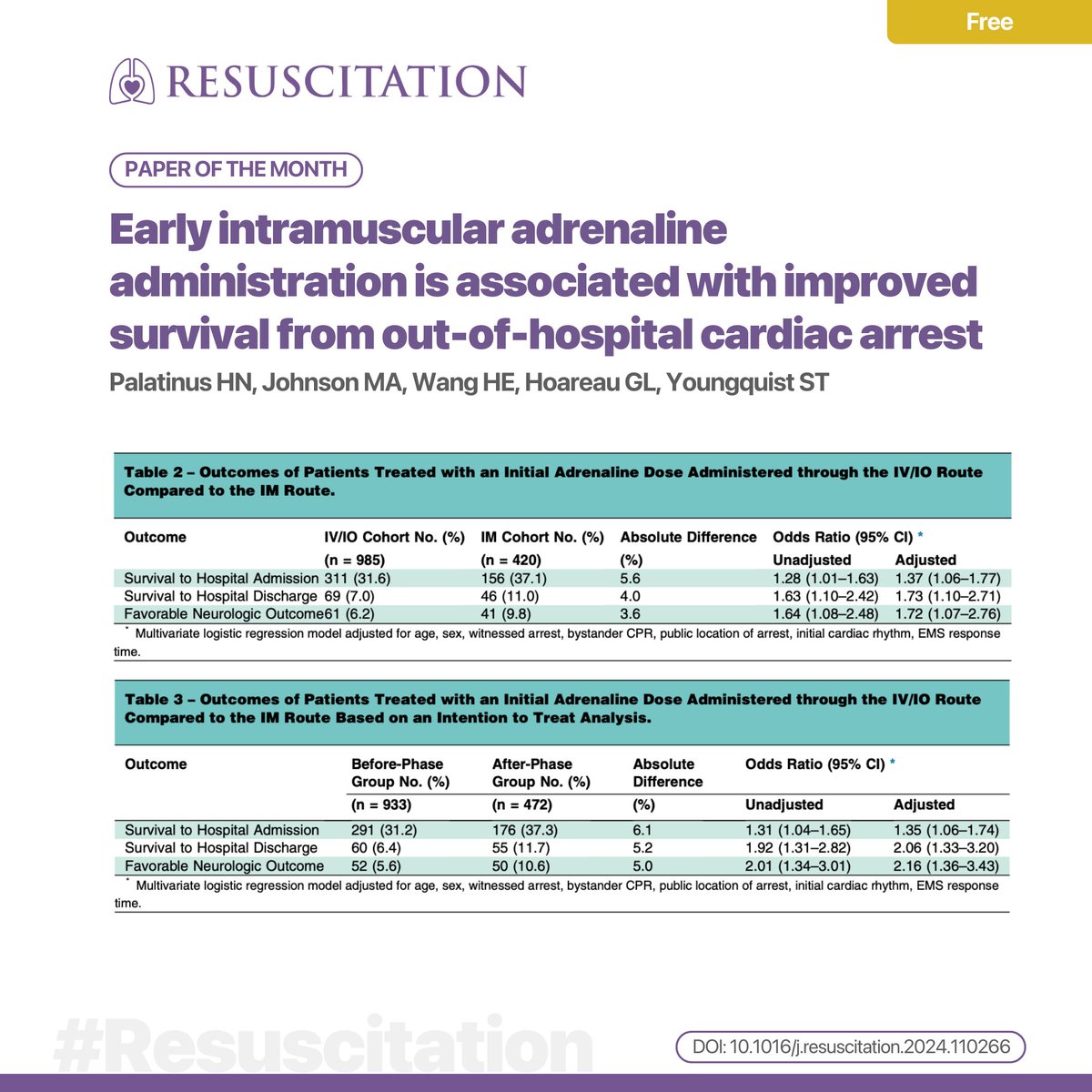
@DrJeffJarvis Saw this one recently different approach to Epinephrin admin.
Intramuscular adrenaline for out-of-hospital cardiac arrest is associated with faster drug delivery: A feasibility ... https://t.co/yRINKrng3h
Harm Reduction is to EMS as fire prevention is to the fire service.
We’re some of the only people in medicine that get 1-on-1 time with patients even after we’re done with what we need to do.
That last bit of time on the ride in is valuable, don’t let it go to waste.
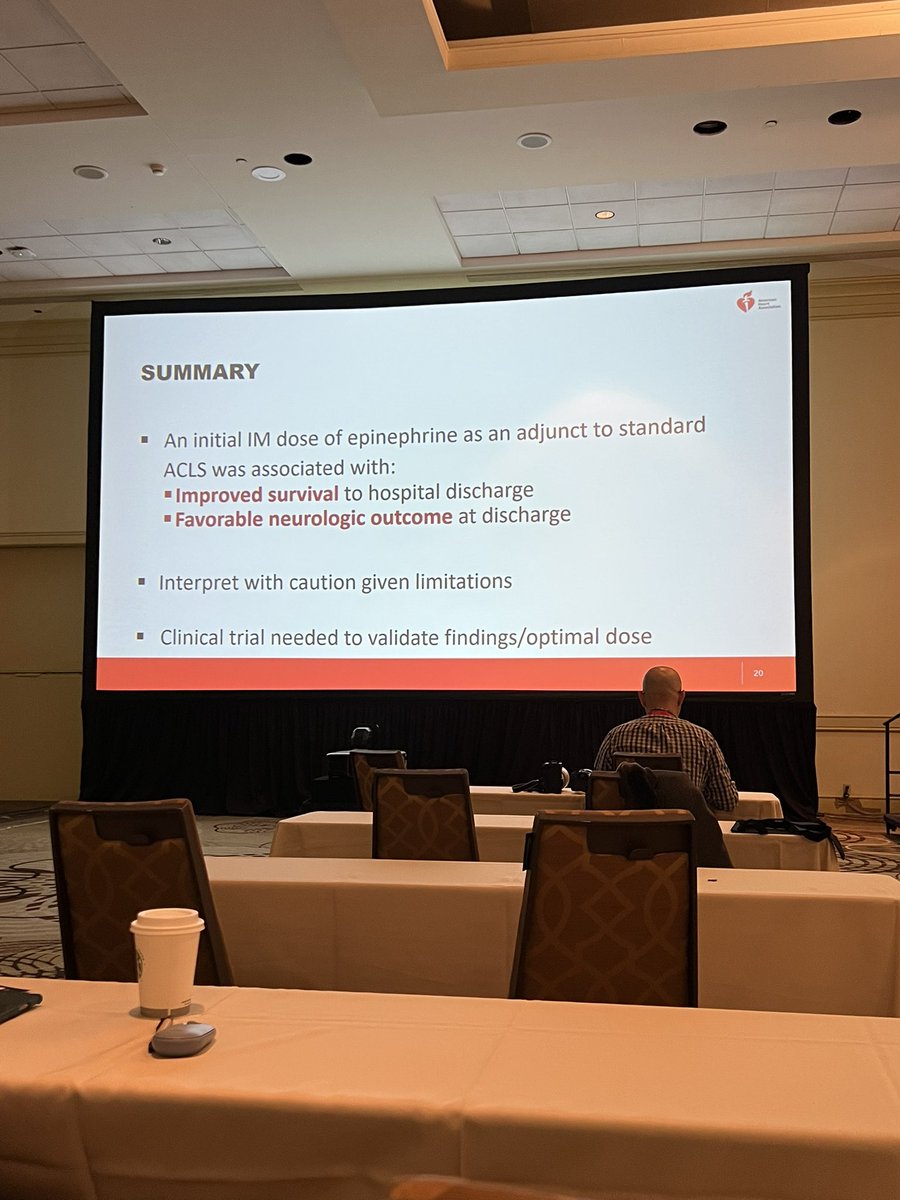
Dr. Palatinus shares the @slcfire experience deploying IM epinephrine in OHCA. #ReSS23
Decreased time to first Epi by 3 minutes, saw no change in hospital admission, but an increase in survival to discharge / good neuro outcomes.






















![hawkvox's tweet photo. Reminder that applications are now open for our 2024 Carolina Wilderness EMS Externship! We will select two Externs (fourth year medical students or resident physicians) and give them an extraordinary field medicine training experience in September 2024. If this sounds like something for you, or someone you know, you can access the application here: https://t.co/r5H6jcpC1n
All applications due by April 1 so don't delay!
[Pictured: MD-67 Stephen Hobson and MD-68 Abigail Wehner, our 2020 Externs, on a night operation]
@CWEMSE @HawkVenture @unch_blue @WPCC_Pioneers @WakeEMresidency @NCparks](https://pbs.twimg.com/media/GGFFQuAaEAA8sy7.jpg)