A mathematician at Bell Labs noticed that the scientists who won Nobel Prizes and the ones who never amounted to anything were equally smart, equally hardworking, and equally credentialed, and the only thing that separated them was a single question almost nobody is brave enough to ask themselves before they die.
His name was Richard Hamming.
He spent 30 years at Bell Labs, in the same building as John Tukey, Walter Brattain, and a long list of physicists who took home Nobel prizes for work they did down the hall from his office, including the legendary Claude Shannon.
His invention of error-correcting codes made modern computing possible. He has won the Turing Award. And all the while he was creating his own legacy he was secretly doing a study on the people around him.
The study was straightforward. 2 Teams. The legends and the lost. Same I.Q.s. Degrees same. Same desk hours. Same access to the world’s best resources.
And yet, at the end of 40 years in their careers, one group had changed entire fields, and the other group could not be remembered by their own colleagues five years after retirement. He wanted to discover what the actual difference was.
In March 1986, he stood before 200 researchers in a Bellcore auditorium and told them what he had seen.
He said it all came down to one question. And hardly anyone he ever met was willing to ask it directly.
He called it the Friday-afternoon ritual. He spent years blocking out his Friday afternoons and not doing anything productive with them every week. No experiments. No meetings. No deliverables.
He called it Great Thoughts Time. He sat down with a notebook and asked himself a couple of questions in order. What are the most relevant problems in my discipline? And why I am not working on either of them.”
Most weeks, the answer was the same, he said. For a week now he had marched confidently in a direction he did not think was the most important direction. He was a goer. He worked a bit. He was getting clean results that would publish in respected journals. (
And for five days straight he'd been lying to himself about whether any of it mattered.
The reason almost nobody does this ritual is because the honest answer is unbearable. The thing is that if you sit down on a Friday afternoon and say out loud that you are not working on the most important problem in your field, now you have to do something about it.
You have an immediate change in direction, or you have to keep lying to yourself every week from that point on. Most people choose the lie.
In the short term it’s cheaper, but over a career it’s more expensive.
Hamming took the ritual a step further in the Bell Labs cafeteria. He began approaching scientists he barely knew, asking them what they thought the most important problems in their field were.
A week later he would ask them why they had not worked on these problems. Eventually people wouldn't have lunch with him. “I had to keep finding new tables,” he said.
Nobody had a good answer for that, and being around someone who kept asking it made every meal feel like a performance review.
The line that broke me is the line that most people skim over in the transcript. His words: If you do not work on an important problem you are unlikely to do important work.
That’s not motivational line. It is a rational one. You cannot make a great result from a problem that does not matter. Input restricts the output. The choice of the problem is the ceiling of the career.
The transcript has been freely available on the internet for almost 40 years. Stripe Press published the complete lectures as a book. Naval Ravikant quotes it all the time. It’s still given out to new hires at every serious engineering lab in Silicon Valley.
Most people will not run the ritual this Friday. They will be busy. They always are.
“Tell him to enter the password he knows is correct. Inform him it is incorrect. Invite him to reset it. Watch as he enters the password he believed it to be all along. Then tell him he cannot use it… because it is his current password.”
Another huge medical achievement from our very own @UHN 🇨🇦🔥
A Toronto man lived with HIV for 27 years. Then he got leukemia and that diagnosis may have just cured him of both.
His doctors found a bone marrow donor carrying CCR5-Δ32, a rare mutation in ~1% of people of European descent. HIV hijacks immune cells through the CCR5 receptor. If you don't have it, the virus has no door.
The transplant replaced his entire immune system with one HIV can't infect.
He stopped antiretroviral therapy in July 2025. As of today, HIV is undetectable by the most sensitive assays available. No viral reservoir. No immune response to HIV. Nine months clean.
He would be the 11th person in history to possibly be cured of HIV.
HIV cure is possible. We just proved it again at @UHN
Proud of the team at @UHN and @UofT !
Source: https://t.co/zH1fIfVubV
A parasite that has been eating people for 3,500 years is about to be wiped off the planet. It infected 3.5 million people in 1986. Last year, it infected 10. And I have not seen it make a single front page.
It is called Guinea worm. You drink contaminated water from a pond in a poor village. A year later, a worm up to three feet long starts coming out of your leg through a burning blister. There is no pill that stops it and no surgery that works. You wrap the worm around a stick and pull it out slowly, over days or weeks, inch by inch. If you rush, the worm breaks inside you and causes a fresh infection.
Guinea worm is ancient. Preserved worms have been pulled out of Egyptian mummies from around 1000 BCE. The Ebers Papyrus, an Egyptian medical scroll from 1550 BCE, describes pulling the worm out with a stick. For three and a half thousand years, that was the best humans could do.
Then in 1986, public health workers decided to kill the parasite off. They had no vaccine and no drug. What they had was cheap cloth water filters and a small army of volunteers willing to walk from village to village for decades.
The plan was simple. Give everyone who drinks from a pond a cloth filter to strain out the tiny water fleas that spread the parasite. Then send volunteers walking house to house, year after year, teaching people how to use the filters and keeping anyone with an emerging worm out of the water.
It worked. From 3.5 million cases a year to 10. Four were in Chad, four in Ethiopia, two in South Sudan. The other four countries where the worm used to be common, Angola, Cameroon, the Central African Republic, and Mali, had zero human cases for the second year in a row. The World Health Organization has already certified 200 countries as Guinea worm free. Six are left.
The last hurdle is dogs. Cameroon had 445 infected animals last year and Chad had 147, so a lot of the remaining work is on animals, not humans. Strays get leashed, and crews treat ponds to kill any remaining worms. The campaign keeps watching until the number hits zero.
When Guinea worm hits zero, it becomes the second human disease ever erased from the planet. The first was smallpox. It will also be the first parasite humans have ever wiped out, and the first disease ever ended without a single dose of medicine. Volunteers walked village to village with cloth filters for 40 years. Now a plague from the age of the pharaohs is about to be gone.
Welcome home Reid, Victor, Christina, and Jeremy! 🫶
The Artemis II astronauts have splashed down at 8:07pm ET (0007 UTC April 11), bringing their historic 10-day mission around the Moon to an end.
Seen few comments of ‘we got it wrong on b-blocker use post MI’
Did we get it wrong? When patients had limited culprit revasc, no bystander revasc, bigger infarcts, more arrhythmia, ongoing smoking, limited HF drugs and minimal statin plaque stabilisation, needs were different.
Some evolved primates dug some stuff out of the ground, pieced it together and are now riding the proceeds 250,000 miles away, further than any humans have ever travelled.
125 years ago we got across the oceans by steam power.
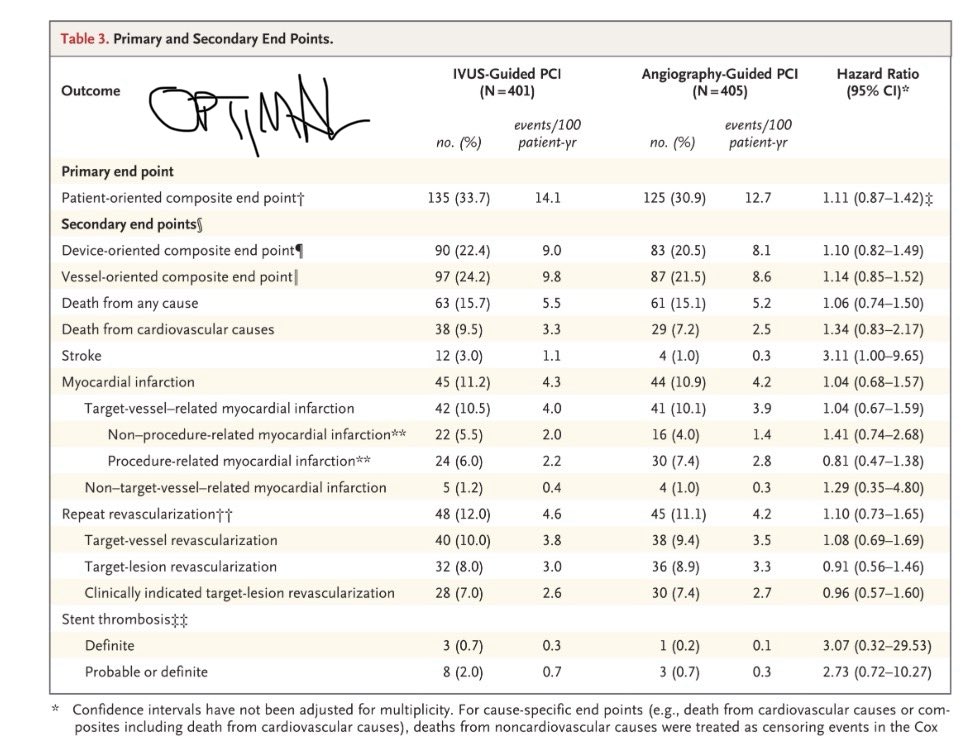
With great pleasure we report metaanalysis of 5 trials including LEMANS at 10 year follow-up in @JACCJournals. There is no difference in mortality between PCI and CABG for left main disease. In fact its identical : 23.4% vs 23.3%, HR 1.02 (0.89–1.17), RMST difference of exactly 0.0 years. Those are outcomes still with BMS and rare IVUS. Not bad! Great news for the patients. @GreggWStone@Hragy@SerruysPatrick@ZSiudak@EAPCIPresident@AHP_PAKS@uniwersytet_afm Thank you David Koeckerling and Ahmad Yosif.
https://t.co/Kk9cy8v11o
@chamath Free AI personal tutoring for kids will help disadvantaged kids more than those from wealthier backgrounds.
It seems unlikely that AI couldn’t teach any motivated kid maths.
You and @Jason talk on the pod about giving back. Surely this is the lowest of low hanging fruit.
🧵 ORBITA-CTO
Seeing a study like ORBITA-CTO being published — regardless of its results — is a beautiful thing.
This level of commitment to producing high-quality, as-unbiased-as-possible evidence in interventional cardiology should be praised. It took 4 years to randomize 50 patients. That's dedication.
Think about what this team had to do:
Noise-cancelling headphones, deep sedation, clocks removed from every room, scripted handovers, overnight admission for both arms, dual-operator procedures lasting 3+ hours — all to protect the blinding.
Bang blinding index ≈ 0. It worked.
Design: 50 patients, single-vessel CTO, confirmed ischemia + viability, J-CTO ≤3, no bystander disease.
1:1 to CTO PCI or placebo after dual-injection angiography.
All anti-anginals stopped at randomization. Daily symptom tracking via ORBITA-app for 6 months. Patient-initiated re-titration only.
Primary endpoint: angina symptom score (Bayesian ordinal MOST model, daily repeated measures).
CTO PCI vs placebo: OR 4.38 (95% CrI 1.57–12.69) Pr(Benefit) = 0.996
Driven by angina frequency: OR 4.38 (95% CrI 1.55–11.78) Pr(Benefit) = 0.997
In patient-centered terms: CTO PCI yielded ~31 additional angina-free days over 6 months vs placebo.
95% CrI: 11.1–50.7 Pr(Benefit) > 0.999
That's roughly 5 extra angina-free days per month.
SAQ domains were consistent:
Angina frequency: +10.7 (CrI 1.4–20.2)
Physical limitation: +13.5 (CrI 4.5–22.3)
Quality of life: +18.2 (CrI 5.4–30.5)
Summary score: +13.7 (CrI 4.2–23.2)
All Pr(Benefit) ≥ 0.988. CCS class also improved.
Dyspnea and EQ-5D did not separate.
Procedural quality was outstanding: 96% technical success, 92% IVUS-guided, experienced dual-operator teams.
One failed PCI case — averaging 6 angina episodes/day — was included in ITT. This biased against the PCI arm.
But the treatment effect survived it.
Why does this matter so much?
EuroCTO (Werner et al.) showed CTO PCI improved symptoms vs OMT at 1 year, sustained at 3 years. But it was open-label, with 17.5% crossover from OMT to PCI.
Without blinding, the placebo contribution to symptom relief was unknown.
ORBITA-CTO quantified it.
Both arms improved — so yes, the placebo response was substantial.
But the PCI effect was immediate and sustained. The placebo group progressively needed more anti-anginals.
Now, what ORBITA-CTO does NOT prove:
1. Benefit in multivessel disease or high-complexity CTOs (J-CTO 4–5)
2. Prognostic benefit (not designed for hard endpoints)
3. Generalizability beyond expert centers with 96% success rates
4. Benefit on dyspnea or generic quality of life
I know. N=50 is small. Credible intervals are wide. This was an expert-center study with carefully selected lesions. Noted.
But 8,631 follow-up days of daily symptom data, a Bayesian framework designed for this exact scenario, and verified blinding give it far more inferential weight than sample size alone suggests.
For years, CTO PCI skeptics had a legitimate point: no blinded evidence.
That point is now addressed. CTO PCI relieves angina beyond placebo — in well-selected patients, at experienced centers. Agreed.
Hats off to the ORBITA-CTO team for doing this the hard way. Our field is better for it. And by the way, this is not me celebrating the results. I don't do CTO. But it makes me happy to see good medical science being made.
#ORBITACTO #CardiologyX #InterventionalCardiology #ACC26 @JACCJournals
Optimal minimal stent area and impact of stent underexpansion in left main up-front 2-stent strategy
This study 📊aimed to revise the #IVUS-derived segmental MSA criteria for optimal stent expansion in patients undergoing an up-front 2-#stent strategy using the crush technique for LM #bifurcation lesions to predict the 5-year clinical outcomes.
🔗 https://t.co/gqSGqwzNYJ
Read this #EAPCI/PCR #JournalClub review ✍️ by @sbrugaletta.
Selected in @CircAHA (image source = graphical abstract)
@djc795@JAMarbach@NavinKapur4 Given that the active arm was no worse, despite ~ 47 mins of planned delay in reperfusion, perhaps it doesn’t end the hypothesis, just this mode of delivery.