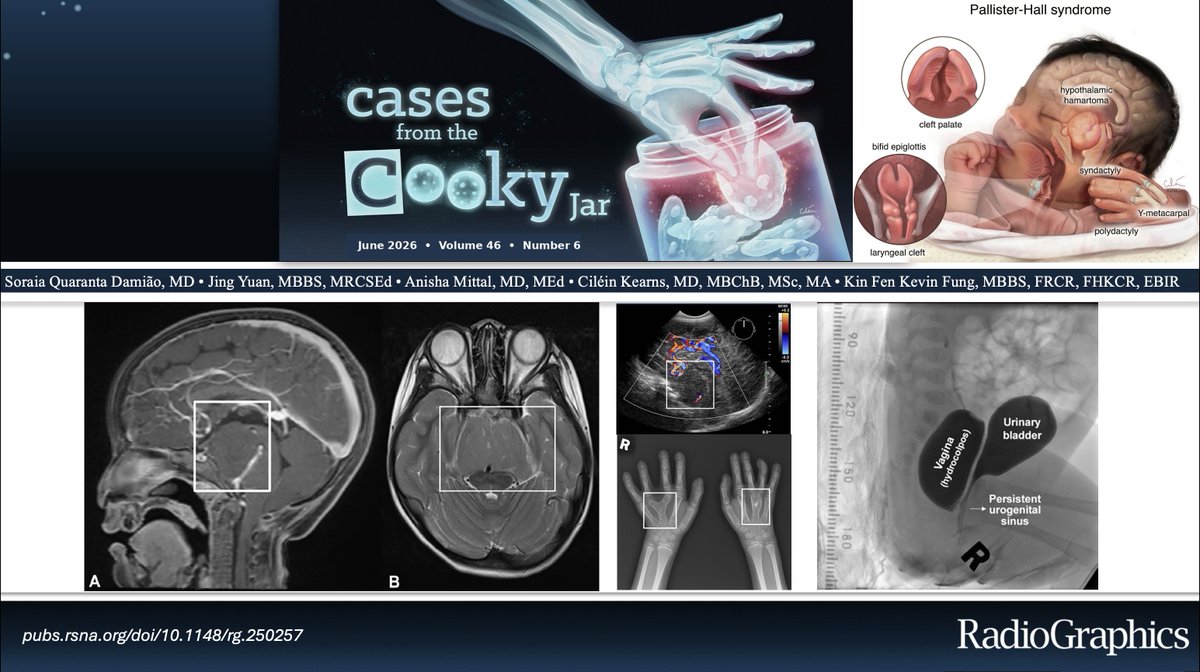
15-day-old female neonate with syndromic congenital findings.
What is the diagnosis?
Answer: 🔗https://t.co/rzMtOiHSoV
Have a companion case? Share using #CookyBites #266. We will RT the best cases!
#RGphx@cookyscan1@RadioGraphics
NEURO CASE 🔥🔥
Young Adult with progress Tremor,dystonia , rigidity and mild liver dysfunction.
Axial T2W is as shown .
What is this classic sign?
What is the diagnosis ?
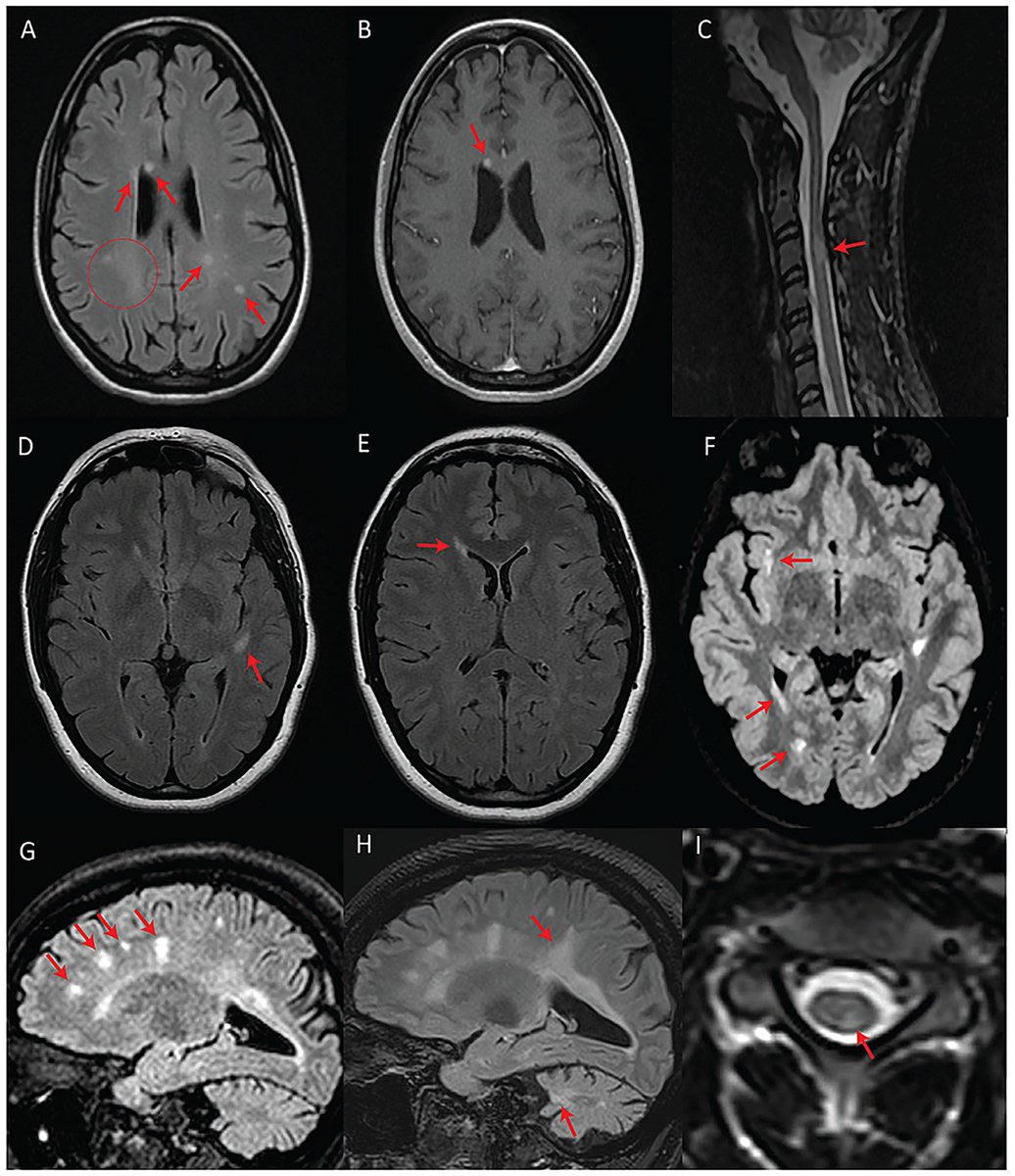
The presence of pontine stripes, superior vermian atrophy or thin corpus callosum in a patient with spastic ataxia should raise suspicion for ARSACS. It can be associated with a demyelinating neuropathy.
Link: 10.4103/aian.AIAN_16_20 @neuro_ian#ARSACS
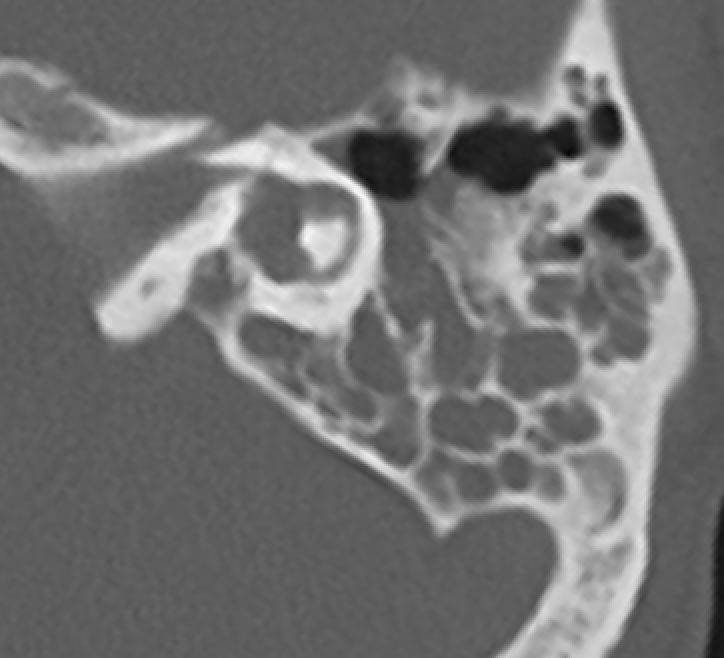
🩻Incidental incomplete partition (IP) type II on a trauma CT, with a dilated vestibule and enlarged vestibular aqueduct (the Mondini triad!). There is also a fracture through the otic capsule involving the basal turn of the cochlea.
💡In IP, you have separation of the cochlea and vestibule (cf. common cavity), normal external cochlear dimensions (cf. cochlear hypoplasia), but various defects of internal architecture.
1⃣ IP type I: the cochlea is "empty" and cystic, with no clearly formed turns.
2⃣ IP type II: confluence of the middle and apical turns, with a deficient apical modiolus and interscalar septum, but a formed basal turn. If this occurs with a dilated vestibule and an enlarged vestibular aqueduct, you have the classic Mondini malformation.
3⃣ IP type III: the cochlea has a typical "corkscrew" appearance. This is seen with POU3F4 mutations in X-linked deafness.
1/They say form follows function!
Brain MRI anatomy is best understood in terms of both form & function.
Here’s a short thread to help you to remember important functional brain anatomy--so you truly can clinically correlate!
Time for an #ISUOGEducation quiz question! 🤩
Ahead of our event Ultrasound Essentials 2026 Dr Prathima Radhakrishnan, one of the fantastic speakers we have lined up, has come up with the following quiz question.
Observe the attached video carefully and answer true/false:
A. This anomaly can always be detected in the first trimester
B. This anomaly is never associated with genetic abnormalities
C. This anomaly is easily correctable surgically
D. This pregnancy requires counselling by pediatric surgeon
Comment your answer below and come back next Friday to find out if your answer is correct! Whilst you wait for the answer why not register to Ultrasound Essentials 2026 (exclusively for low-resource settings) > https://t.co/uXYbAQaVNA
#ISUOG2025 #LoveUltrasound #UE2026 #UltrasoundEssentials
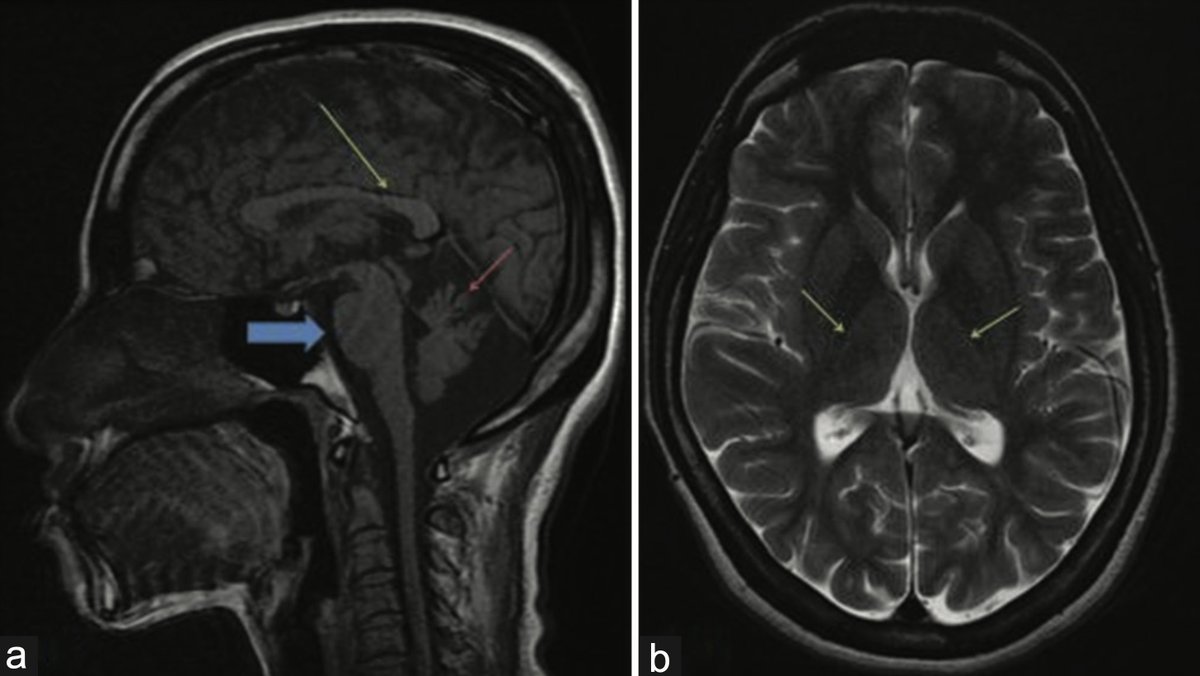
Are these MRI findings in people with multiple sclerosis? Shockingly, NO! They actually have Wolfram syndrome (WFS), a rare genetic disorder associated with pathogenic variants in WFS1 and is linked to optic atrophy, hearing loss and diabetes. https://t.co/d4CyBu23s7
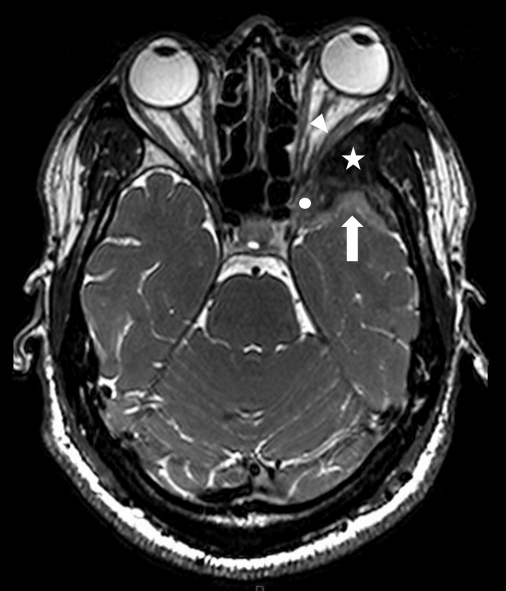
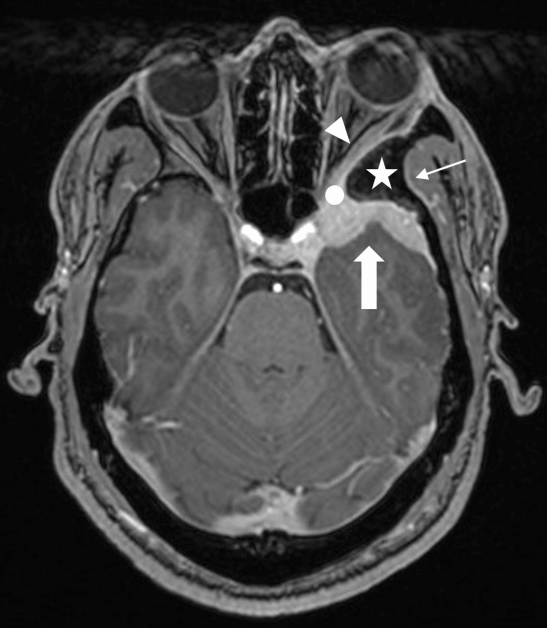
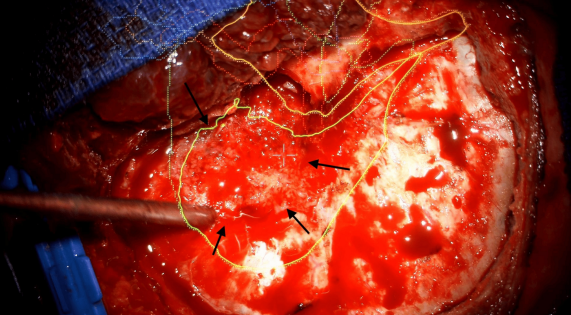
👨🚀A 34-year-old man presents with years of retro-orbital headache, mild proptosis, and new-onset blurred vision. An extra-axial spheno-orbital mass with associated bone changes leads to a presumed diagnosis, but pathology reveal something different.
What is your diagnosis?
This week's SPIN POV: Vitamin B12 deficiency is a rare and treatable cause of developmental regression in infants. Imaging typically reveals generalised atrophy. Complete reversal of the atrophy and neurological recovery is possible post-treatment with cobalamin.
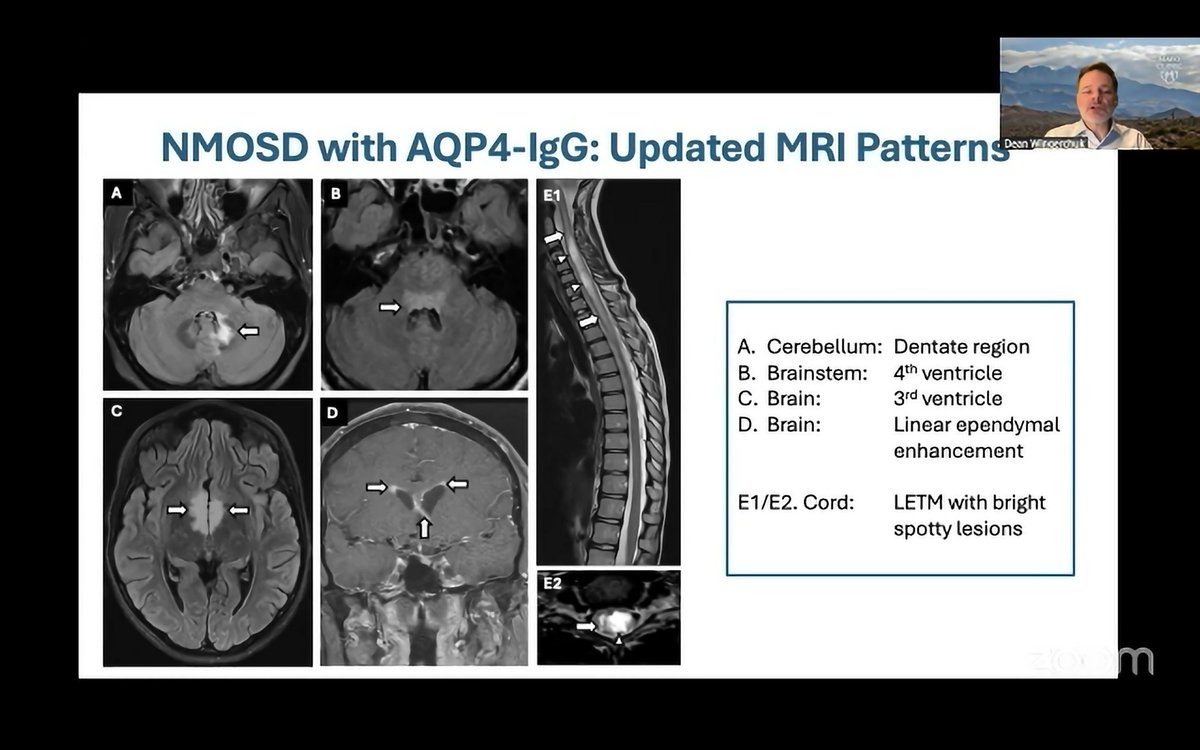
Update on IPND 2025 NMOSD diagnostic criteria presented by Dr Dean Wingerchuk via @thelimbicneuro.
Highlights:
- New clinicorad cerebellar syndrome
- Guidance regarding AQP4 testing methods: LCBA > FCBA >> ELISA
- Clarifying that double-seronegative phenocopies are not NMOSD