Radiation Oncologist | Researcher |Associate Professor @UOttawa @OttawaHospital @Cheo | Father and Husband🇨🇦 | Tweets, likes and RT are not endorsements.
Did you get your poster accepted for @caro_acro_ca Annual meeting? Don't forget to upload your poster at the CARO-Cureus Channel .
https://t.co/9sf6sIsHeo
@caroresidents
See your email from CARO for details!
@mary_hooey
Colorectal cancer rates in adults under 50 have doubled since the late 1980s.
One in five colorectal cancer diagnoses now occurs in someone under 55, up from one in ten in 1995.
A new study highlights the most concrete factor responsible for this trend.
Using DNA methylation profiles as molecular records of lifetime exposure, the authors compared cancer patients under 50 with patients over 70 and identified the herbicide picloram as a significant new risk factor.
There are converging lines of evidence.
The picloram exposure signature was significantly elevated in early-onset tumor tissue and replicated across nine independent patient cohorts. Across 21 years of US county-level data spanning seven states, higher picloram use tracked higher early-onset CRC incidence, and the signal held after adjusting for income, education, and the use of other pesticides.
Picloram associated tumors also showed a distinct molecular profile, with APC mutations at 74% versus 90% in low-exposure tumors, suggesting these cancers follow a different biological pathway than classical CRC.
Picloram entered commercial use in 1964. Patients now diagnosed in their 70s were already adults before meaningful exposure was possible. Patients now diagnosed in their 30s and 40s were exposed across childhood and adolescence, the developmental windows when epigenetic programming is most plastic.
This study delivers the first triangulation of molecular, ecological, and temporal evidence pointing at a specific environmental driver of one of the steepest cancer trends in modern epidemiology.
Colonoscopy vs FIT vs no screening 🩺
What do we actually gain in the first 5 years? 🧠
SCREESCO RCT (Nature Medicine 2026) finally includes a true usual-care control arm 📊
👥 278k screening-naive adults
🎂 Age 60 years
⏱️ Median follow-up 4.8 years
🧪 Arms
🔵 Once-only colonoscopy
🟢 FIT ×2 (two-stool, low cutoff)
⚪ No screening
📊 Key results
❌ Overall CRC incidence: no reduction
⬆️ Stage I–II CRC
• Colonoscopy IRR 1.38
• FIT IRR 1.19
⬇️ Stage III–IV CRC
• Colonoscopy IRR 0.86
• FIT IRR 0.71
⚠️ Harms
🩸 Slight ↑ GI/CV events in year 1
🧬 Serious colonoscopy AEs ~0.2%
⚖️ No excess all-cause mortality
🧠 Clinical takeaway
Screening delivers an early stage shift, not early incidence reduction 🎯
Mortality data still awaited ⏳
📖 Full paper in comment ⬇️
#OncoTwitter #GIOncology #ColorectalCancer @esmo_open@OncoAlert@ASCO
Treatment for Brain Metastases With Stereotactic Radiation vs Hippocampal-Avoidance Whole Brain Radiation
A Randomized Clinical Trial
https://t.co/ViQTBACbME
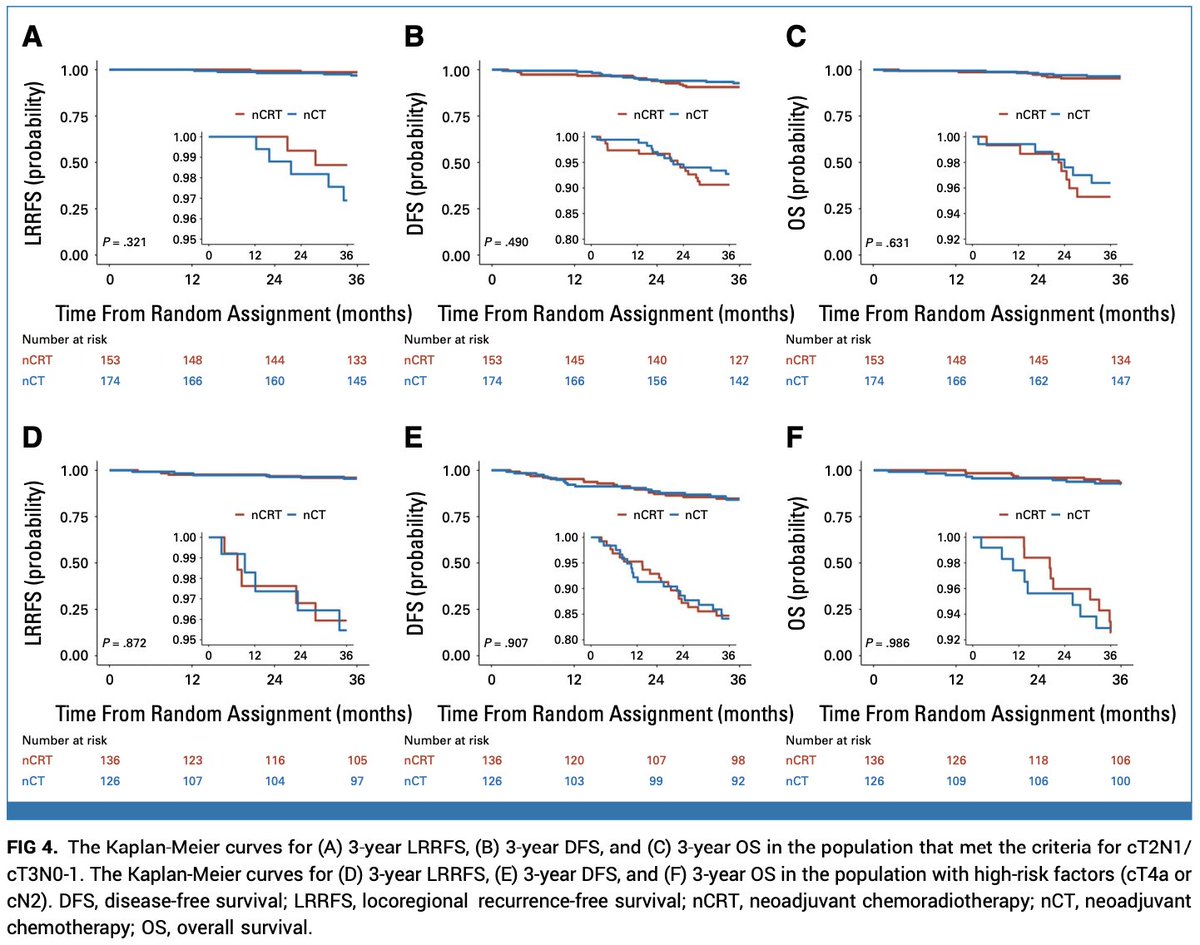
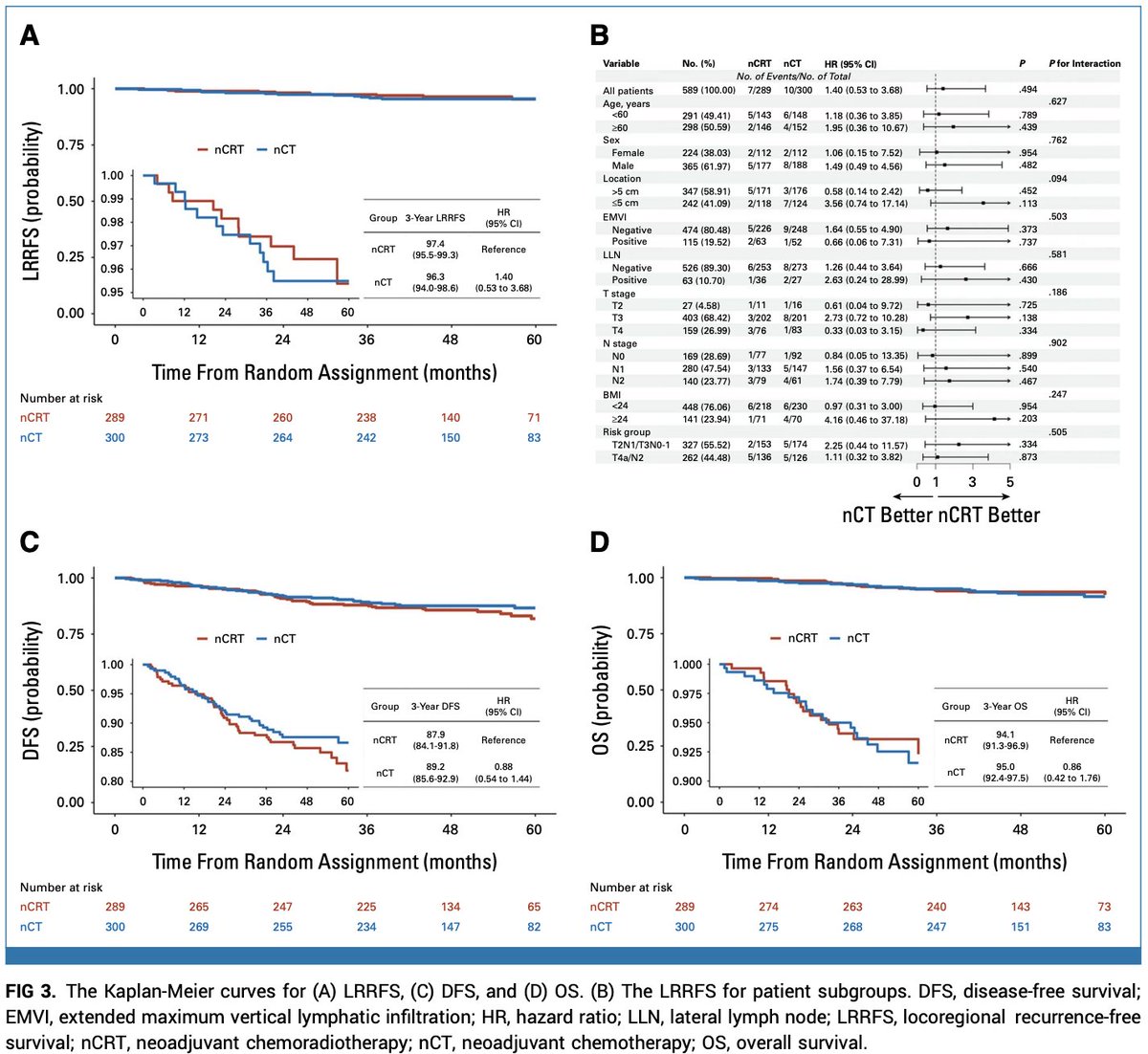
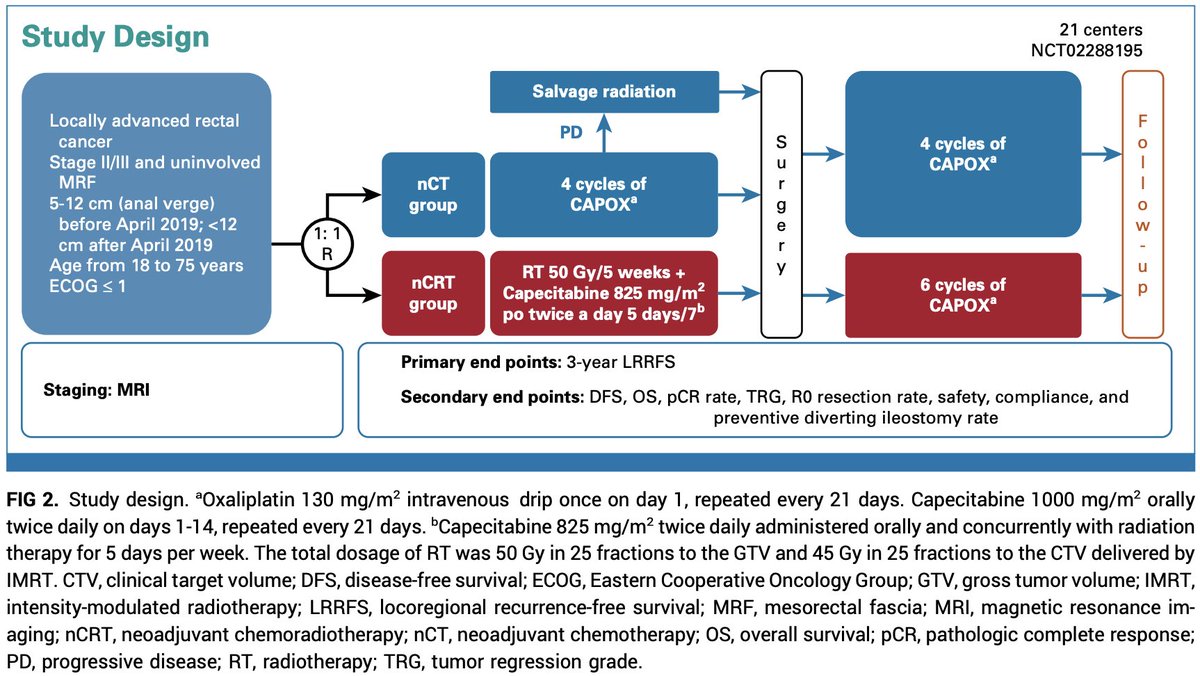
Can we safely omit radiation in selected locally advanced rectal cancer?
The CONVERT trial randomized mesorectal fascia–negative patients to neoadjuvant CAPOX vs ChTR
3-year local control: 96.3% vs 97.4%.
Non-inferiority was not formally met ⚠️
DFS/OS were similar between arms.
Long-term toxicity favored ChT alone.
Careful selection may allow de-escalation w/o compromising outcomes.
https://t.co/YW0Zh3ghey @JCO_ASCO@OncoAlert
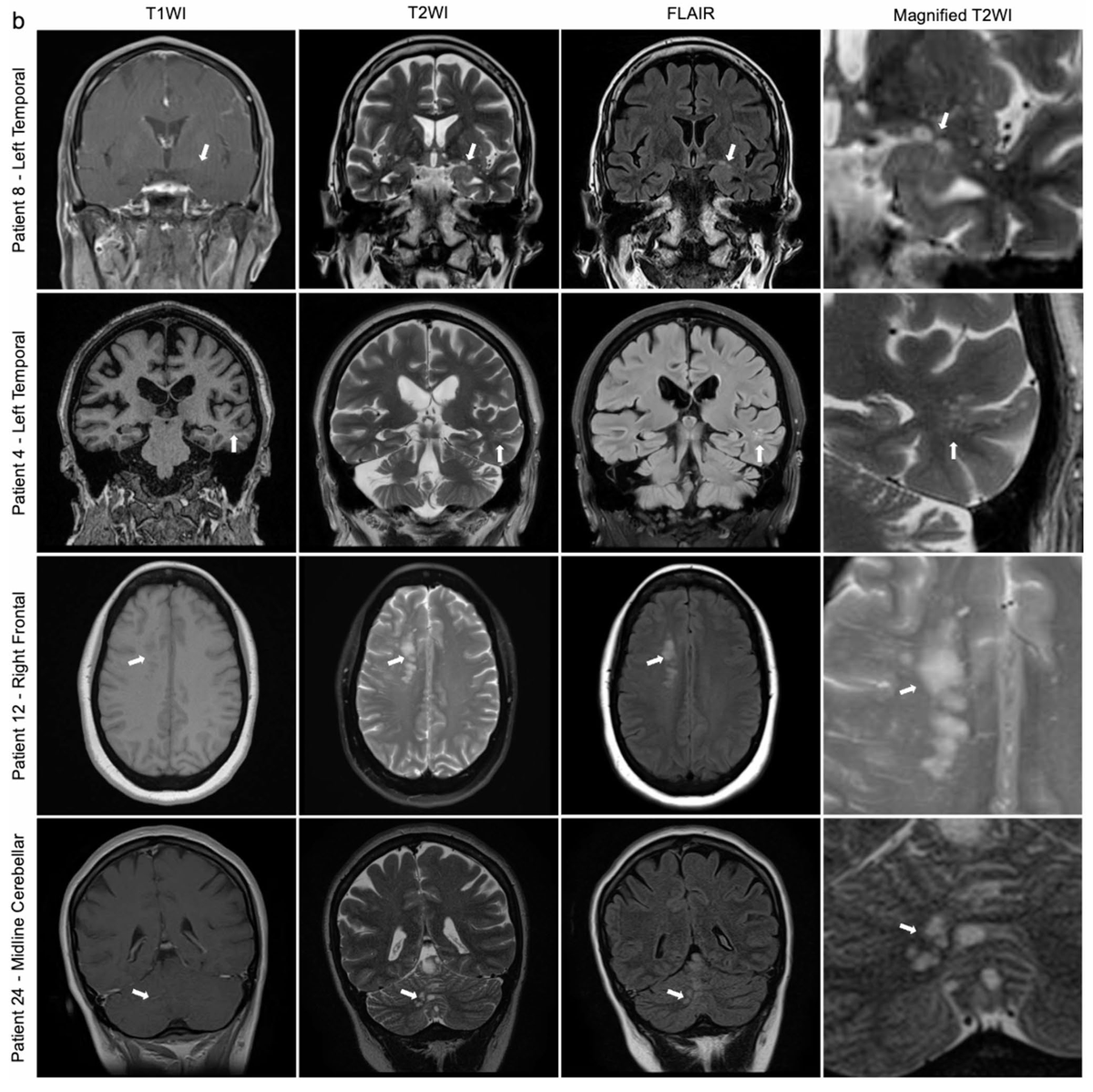
Multinodular & vacuolating neuronal tumor (MVNT) is a rare, benign entity often found incidentally, w/ characteristic MR findings: Subcortical, FLAIR-hyperintense, nonenhancing nodules. In our cohort, most did well w/ conservative management.
@JordinaRT_md
https://t.co/ZYm7zjQP4R
New research shows that smarter brains burn less glucose to solve the same problems—fewer neurons firing, faster adaptation, cleaner circuitry.
In simple terms: higher intelligence = lower energy cost.
Another reason to put the phone down and let your brain do its thing. 😉
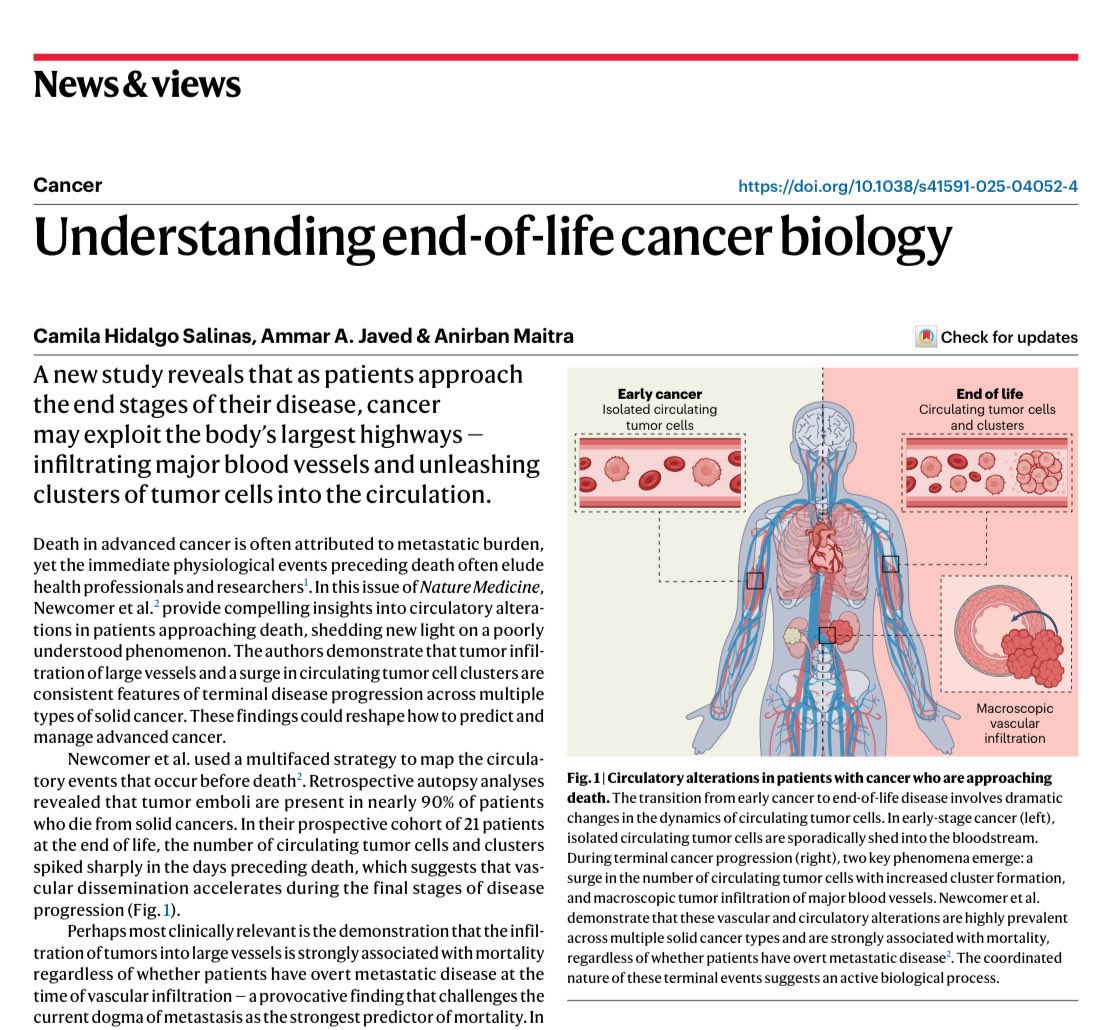
🆕 @NatureMedicine: end-of-life cancer biology. As patients near death, tumors infiltrate major vessels and release surges of CTC/clusters (across multiple solid tumors…)
https://t.co/eStsKibkb8
📌 Vascular invasion strongly associates with mortality, even without overt M1
When cancer takes the “highways” at the end…maybe it’s time we rethink the map itself 🛣️
@OncoAlert #OncoAlertAF @OncoReporte@myESMO@_SEOM@realbowtiedoc@Nature@SuyogCancer
New in JAMA Oncology: Over 231,000 adults followed for 32 years.
🏃♂️Consistent mod physical activity (~17 MET-hrs/week = ~5 hrs brisk walking or ~2 hrs running) led to major reductions in digestive system cancer risk.
🔥 More exercise (~39 MET-hrs/week) didn’t bring extra benefit.
Consistent moderate physical activity—about 17 metabolic equivalent task-hours/week over 3 decades—was associated with optimally reduced risk of digestive system cancers in a large cohort study. https://t.co/TWvGrT0mwG
Back at #WFNOS2025#SNO2025#Hawaii#aloha
Excited about the scientific program and seeing all my wonderful colleagues!
If you are here do give a shout! https://t.co/Jn5UjGS75F…
Time is an under-recognised social determinant of brain health.
In The Lancet Healthy Longevity, authors call for temporal justice through research and policies that recognise time as both a resource and a site of inequity in ageing and dementia: https://t.co/S3AVviAnZY
Radiation lymphoma studies that are published in rad onc journals are better cited, despite lower impact factor. Lymphoma studies reporting on radiation negative clinical outcomes are more likely to be published in non-rad onc and higher impact factor journals, and by non-rad onc authors: https://t.co/MGciPMCmIg
Reirradiation (reRT) is reshaping cancer care—offering hope for recurrent tumors w/ advanced precision techniques like IMRT & SBRT. Multidisciplinary care, imaging, and innovation are key.
#OpenAccess review by Andratschke et al:
https://t.co/T41ik4rEsa
@OncoAlert#RadOnc
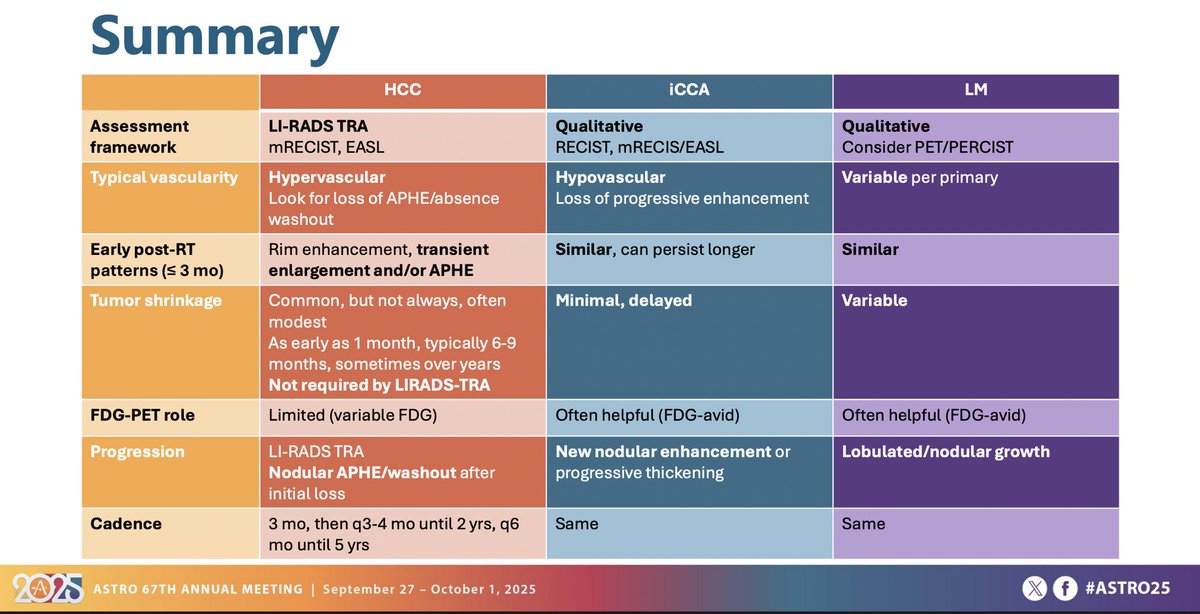
This was a great talk by Jim Apisarnthanarax on response assessment for liver tumors.
Summary slide here on imaging characteristics at diagnosis & post RT for HCC vs. cholangio vs. liver mets is 💯.
#ASTRO25