This review outlines an approach for the diagnosis and treatment of postural tachycardia syndrome (#POTS) and related dysautonomia in a general practice setting: https://t.co/MGNRkWZrEn
Voy escribir algo revolucionario, espero no herir sensibilidades.
Creo que los colegios e institutos de nuestro país deberían tener obligatoriamente aire acondicionado en las aulas.
Un saludo.
Inflammatory myopathies are typically associated with a myositis-specific autoantibody that determines the diagnosis and prognosis. Myositis subgroups have distinct pathomechanisms that now allow for targeted therapies.
Learn more in the Review Article “Inflammatory Myopathies” by Yves Allenbach, MD, PhD, and Olivier Benveniste, MD, PhD: https://t.co/ZeCKdNe87v
👨🦼 En el marco del Día de las Enfermedades Raras, hoy nos centramos en la ELA, una enfermedad que afecta a las células nerviosas del sistema motor. En Asturias hay más de un centenar de pacientes diagnosticados y uno de ellos es Roberto Palacios.
#PanoramaRegional
📺 La miastenia gravis es una enfermedad poco frecuente que se da cuando las órdenes nerviosas no llegan a los músculos, lo que se traduce en dificultades para respirar, hablar o tragar. En Asturias, afecta a casi 300 personas.
#PanoramaRegional
Do you know all the updates on restless legs syndrome (RLS) 2026? Are we getting the diagnosis right and the treatment smarter. Spoiler alert: ‘Gabapentinoids’ now take center stage. What does RLS mean? RLS or restless legs syndrome is a movement disorder marked by an urge to move the legs that worsens at rest, improves w/ movement and is strongest in the evening or night. Winkelman and Wipper describe in a just dropped paper in JAMA what is new in understanding, diagnosing and treating RLS in 2026.
Key points:
- RLS affects about 3 percent of adults and frequently disrupts sleep mood and quality of life.
- Abnormal brain iron handling, genetic risk and dopamine system changes appear central to RLS biology.
- Gabapentinoids are now first line therapy, while dopamine agonists are no longer preferred due to augmentation risk.
My take: RLS is frequently misdiagnosed or treated in ways that make symptoms worse over time. This review provides a clear practical reset. The message is simple, but powerful. Get the diagnosis right, check iron thoughtfully and treat in a way that protects folks long-term, rather than chasing short term relief. In our MDS Aspen course, the experts have been chirping for 3-5 years to shift away from dopamine agonists and to ‘gabapentinoids.’ The time has come! Here are 5 points that resonated w/ me:
1- RLS is a clinical diagnosis and sleep studies are not required for most folks.
2- Iron deficiency in the brain can exist even when blood iron looks normal.
3- Gabapentinoids help many folks and avoid the long term risks seen w/ dopamine agonist and dopaminergic drugs.
4- Augmentation is a real and a frequently underrecognized complication of dopamine agonists.
5- Thoughtful stepwise care by health care providers can markedly improve sleep and daily function for folks living w/ RLS.
https://t.co/lFXaqWFt1w @ParkinsonDotOrg@FixelInstitute@movedisorder #RLS @JAMA_current@JAMANeuro
Hoy lanzamos un nuevo Manual de Práctica Clínica en #Cefaleas, que recoge toda la actualidad del cocimiento científico sobre cefaleas y neuralgias craneofaciales, en forma de recomendaciones diagnóstico-terapéuticas.
Se puede consultar online en: https://t.co/TyepbGiuY9
Estimado Alberto: Los médicos no pedimos normas que invadan competencias autonómicas ni leyes “de carta a los Reyes Magos”. Pedimos que el Estado ejercite plenamente las competencias que sí tiene, y que hoy no está ejerciendo.
El Estatuto Marco es una ley básica estatal (art. 149.1.18 CE). Eso significa que puede y debe fijar:
– límites máximos de jornada y descanso,
– un marco básico de guardias,
– criterios comunes de salud laboral,
– principios de carrera profesional y jubilación,
– y garantías mínimas para la seguridad del paciente.
Todo ello sin gestionar plantillas ni presupuestos autonómicos, que es donde empieza y termina la competencia de las CCAA.
Decir que el margen estatal es “muy estrecho” no es exacto:
el Estado ya regula jornada, incompatibilidades, formación MIR, homologaciones, evaluación, bases del empleo público y derechos laborales básicos en sanidad desde hace décadas, y el Tribunal Constitucional lo ha avalado reiteradamente.
Lo que pedimos los médicos no es centralismo, sino bases claras y seguras que eviten precisamente la litigiosidad y la desigualdad territorial que hoy existe.
Que una norma pueda ser recurrida no puede convertirse en excusa para no legislar, porque entonces ninguna ley básica social sería posible. El riesgo de control judicial forma parte del Estado de Derecho; la inacción también tiene consecuencias, y hoy las estamos viendo en forma de agotamiento profesional, fuga de talento y deterioro asistencial.
Por último: cuando miles de médicos paran durante varios días no están pidiendo milagros.
Están diciendo que el marco actual y el propuesto no protege ni a los profesionales ni a los pacientes.
Eso merece algo más que resignación jurídica. Merece una reforma ambiciosa, bien hecha y dentro de la Constitución.
In this wonderfully written review, Coleman et al provide a comprehensive update on current understanding of idiopathic intracranial hypertension pathophysiology. This one is a must-read! 🔎 👇
https://t.co/FpS6cjkTSa
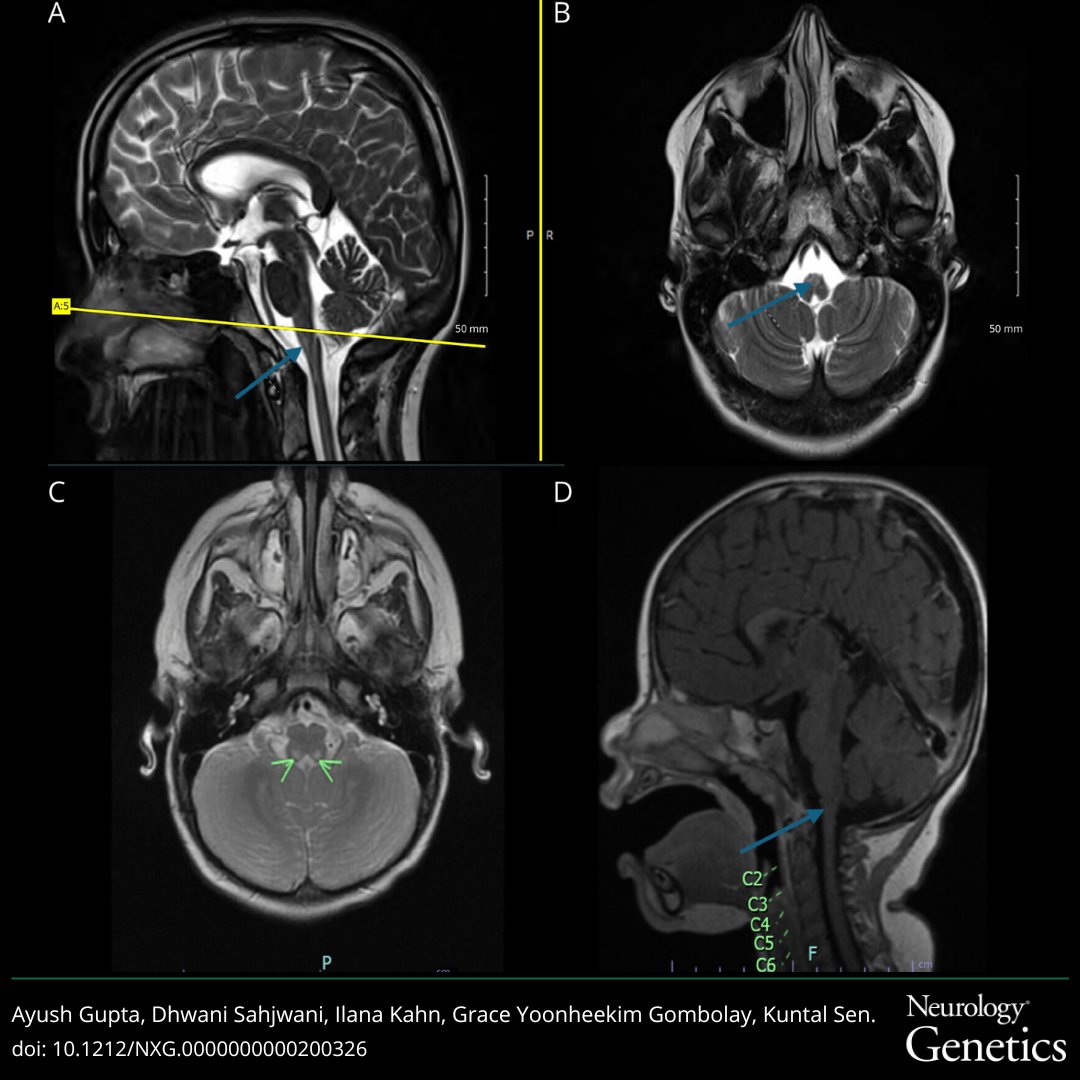
In this study a considerable proportion of patients diagnosed with seronegative #MyastheniaGravis had an underlying hereditary etiology. Offering genetic testing to seronegative patients with myasthenic syndromes may have profound therapeutic implications: https://t.co/rVQUzLcaNP
This case highlights the differential diagnosis of autonomic failure, emphasizing the role of specific clinical, laboratory, and imaging cues in guiding clinical reasoning: https://t.co/8t4ePSVIEy
#NeurologyRF#NeuroTwitter
Non-neuromuscular physicians, the severity of a distal symmetric polyneuropathy on nerve conduction studies is not determined by the conduction results in the lower limbs. Regardless of age, if someone has normal upper limb conductions, they do not have a severe polyneuropathy.
Desde el Grupo de Ictus de la Sociedad Neurológica Asturiana 🧠hemos abierto un canal de YouTube en el que compartiremos contenido de nuestras actividades formativas. 🧵⬇️⬇️