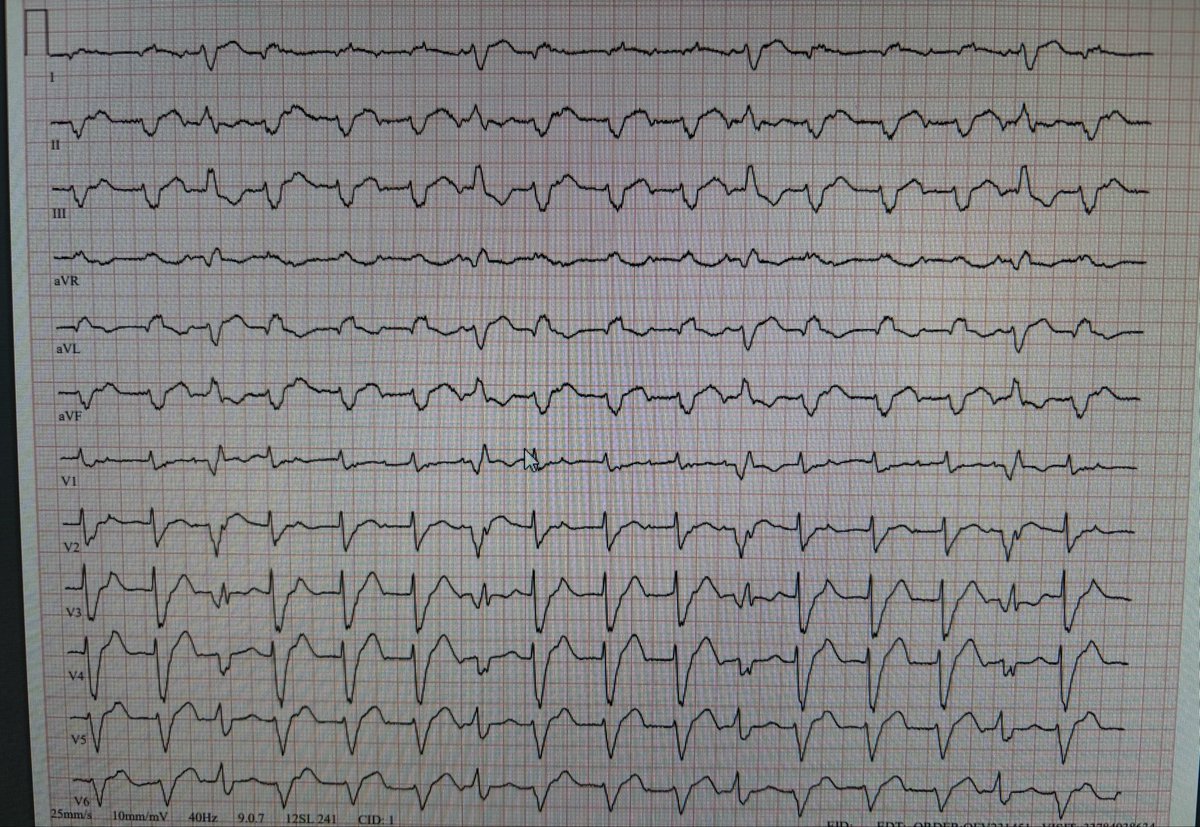
🟡 VT with 1:1 VA conduction 🟡
You have no AV dissociation but one to one association from the retrograde conduction in this ventricular tachycardia.
🧵 & 🔗
@Frances98392343@lila_enis@Frances98392343@lila_enis
Here, a narrow QRS tachycardia is evolving into a wide QRS tachycardia. Given that this patient initially had frequent PACs and atrial tachycardia, could there be aberration or pre-excitation involved?
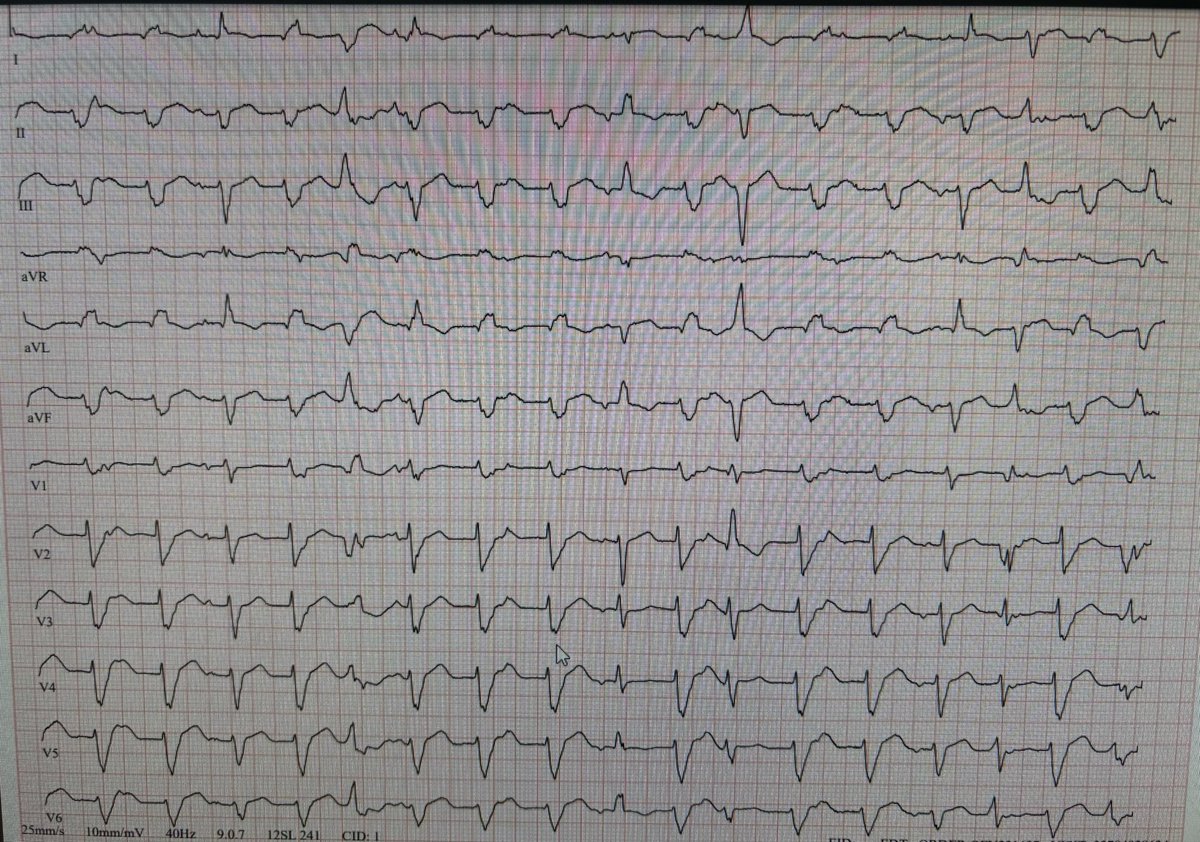
39F with a history of myocarditis, cardiac MRI showing 49% EF and LGE+. What could a wide QRS tachycardia with negative concordance during an exercise stress test indicate?
@Frances98392343@lila_enis You're right. They say, 'When you hear hoofbeats, think horses, not zebras,' but they also say, 'All that glitters is not gold.'
https://t.co/mEiuruqeEu
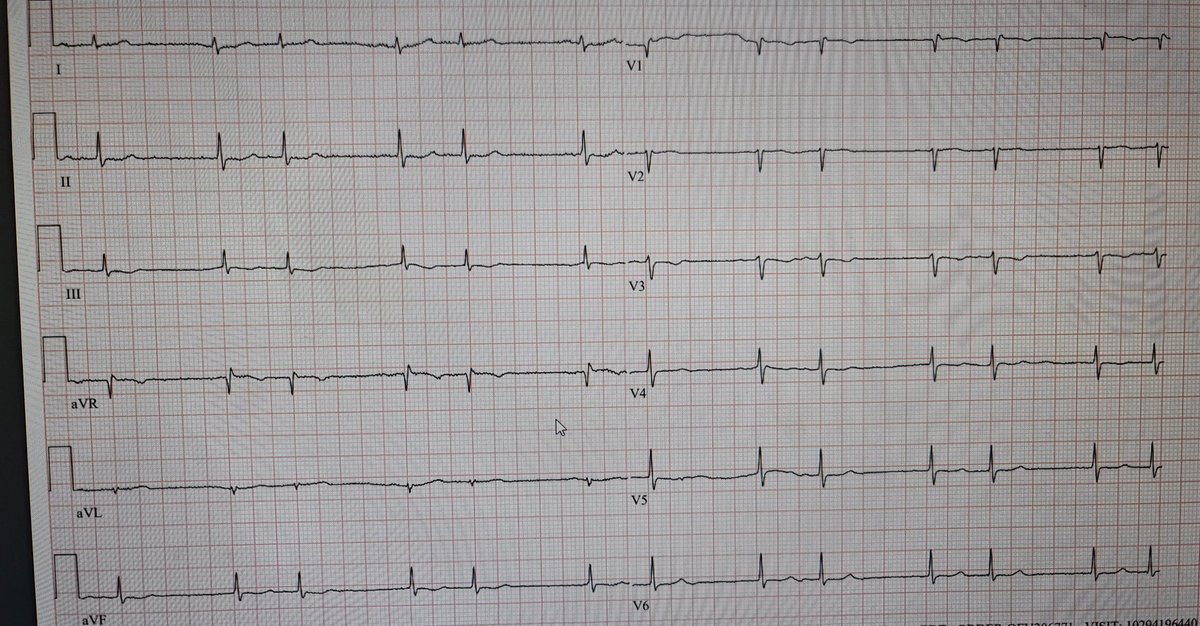
@EleanorRigby18@Frances98392343 Could you look at V1. Before the 5th, 6th, and 7th QRS complexes, the PR interval is progressively shortening. The same pattern is also present before 9-10-11 and 13-14-15, meaning there seems to be a regular relationship. I am not sure if this is an AV dissociation.
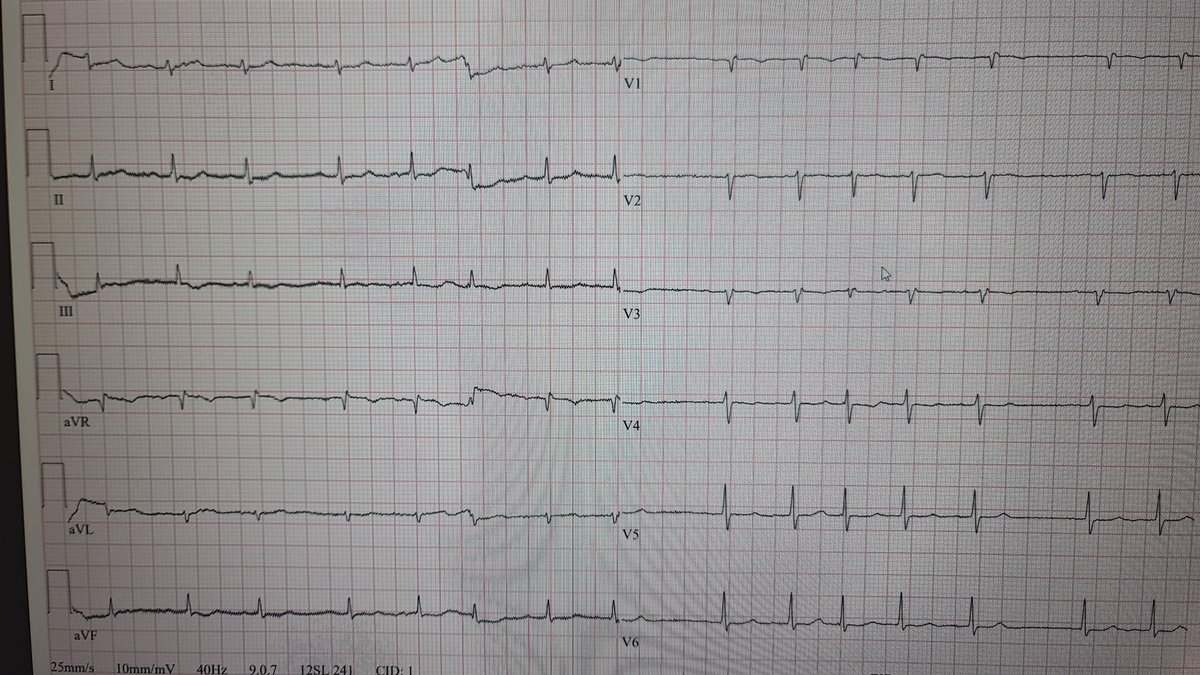
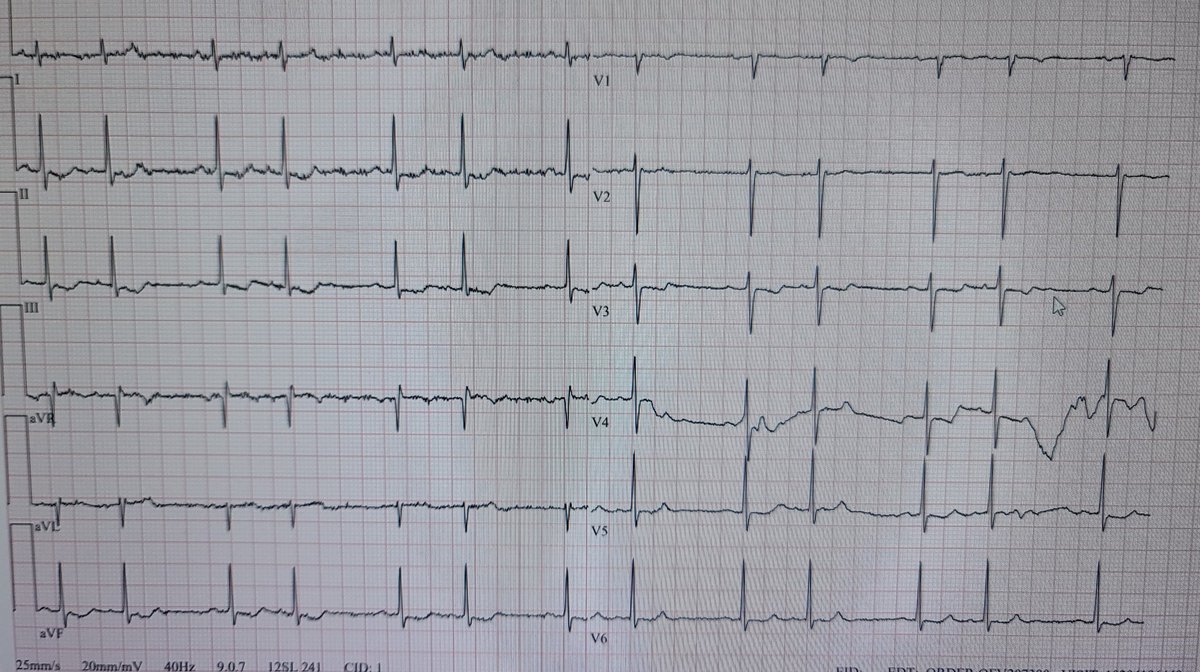
20 y/o female has limb-girdle muscular dystrophy and is being evaluated for suspected stroke/TIA; these two ECGs belong to that patient. What do you think the rhythm is?
I am not sure, I'm just speculating. The right-sided ECG may represent a fever-induced Brugada pattern Type 1. Lead V3 resembles a Brugada pattern Type 2.
Fever exacerbates sodium channel dysfunction, destabilizing cardiac membrane potential and increasing the risk of early afterdepolarizations and re-entrant circuits that trigger VF. This pathophysiological cascade underscores the importance of aggressive fever management with antipyretics to prevent severe arrhythmic events.
@Frances98392343 There are polymorphic PVCs, and the tachycardia on the left has the same morphology as one of those PVCs. There’s also a capture beat. Yes, I agree with you — this is VT. Could the right side possibly represent an atrial run or tachycardia?
@Frances98392343 I can’t clearly identify regular atrial activity, and the P waves I do see raise a suspicion of intermittent WPW in my mind. What is your interpretation of the second ECG?
Although Takotsubo syndrome is often perceived as a postmenopausal female disease, it can also occur in men, particularly those exposed to physical stress. In a patient with such an ECG, coronary angiography should, of course, be performed; personally, if the results are normal, I prefer to proceed with ventriculography.
DD: MINOCA and myocarditis.